Abstract

Background
Bright red rectal bleeding is a common symptom in the young population. Ninety per cent of patients referred for evaluation are found to have benign anorectal pathology; this figure may be higher due to substantial under–reporting of these symptoms, especially in the young population (Penner & Majumdar, 2007; Tally & Jones, 1998). Bowel cancer incidence is strongly related to age: in the UK between 2009 and 2011, an average 43% of bowel cancer cases were diagnosed in people aged 75 years and over, and 95% were diagnosed in those aged 50 and over (Cancer Research UK, 2014).
Younger patients (less than 45 years in age) are perhaps over-investigated when presenting solely with bright red rectal bleeding. Referral to a surgical clinic will involve detailed history, examination, as well as proctoscopy and/or rigid sigmoidoscopy (Ferguson, 2005). To subject all patients to flexible sigmoidoscopy is a significant strain on resources (the current UK cost is approximately £600), especially in the absence of associated bowel symptoms, or after identifying an anorectal cause at proctoscopy or rigid sigmoidoscopy. In this article, we evaluate the flexible sigmoidoscopy examinations performed in our district general hospital for bright red rectal bleeding as the only reported symptom in patients younger than 45 years in age, and propose a management pathway for such patients in secondary care.
Current evidence
Any patient with rectal bleeding meeting the following criteria should be referred urgently under the 2-week wait guidelines, as recommended by the National Institute for Health and Care Excellence (NICE) Referral Guidelines for Suspected Cancer (NICE, 2005):
Aged 40 years or more, with rectal bleeding and change in bowel habit towards looser and/or more frequent stools for 6 weeks or more Aged 60 years or more, with rectal bleeding persisting for 6 weeks or more without change in bowel habit and without anal symptoms Aged 60 years or more, with change in bowel habit towards looser and/or more frequent stools for 6 weeks or more independent of rectal bleeding Palpable rectal or lower abdominal mass irrespective of age Iron-deficiency anaemia in men of any age (Hb 11 or less) and non-menstruating women (Hb 10 or less)
Separately, the British Society of Gastroenterology commissioning guidelines (British Society of Gastroenterology, 2009) on current best practice states:
Those with a very low risk of significant pathology (young, no other concerning symptoms, obvious anal cause of bleeding) are usually simply reassured and managed conservatively (dietary advice, topical medication) Where the risk of other pathology (particularly cancer) is higher (e.g. aged over 50 years, absence of anal source of bleeding, change in bowel habit), investigation is needed (flexible sigmoidoscopy, colonoscopy or virtual colonoscopy, depending on symptoms)
Design
Data was collected retrospectively from the endoscopy database of all flexible sigmoidoscopy examinations over 3 years, from 2010 to 2013. A younger patient for the purpose of this service evaluation is defined as one aged 45 years or less. Patients with rectal bleeding as their only symptom were included in the study. The presence of any associated bowel symptoms, anaemia, raised faecal calprotectin, weight loss, a palpable mass, previous history of inflammatory bowel disease or polyps, and family history of polyps served as exclusion criteria for the study.
Referrals included suspected cancer 2-week wait, all urgent and in-patient referrals. However, routine and follow-up referrals were excluded for the purpose of this study. Mean with one standard deviation was computed for the relevant data and statistics calculated using student t-test and Fishers exact analysis. A p-value of less than 0.05 was considered significant.
Results
A total of 3000 flexible sigmoidoscopies were performed and after applying the exclusion criteria, 516 patients were identified. Either Moviprep or Kleen-Prep was used as the bowel preparation. Entonox was used as analgesia in the majority; a small proportion required fentanyl or pethidine. The age range of patients in the study group ranged from 17 to 44 years, with a mean of 34.9 years. There were 247 female patients and 269 male patients. Although no procedure-related complications were reported, eight flexible sigmoidoscopies were incomplete due to pain and/or poor bowel preparation. Endoscopic diagnoses included normal flexible sigmoidoscopy, haemorrhoids, diverticular disease, anal fissure, solitary rectal ulcer, polyps and proctitis (Fig. 1).
Endoscopic findings at flexible sigmoidoscopy (n = 516).
Of the 400 patients who had no mucosal pathology identified at flexible sigmoidoscopy, over 96% reported their symptoms to have resolved completely at the time of the procedure, and in the remaining patients, their symptoms were attributed to small internal haemorrhoids not requiring any intervention. At endoscopy, 39 polyps were identified, of which 31 were in the rectum and eight in the sigmoid colon. Standard fluid-assisted polypectomy was carried out for larger polyps (more than 5 mm), with the remaining ones being removed using a hot snare. Histological assessment revealed nine tubulovillous adenomas (two larger than 1 cm), one carcinoid tumour of the rectum, and two carcinomas of the rectum (0.4%). Two had no polyp tissue on histology and the remaining 25 were hyperplastic polyps of the rectum. On subgroup analysis, increasing age and male sex were identified as predictors for polyp occurrence (p-value less than 0.05).
Discussion
Rectal bleeding and/or a change in bowel habit (frequent bowel motions or increased looseness) in association with increasing age (over 60 years) serves as a powerful predictor of colorectal cancer (Selvachandran, Hodder, Ballal, Jones, & Cade, 2002). The positive predictive value of rectal bleeding as a symptom of colorectal cancer increases with age: 21% in the 70–79 years age group and less than 1% in patients younger than 50 years (Wauters, van Casteren, & Buntinx, 2000).
Prevalence of advanced adenomas (defined as adenomas 1 cm or greater, or with villous components (tubulovillous or villous), or with high-grade or severe dysplasia), such as cancer, increases with age and this has been reported by several studies (Brenner, Althenhofen, & Hoffmeister, 2010; Chung et al., 2010). In our service evaluation, the adenoma rate was 1.7%, including an advanced adenoma rate of 0.4% and a cancer rate at 0.4%. Advanced adenomas are likely to develop into cancer. However, age alone should not serve as the differentiating factor in evaluating these patients. In the younger, lower-risk patient with suspected inflammatory bowel disease (IBD), faecal calprotectin is a useful screening tool. A flexible sigmoidoscopy costs about £600, whereas faecal calprotectin costs less than £50. Waugh et al. (2013) reported that a negative faecal calprotectin result is a reliable way of excluding IBD, thus reducing the need and cost for invasive investigations such as colonoscopy. Separately, various epidemiological studies based on long-term follow-up periods of up to 10 years on outcomes in undiagnosed rectal bleeding have reported a cancer incidence of 2.3%. Of these, no cancer was diagnosed in patients younger than 50 years, however, 7% had polyps (Fitjen et al., 1995; Helfand, Marton, Zimmer-Gembeck, & Sox,1997).
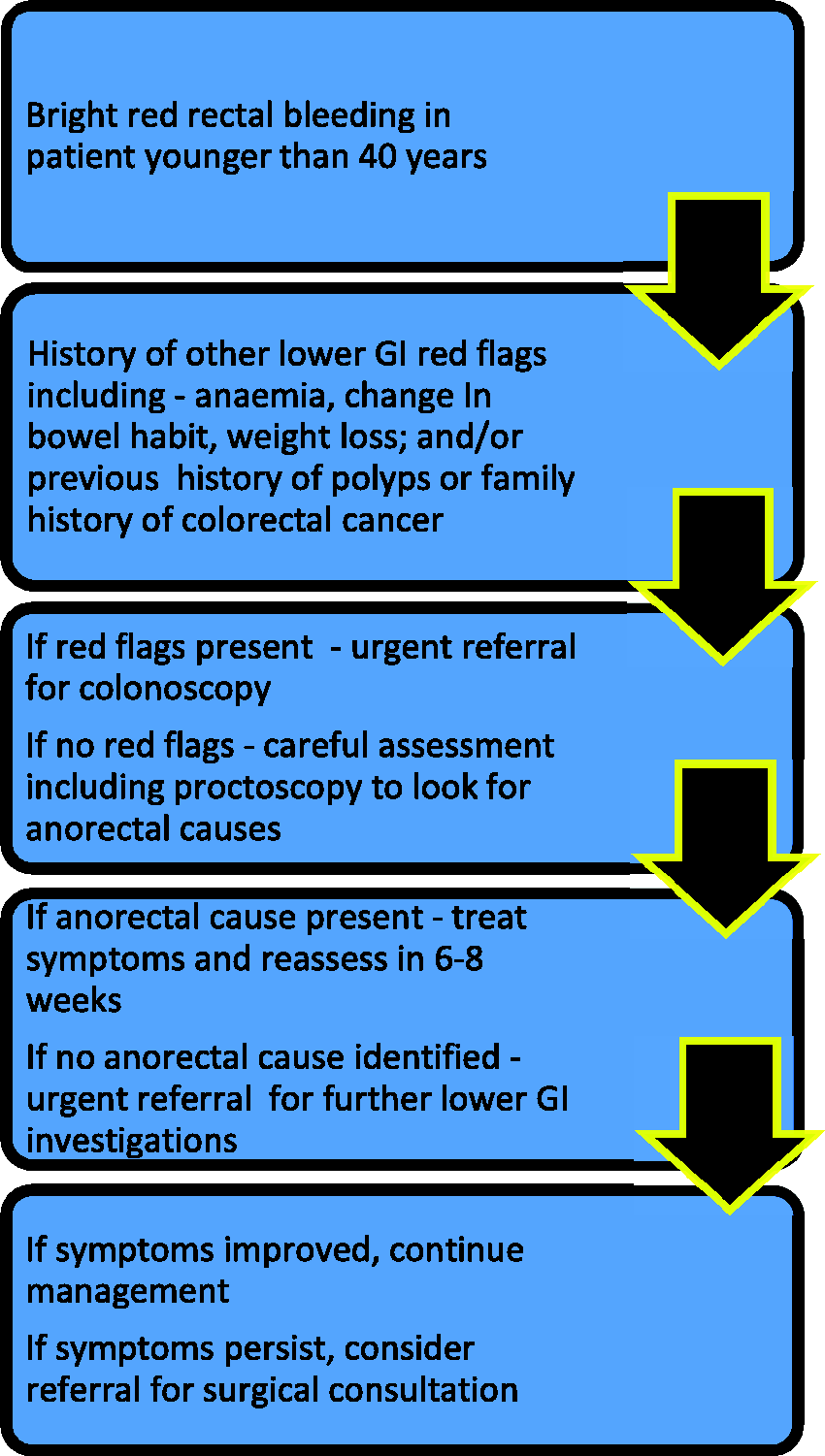
It is reasonable to have a high index of suspicion in patients aged less than 45 years presenting with rectal bleeding, especially when symptoms persist along with no identifiable ano-rectal pathology: this should warrant further evaluation (Fig. 2). Selective use of flexible sigmoidoscopy in such situations may offer a more cost-effective diagnostic approach; thus, reducing the strain on limited NHS resources in evaluating younger patients with bright red rectal bleeding and an identifiable ano-rectal source.
Suggested referral pathway in evaluation of bright red rectal bleeding in the young population.