
Abstract
In the past two to three decades health behavior scientists have increasingly emphasized affect-related concepts (including, but not limited to emotion) in their attempts to understand and facilitate change in important health behaviors, such as smoking, eating, physical activity, substance abuse, and sex. This article provides a narrative review of this burgeoning literature, including relevant theory and research on affective response (e.g., hedonic response to eating and drug use), incidental affect (e.g., work-related stress as a determinant of alcohol use), affect processing (e.g., anticipated regret for illicit sex or skipping an exercise session), and affectively charged motivation (e.g., cigarette craving). An integrative dual-processing framework is presented that suggests pathways through which affect-related concepts may interrelate to influence health behavior.
Keywords
Health-related behaviors, such as smoking, eating, physical inactivity, substance abuse, and sex, account for a significant proportion of chronic disease and death in the US and worldwide (Danaei et al., 2009; Mokdad, Marks, Stroup, & Gerberding, 2004; World Health Organization, 2005, 2011). Understanding why people engage (or fail to engage) in health behaviors and identifying strategies to help people change their health behaviors are central goals for health behavior science—a subfield of public health.
The most often used theories in health behavior science (see Glanz & Bishop, 2010) emphasize conscious cognitive beliefs as determinants of health behavior (Ajzen, 1991; Bandura, 1986; Fishbein, 1979; Prochaska & DiClemente, 1983; Rosenstock, 1966) consistent with the cognitive paradigm in psychology that came into favor in the 1950s. However, in the past two to three decades there has been an explosion of theory and research on affect-related concepts (including, but not limited to emotion) as determinants of health behavior. The present article provides a narrative review of this burgeoning literature. Affect-related concepts are divided into four categories based on their relation to the target health behavior (see Figure 1):(a) affective response to the target behavior; (b) incidental affect: affect that is not caused by the target behavior but may influence the target behavior (see Bodenhausen, 1993); (c) affect processing: cognitive processing of previous or anticipated affective responses to the target behavior, including anticipated affective response, affective attitude, affective association, and implicit attitude; and (d) affectively charged motivation: motivational states that include an affective component, including craving, desire, fear, and intrinsic motivation. Following the review, an integrative dual-processing framework is presented that suggests possible pathways through which affect-related concepts may interrelate to influence health behavior.

Affect-related concepts commonly used in health behavior research.
Affective Response
According to multiple seminal and contemporary theories of human behavior, positive affective responses to a target behavior (i.e., positive shifts in hedonic valence; Russell, 1980) are posited to lead to more frequent performance of the behavior, whereas negative affective responses lead to less frequent behavior (e.g., Cabanac, 1992; Darwin, 1872/1998; James, 1894/1994; Kahneman, Wakker, & Sarin, 1997). This hedonic principle is considered an important mechanism of reinforcement in theories of addiction and eating behavior. Positive reinforcement theories emphasize shifts from neutral to positive hedonic valence in response to substance use or eating (Berridge, 2000; Cota, Tschop, Horvath, & Levine, 2006; Ely, Winter, & Lowe, 2013; Lutter & Nestler, 2009; Nasser, 2001; Nathan & Bullmore, 2009; van den Bos & de Ridder, 2006), whereas negative reinforcement theories emphasize the relief of negative affective states, such as work-related stress or drug withdrawal (Baker, Piper, McCarthy, Majeskie, & Fiore, 2004; Koob, 2013; Parylak, Koob, & Zorrilla, 2011).
Research among humans and nonhuman animals generally supports hedonic theories of drug use (for reviews see Cheetham, Allen, Yucel, & Lubman, 2010; de Wit & Pham, 2010; de Wit & Phillips, 2012; McCarthy, Curtin, Piper, & Baker, 2010) and eating (for reviews see Lowe & Butryn, 2007; Yeomans, 2008). Likewise, studies have shown that more positive (or less negative) hedonic responses are associated with greater likelihood of smoking relapse (Barrett, Boileau, Okker, Pihl, & Dagher, 2004; Forestell & Mennella, 2005; Shiffman, Ferguson, & Gwaltney, 2006; Thuerauf, Kaegler, Renner, Barocka, & Kobal, 2000), initiation and continuation of exercise programs (Kwan & Bryan, 2010; Schneider, Dunn, & Cooper, 2009; Williams, Dunsiger, et al., 2008; Williams, Dunsiger, Jennings, & Marcus, 2012), and greater alcohol use (Newlin & Renton, 2010; Newlin & Thomson, 1990).
In contrast to the immense literature emphasizing positive versus negative shifts in hedonic valence, few studies have focused on specific emotional states in response to health behavior (Desteno, Gross, & Kubzansky, 2013). One exception is research guided by Rothman’s (2000) hypothesis that satisfaction with the outcomes of behavior change is a key determinant of health behavior maintenance—an idea that has been supported in the context of smoking cessation (Baldwin et al., 2006; Hertel et al., 2008), exercise (Williams, Lewis, et al., 2008), and weight loss (Finch et al., 2005). Additionally, a small number of studies have shown that, contrary to the hedonic principle, guilt or regret 1 in response to a lapse in self-control may lead to subsequent self-control failures in the context of smoking (Baer, Kamarck, Lichtenstein, & Ransom, 1989), alcohol use (Muraven, Collins, Morsheimer, Shiffman, & Paty, 2005), and multiple health behaviors (Hofmann & Fisher, 2012).
Incidental Affect
Negative Incidental Affect
Much of the research on negative incidental affect as a determinant of health behavior has been driven by affect regulation theories, including general theories of behavior (Morris & Reilly, 1987; Tice, Bratslavsky, & Baumeister, 2001; Wegener & Petty, 1994) and domain-specific theories of eating (Greeno & Wing, 1994; Polivy & Herman, 1976), smoking (Brandon, 1994), and alcohol and drug abuse (Cox & Klinger, 1988; Khantzian, 1985). Common to all of these theories is the notion that negative incidental affect often leads to maladaptive behavior because the subject anticipates that the behavior will alleviate their negative affective state. 2 Contrary to affect regulation theory, some researchers have argued that negative incidental affect may, in certain situations, lead to decreased likelihood of performing the target behavior (Andrade, 2005; Kassel, Stroud, & Paronis, 2003; Macht, 2008). This formulation is consistent with broader theories of affect congruency (Bower, 1981; Forgas, 1995; Schwarz & Clore, 1983). Predictions from affect congruency and affect regulation theories diverge when the target behavior is expected to result in a shift in affective valence that is opposite from the incidental affective valence. For example, according to affect congruency theories negative incidental affect should lead to decreased likelihood of chocolate eating; however, affect regulation theory would predict increased likelihood of chocolate eating if affective response to the chocolate is expected to be positive.
Numerous studies have shown that negative incidental affective states, including diffuse negative moods (e.g., depressed mood, life stress) or acute negative affect (e.g., social anxiety, shame) in clinical (e.g., depressive or anxiety disorders) and normal populations, are predictive of increases in maladaptive but potentially affect-enhancing behaviors, such as eating, smoking, and alcohol and drug use (for reviews see Carrigan & Randall, 2003; Cheetham et al., 2010; Gibson, 2012; Haedt-Matt & Keel, 2011; Kassel et al., 2003). Some studies have, however, failed to find this relationship for certain affect–behavior combinations, such as depression and cocaine relapse (see Bradizza, Stasiewicz, & Paas, 2006), or certain population–behavior combinations, such as sexual risk behavior among HIV positive individuals (Crepaz & Marks, 2001). Additionally, a review of studies employing ecological momentary assessment showed that while binge eating is often preceded by negative incidental affect, it does not subsequently decrease negative affect as predicted by affect regulation theory (Haedt-Matt & Keel, 2011).
Positive Incidental Affect
In multiple theories, positive affect is posited to lead to increases in optimism, risk aversion, or active engagement with positive goals, which in turn results in favorable outcomes, such as higher life satisfaction, strong social relationships, financial success, and better global health (Chesney et al., 2005; Fredrickson, Mancuso, Branigan, & Tugade, 2000; Isen & Patrick, 1983; Lyubomirsky, 2001). According to these theories, positive incidental affect should increase the likelihood and/or frequency of healthy behaviors, such as higher levels of physical activity and lower levels of cigarette and alcohol use. Conversely, Cyders and Smith (2008) have recently argued that extreme positive affect can—along with extreme negative affect—lead to increased likelihood or frequency of risky or addictive behaviors (see also Whiteside & Lynam, 2001).
Relative to the robust literature on negative incidental affect, less research has been conducted on positive incidental affect as a determinant of health behavior. However, a review of research on the role of positive incidental affect across a range of behavioral domains suggests that positive incidental affect tends to increase rates of positive health behaviors such as physical activity, and reduce negative health behaviors such as smoking (Lyubomirsky, King, & Diener, 2005).
Affect Processing
Anticipated Affective Response
The concept of anticipated affective response is consistent with the broader notion of outcome expectancy in social learning theory (Bandura, 1977; Rotter, 1954), the health belief model (Rosenstock, 1966), social cognitive theory (Bandura, 1986), and the theories of reasoned action and planned behavior (Ajzen, 1991; Fishbein, 1979). In addition to these broad-based expectancy theories, greater focus on anticipated affective response can be found in response expectancy theory (Kirsch, 1985), decision affect theory (Mellers, Schwartz, Ho, & Ritov, 1997), and research on affective forecasting (Gilbert & Wilson, 2007; Kahneman, Krueger, Schkade, Schwarz, & Stone, 2006; Loewenstein & Schkade, 1999).
In the context of health behavior, research has shown that anticipated positive affective responses, such as enjoyment or satisfaction, increase likelihood of exercise behavior, whereas anticipated displeasure decreases likelihood of exercise (for reviews see Nasuti & Rhodes, 2013; Rhodes, Fiala, & Conner, 2009). Likewise, anticipated regret for performing maladaptive behaviors (e.g., smoking) often decreases likelihood of the behavior, while anticipated regret for not performing adaptive behaviors (e.g., condom use, exercise) increases likelihood of the behavior (for reviews see Rivis, Sheeran, & Armitage, 2009; Sandberg & Conner, 2008). Thus, unlike experienced regret, which can lead to increases in maladaptive behaviors (see previous lines), anticipated regret may lead to decreases in maladaptive health behaviors, consistent with the hedonic principle.
Affective Attitudes
Affective attitudes are evaluations of the target behavior based on aggregation of the likelihood of anticipated affective responses—for example, exercise is enjoyable versus miserable. Affective attitudes are contrasted with instrumental attitudes in which the target behavior is evaluated based on aggregation of expected instrumental outcomes—for example, exercise is beneficial versus harmful (Ajzen, 1991; Crites, Fabrigar, & Petty, 1994). Though affective attitudes have an evaluative component, they are distinct from affective responses to the target behavior. Affective attitudes can be considered and reported at any time, whereas affective response occurs only in the context of the target behavior. Moreover, one may, for example, report a positive affective attitude toward exercise while simultaneously experiencing a negative affective response.
Two recent meta-analyses have shown consistent positive associations between affective attitudes toward exercise and exercise behavior (Nasuti & Rhodes, 2013; Rhodes et al., 2009). 3 Likewise, individual studies have shown positive associations between affective attitudes and alcohol and marijuana use (Simons & Carey, 1998), smoking (Trafimow & Sheeran, 1998), and blood donation (Conner, Godin, Sheeran, & Germain, 2013). Finally, at least three studies have examined affective attitudes toward multiple health-related behaviors, generally showing positive associations that are in many instances stronger than the associations between instrumental attitudes and behavior (Ajzen & Timko, 1986; Keer, van den Putte, & Neijens, 2009; Trafimow et al., 2004).
Affective Associations
Affective associations are automatic associations between the target behavior and previously experienced affective responses to the target behavior (Kiviniemi, Voss-Humke, & Seifert, 2007). For example, someone who is a habitual cigarette smoker may automatically associate the thought of smoking with the pleasant taste of a cigarette. The potential effects of affective associations on health behavior are consistent with the somatic marker hypothesis in which automatic somatosensory representations of hedonic responses to the target behavior are posited to influence behavioral decision-making (Damasio, 1994). Likewise, the concept of affective associations is implicated in the affect heuristic in which affective associations with potential behavioral alternatives influence behavioral decision-making (Finucane, Alhakami, Slovic, & Johnson, 2000). Theoretically, affective associations and affective attitudes are a function of automatic versus deliberative processing, respectively. However, questionnaire-based assessments of affective association (e.g., “I feel pleasure vs. displeasure when considering [target health behavior]”) and affective attitudes (e.g., “[target health behavior] is pleasant vs. unpleasant”) are similar, and may be difficult to distinguish empirically (Richard, van der Pligt, & de Vries, 1996).
Relative to anticipated affect and affective attitudes, affective associations have received less attention in health behavior research. However, a few studies have shown that more positive affective associations are associated with greater likelihood of exercise behavior (Kiviniemi et al., 2007), fruit and vegetable consumption (Kiviniemi & Duangdao, 2009), and binge drinking (Karlsson, 2012).
Implicit Attitudes
According to dual-processing theories, explicit attitudes (including affective and instrumental subtypes; see previous lines) are distinguished from implicit attitudes, which are automatically activated evaluations of the target behavior based on an aggregation of affective associations (Gawronski & Bodenhausen, 2006). Theoretically, the relationship between implicit attitudes and affective associations is analogous to the relationship between affective attitudes and anticipated affect, with the two pairs of concepts representing automatic versus reflective processing, respectively (Gawronski & Bodenhausen, 2006; Hofmann, Friese, & Wiers, 2008; but see Conner, Prestwich, & Ayres, 2011).
In order to minimize the effects of conscious deliberation, implicit attitudes are typically assessed via computer-based priming or reaction time tasks (De Houwer, Teige-Mocigemba, Spruyt, & Moors, 2009). Using such measures, several studies, reviewed in the context of a recent meta-analysis, have shown implicit attitudes to be associated with smoking, alcohol and drug use, and eating behavior, though some studies produced null findings (Greenwald, Poehlman, Uhlmann, & Banaji, 2009). A recent narrative review also discusses evidence supporting the importance of implicit attitudes as predictors of health-related behaviors (Sheeran, Gollwitzer, & Bargh, 2013).
Affectively Charged Motivation
Craving and Desire
In multiple theories craving and desire refer to subjectively experienced and affectively charged wanting of an object (e.g., food, drugs) or wanting to perform a target behavior (e.g., sex, smoking; Baker et al., 2004; Franken, 2003; Hofmann & van Dillen, 2012; Kavanagh, Andrade, & May, 2005; Kavanagh et al., 2013; Sayette et al., 2000; Skinner & Aubin, 2010; Tiffany & Conklin, 2000). Alternatively, craving and desire have been defined in terms of a dopaminergic response to a behavioral cue that underlies (though does not always manifest in) the subjective experience of wanting (Berridge, 2007; Berridge & Robinson, 1998). Regardless of whether experiential or neurophysiological aspects of craving and desire are emphasized, craving/desire is intimately tied to the concept of affective response in the context of contemporary theories of reward—that is, people typically crave/desire what they previously had a positive affective response to (Berridge & Robinson, 2003; Cota et al., 2006; Ely et al., 2013; Everitt et al., 2008; Finlayson, King, & Blundell, 2007; Ikemoto & Bonci, 2013; Lutter & Nestler, 2009; Mela, 2006; Nasser, 2001; Nathan & Bullmore, 2009; van den Bos & de Ridder, 2006). However, despite their interlinked roles in reward, craving/desire and affective response are distinct. First, there is an inherent time interval between previous affective response and future instances of craving/desire. Second, craving/desire differs experientially from positive affective response: the experience of craving/desire includes subjective wanting and is not necessarily characterized by positive affective valence. Indeed, craving/desire can include negative affective valence when the target of the craving/desire is not readily available or is in conflict with other behavioral goals (Kavanagh et al., 2005). Finally, craving/desire has different neurological underpinnings than affective response such that, in addictive behaviors, strong craving/desire may occur despite blunting of positive affective responses to the addictive behavior (Berridge & Robinson, 2003; Kalivas & Volkow, 2005; Redish, 2004).
In health behavior research, craving and desire are most often implicated in behaviors that involve immediate positive shifts in affective valence, such as eating calorie-dense foods, smoking, drug use, and sex. Studies employing self-reports of craving/desire, as well as neuroimaging and neuroscience methods in humans and nonhuman animals, show that craving and desire are important determinants of behavior, though certain factors (e.g., behavior availability, social constraints) may moderate their effects (for reviews see Budak & Thomas, 2009; Diamond & Dickenson, 2012; Kalivas & Volkow, 2005; Kavanagh et al., 2013; Kuhn & Gallinat, 2011; P. J. Rogers & Smit, 2000; Tang, Fellows, Small, & Dagher, 2012).
Fear
Fear is an emotion that has a motivational component—that is, to avoid or move away from behaviors or objects that are expected to or have previously resulted in negative affective responses (LeDoux, 2012). The study of fear has a long history in health behavior theory and research. In the fear-drive model of behavior, first proposed in the 1950s, instilling fear of the outcomes of engaging (e.g., smoking, drug use) or not engaging (e.g., cancer screenings, dental hygiene) in certain behaviors was posited to influence performance of the target behavior (Hovland, Janis, & Kelley, 1953). However, theories of fear and health behavior (Leventhal, Diefenbach, & Leventhal, 1992; Miller, Shoda, & Hurley, 1996; R. W. Rogers, 1975, 1983; Witte, 1992) have increasingly emphasized the cognitive interpretation of fear appeals rather than experienced fear (see Ruiter, Abraham, & Kok, 2001).
Accordingly, research on fear appeals and health behavior has focused on cognitive appraisals rather than fear per se (for reviews see de Hoog, Stroebe, & de Wit, 2007; Witte & Allen, 2000). For example, while a growing literature suggests that fear appeals may be effective in the context of cigarette warning labels, few studies have assessed actual fear responses to the warning labels (Hammond, 2011). Additionally, most of the research on fear has focused on fear of the postbehavior outcomes of health-related behaviors, such as the dangers of smoking and drug use, and the health consequences of poor dental hygiene or failure to exercise. Fear may also be conceptualized, however, in terms of motivation to avoid or move away from behaviors that are expected to or have previously resulted in immediate negative affective responses. This relationship between fear and immediate negative affective response is analogous to the relationship between desire/craving and immediate positive affective response. Indeed, some neuroscientists have posited punishment-processing circuitry that links previous negative affective responses (i.e., “disliking”) to fear (i.e., “dread” in Berridge’s [1999] terminology) analogous to the reward-processing brain circuitry that links previous positive affective responses (i.e., “liking”) to desire (i.e., “wanting”; see also Carlezon & Thomas, 2009; Johansen, Cain, Ostroff, & LeDoux, 2011; Levita, Dalley, & Robbins, 2002). The study of fear of immediate negative affective responses is perhaps best applied to beneficial health behaviors, such as exercise, that result in positive instrumental outcomes (i.e., health benefits), but, for many people, tend to have immediate negative affective consequences (Ekkekakis & Lind, 2006). For example, some research suggests that anxiety sensitivity—that is, fear of experiencing anxiety symptoms—can inhibit exercise behavior, particularly for vigorous exercise and for those with higher body mass indexes (BMIs; Moshier et al., 2013; Smits, Tart, Presnell, Rosenfield, & Otto, 2010).
Intrinsic Motivation
In self-determination theory the distinction between intrinsic and extrinsic motivation refers to the pursuit (or avoidance) of affective versus instrumental outcomes of behavior, respectively (Ryan & Deci, 2000). For the most part, intrinsic motivation maps on to the affectively charged motivational states of craving/desire and fear, whereas extrinsic motivation maps on to non-affectively-charged behavioral intentions and goals. However, the mapping is not perfect, because the source of motivation (i.e., pursuit of affective vs. instrumental outcomes of behavior) is logically independent of whether or not a motivational state is (i.e., craving, desire, fear) or is not (i.e., behavioral intention, goal) affectively charged. For example, one can have strong affectively charged desire to perform a behavior because it is expected to result in a large financial reward—that is, extrinsic motivation. Conversely, one may expect that going for a walk would be enjoyable, and thus be intrinsically motivated to do so despite a lack of affectively charged desire. Nonetheless, intrinsic motivation is typically an affectively charged motivational state that involves either craving/desire or fear.
Despite this conceptual overlap with craving, desire, and fear, research on intrinsic motivation and health-related behavior is characterized by a separate literature that is mostly informed by self-determination theory. Research generally supports the role of intrinsic motivation as a predictor of exercise behavior, smoking cessation, and medication adherence (for reviews, see Ng et al., 2012; Wilson, Mack, & Grattan, 2008).
An Affect and Health Behavior Framework
In this section we present an affect and health behavior framework (AHBF) that suggests potential interrelationships among the various affect-related determinants of health behavior (see Figure 2). As a starting point for the framework, affective response to health behavior is divided into immediate and postbehavior affective response, because affective responses that occur during versus following health-related behaviors often have opposing hedonic valences. For example, due to evolved neurological mechanisms, eating calorie-dense foods and engaging in illicit sex or drug use often leads to immediate pleasure (Hladik, Pasquet, & Simmen, 2002; Johnston, 1999; Rozin, 1999). However, because of modern health-related and social contingencies, these same behaviors can lead to postbehavior or postoutcome shame, embarrassment, and regret (Hofmann & Fisher, 2012; Ulijaszek, 2007). Likewise, vigorous physical exercise can lead to immediate pain and discomfort, but can also lead to postbehavior relief for finishing the exercise session, as well as postoutcome pride and satisfaction with the outcomes of exercise (Ekkekakis, 2009; Rose & Parfitt, 2007).
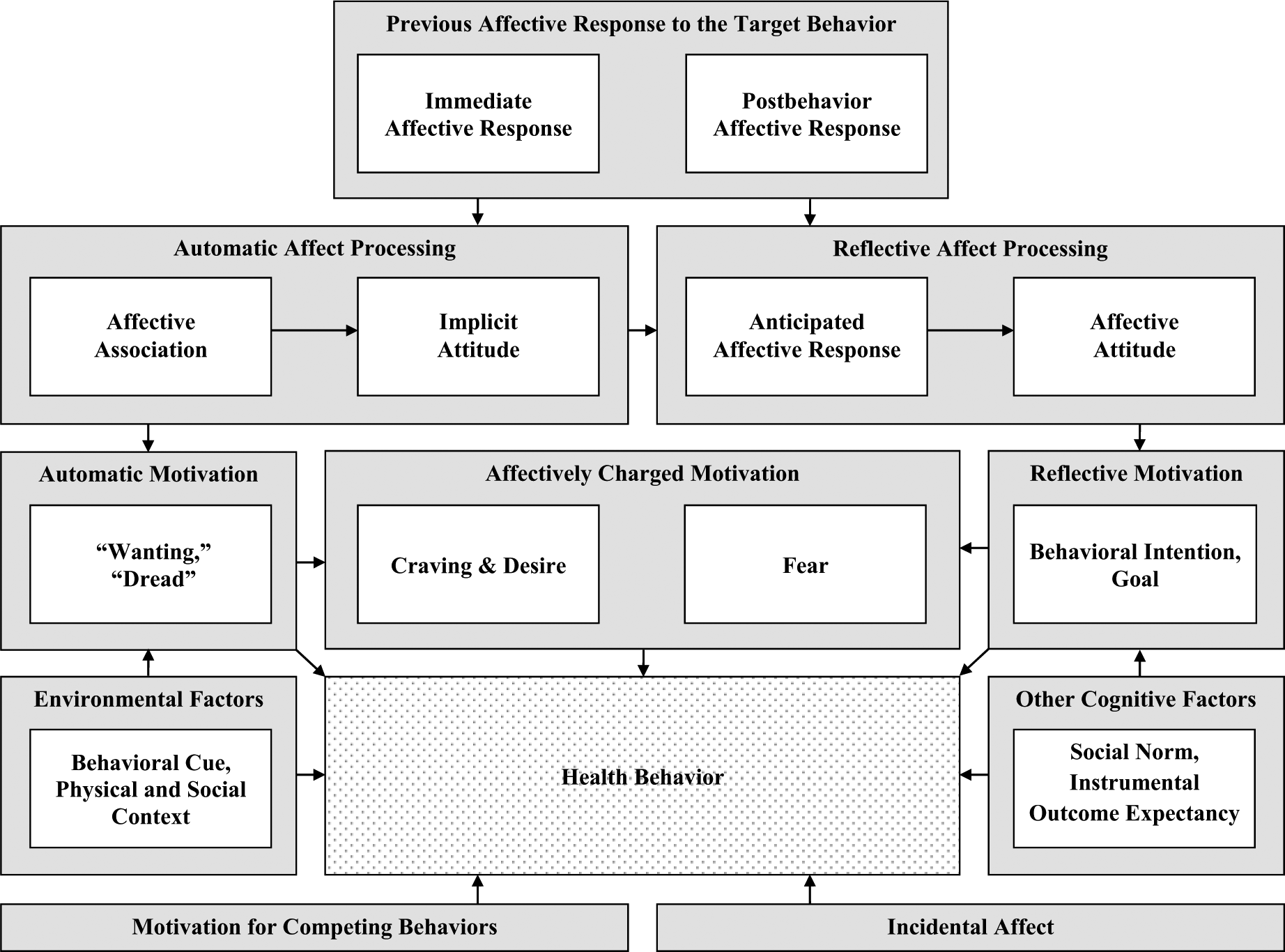
Affect and health behavior framework.
In the AHBF, a causal pathway extends from previous affective response to affect processing to motivation to behavior. This general causal pathway can be further divided into automatic and reflective components based on recent dual-processing perspectives (Evans, 2008; Gawronski & Bodenhausen, 2006; Hofmann et al., 2008; Sheeran et al., 2013; Smith & DeCoster, 2000; Strack & Deutsch, 2004). 4 In the automatic processing pathway, previously experienced positive or negative affective responses to the target behavior increase or decrease (respectively) the likelihood of future behavior through their effects on affective associations and implicit attitudes, and, in turn, automatic neurobiological substrates of motivation (i.e., “wanting” or “dread”; Berridge, 1999; Damasio, 1994; Finucane et al., 2000; Gawronski & Bodenhausen, 2006; Loewenstein, Weber, Hsee, & Welch, 2001). In the reflective processing pathway, anticipated positive or negative affective responses to the target behavior increase or decrease (respectively) the likelihood of future behavior through their effects on deliberative forms of motivation, such as behavioral intentions and goals (Ajzen, 1991; Bandura, 1986; Gilbert & Wilson, 2007; Kahneman et al., 2006; Kirsch, 1985; Loewenstein & Schkade, 1999; Mellers et al., 1997). Theoretically, the automatic processing pathway should be biased toward more immediate affective responses (pain and discomfort of vigorous exercise; pleasure of drug use or unprotected sex) rather than distal affective responses (e.g., pride and satisfaction with the outcomes of regular vigorous exercise; regret and shame for drug use or illicit sex), because, according to models of associative memory (Evans, 2008; Smith & DeCoster, 2000; Strack & Deutsch, 2004), stronger automatic associations are formed among stimuli that have been previously experienced as spatially and temporally contiguous. Conversely, the reflective processing pathway should be biased toward more distal affective responses to the target behavior, because reflective processing allows for deliberation regarding more distal affective consequences of the target behavior (Evans, 2008; Smith & DeCoster, 2000; Strack & Deutsch, 2004).
Conflicts between automatic and reflective motivation (e.g., an automatic impulse to smoke conflicts with the intention to quit smoking) become a focus of conscious attention and result in an affectively charged motivational state (i.e., craving, desire, fear; Baker et al., 2004; Franken, 2003; Hofmann & van Dillen, 2012; Kavanagh et al., 2005). Affectively charged motivation to perform health-related behaviors (i.e., craving and desire) tends to occur in the context of behaviors that are immediately pleasurable but have unfavorable health consequences, such as addictive behaviors, eating delicious foods, and engaging in illicit sex. Conversely, affectively charged motivation to not perform health-related behaviors (i.e., fear, aversion) tends to occur in the context of behaviors that are immediately aversive but have favorable health consequences, such as physical exercise or visiting the dentist. Consistent with theories of affect regulation and affect congruency, incidental affect exerts an independent effect on health behavior that potentially interacts with the above delineated causal chain (Bower, 1981; Forgas, 1995; Morris & Reilly, 1987; Schwarz & Clore, 1983; Tice et al., 2001; Wegener & Petty, 1994).
Finally, it is acknowledged that other factors not emphasized in this article also influence behavior both directly and through their effects on motivation. These include environmental and social contexts (e.g., behavior cues, physical and social environments; Sallis, Owen, & Fisher, 2008; Stokols, 1996), cognitive factors that do not include or directly refer to affect (e.g., social norms, instrumental outcome expectancies; Ajzen, 1991; Bandura, 1986), and motivation for competing behavioral alternatives (e.g., motivation to watch television instead of exercising; Richetin, Conner, & Perugini, 2011).
The AHBF in the Context of Unhealthy (Smoking) and Healthy (Exercise) Behaviors
For someone who smokes, but wants to quit, the strength of intention to quit smoking (i.e., reflective motivation) is based, in part, on anticipation (i.e., reflective affect processing) of postbehavior affective consequences of smoking, such as regret and shame for failing to quit smoking, as well as fear of disease. The sight of a cigarette advertisement in a convenience store (i.e., behavioral cue) may, however, activate automatic “wanting” to smoke (i.e., automatic motivation) based on positive affective associations (i.e., automatic affect processing) with previous immediate affective responses to smoking, such as the pleasurable taste of cigarettes and relief from withdrawal symptoms. When automatic “wanting” to smoke comes into conflict with the intention to quit smoking, the person is likely to experience a conscious craving for cigarettes (i.e., affectively charged motivation). In addition to the strength of intention to quit smoking, automatic “wanting” to smoke, and cigarette craving, smoking behavior may also be influenced by whether smoking is available and permissible (i.e., environmental factors), the person’s mood prior to seeing the cigarette ad (i.e., incidental affect), whether the person is in a rush to go somewhere (i.e., motivation for competing behaviors), and whether smoking is perceived as normative in the social context (i.e., other cognitive factors).
For someone who is previously sedentary, the strength of intention to start an exercise program (i.e., reflective motivation) is based, in part, on anticipation (i.e., reflective affect processing) of postbehavior affective consequences of exercise, such as pride and satisfaction, as well as relief upon finishing the workout. The thought of a planned evening run (i.e., behavioral cue) may, however, activate automatic “dread” of exercise (i.e., automatic motivation) based on negative affective associations (i.e., automatic affect processing) with immediate affective responses to exercise, such as pain and discomfort during vigorous exercise. When automatic “dread” of exercise comes into conflict with the intention to exercise, the person is likely to experience a conscious fear of or anxiety about exercising (i.e., affectively charged motivation). In addition to the strength of intention to exercise, automatic “dread” of exercise, and exercise anxiety, exercise behavior may also be influenced by current weather conditions and availability of an exercise partner (i.e., environmental factors), the person’s mood prior to thinking about the pending exercise session (i.e., incidental affect), whether the person is expecting dinner company that night (i.e., motivation for competing behaviors), and whether the person receives encouragement from their partner (i.e., other cognitive factors).
Summary and Conclusions
In the present review, we identified affect-related concepts that have been examined as potential health behavior determinants and organized them into four categories: affective response, incidental affect, affect processing, and affectively charged motivation. For each concept within these four categories, we summarized relevant theory and empirical research. We then synthesized the affect-related concepts in the context of a conceptual framework using a dual-processing perspective. It is hoped that researchers will find the present review to be a useful starting point for identifying the many affect-related concepts that have been studied in health behavior science.
Footnotes
Author note:
This project was funded in part by a grant from the National Cancer Institute (CA155381). We would like to thank Chris Kahler, Carolyn Rabin, and Dick Winett for their comments on earlier versions of this manuscript. Special thanks to Justin Nash for his feedback on multiple drafts.