
Abstract
Polycystic ovary syndrome is the most common endocrine disturbance to affect women, with approximately 10–15% of women experiencing this problem. It involves a spectrum of signs and symptoms, which include menstrual cycle disturbance and infertility, dermatological problems of acne and hirsutism (sometimes alopecia), and being overweight. The latter both aggravates the condition, and increases the risk for metabolic problems that lead to type 2 diabetes and cardiovascular disease.
The GP curriculum and polycystic ovary syndrome
Know that women-specific health matters including contraception, pregnancy, menopause and disorders of reproductive organs will account for over 25% of your time as a GP Demonstrate knowledge of women’s health problems, conditions and diseases, and recognise that some non-gender-specific issues present differently in women, such as depression, alcoholism, eating disorders and domestic violence Recognise common signs and symptoms of, and know how to manage, gynaecological disease; be the first port of call for pregnancy, eating disorders and other conditions confined to or more common in women, involving other members of the healthcare team as appropriate Demonstrate an understanding of the important risk factors in the diagnosis and management of women’s problems Discuss the psychological component of women’s health and the need, in some cases, to provide women patients with additional emotional and organisational support
Definition and diagnosis
Normal ovarian function relies upon the selection of a follicle, which responds to an appropriate signal (follicle-stimulating hormone, FSH) in order to grow, become ‘dominant' and ovulate. This mechanism is disturbed in women with polycystic ovary syndrome (PCOS), resulting in multiple small ovarian cysts (follicles), most of which contain potentially viable oocytes but within dysfunctional follicles.
PCOS is a heterogeneous condition, whose pathophysiology appears to be multifactorial and polygenic. The definition of the syndrome has been much debated. Key features include menstrual cycle disturbance, hyperandrogenism and obesity. There are many extra-ovarian aspects to the pathophysiology of PCOS, yet ovarian dysfunction is central (Balen, 1999). An international consensus meeting redefined PCOS as requiring the presence of two out of the following three criteria (The Rotterdam ESHRE/ASRM-sponsored PCOS Consensus Workshop Group, 2004):
A menstrual cycle disturbance (oligomenorrhoea or amenorrhoea) Hyperandrogenism (clinical and/or biochemical) Polycystic ovaries as seen on ultrasound scan
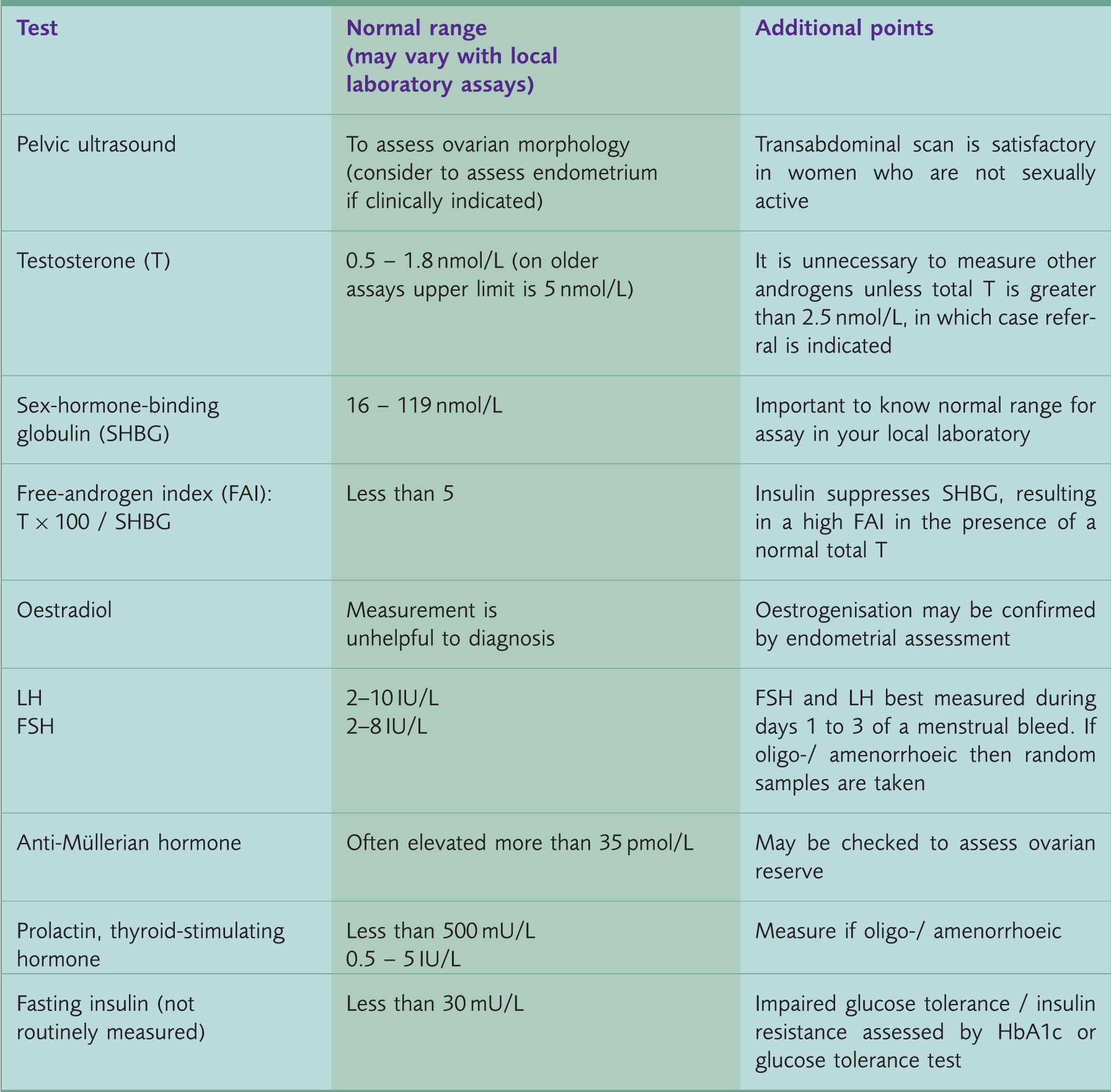
Investigations for PCOS.
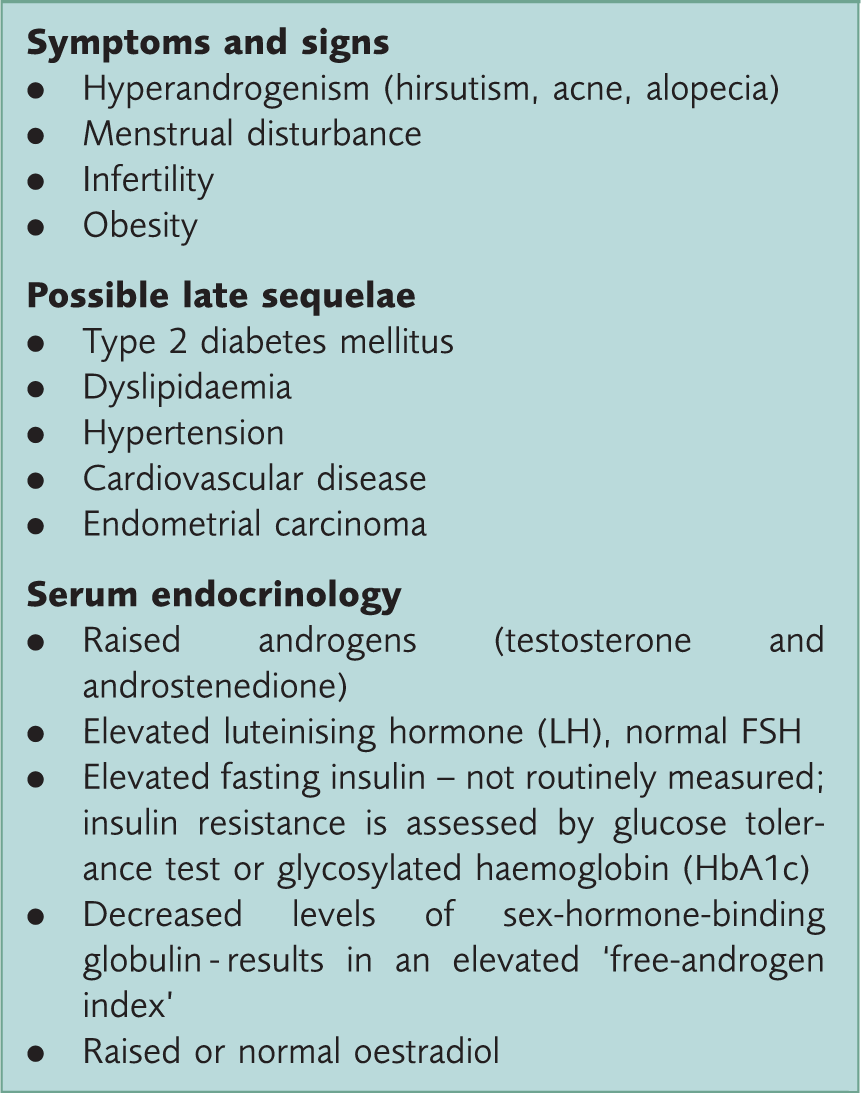
Heterogeneity and expression of PCOS
The spectrum of clinical manifestations of PCOS.
Weight is one of a number of interlinking factors that may affect the expression of PCOS. A gain in weight is associated with a worsening of symptoms, whereas weight loss will ameliorate the endocrine and metabolic profile and symptomatology (Clark et al., 1995). Elevated serum concentrations of insulin are more common in both lean and obese women with PCOS than weight-matched controls. Indeed, it is hyperinsulinaemia that appears to be a key player in the pathogenesis of the syndrome, particularly in those who are overweight. Insulin stimulates androgen secretion by the ovarian stroma and appears to affect the normal development of ovarian follicles, both by the adverse effects of androgens on follicular growth and possibly also by suppressing apoptosis and permitting the survival of follicles otherwise destined to disappear (Dunaif, 1997). The prevalence of diabetes in obese women with PCOS is at least 11%, and so a measurement of impaired glucose tolerance is important and long-term screening advisable (Bates & Legro, 2013). Insulin resistance correlates both with inter-menstrual interval and with hyperandrogenaemia: in other words the greater the degree of menstrual disturbance or androgen excess the greater the metabolic disturbance.
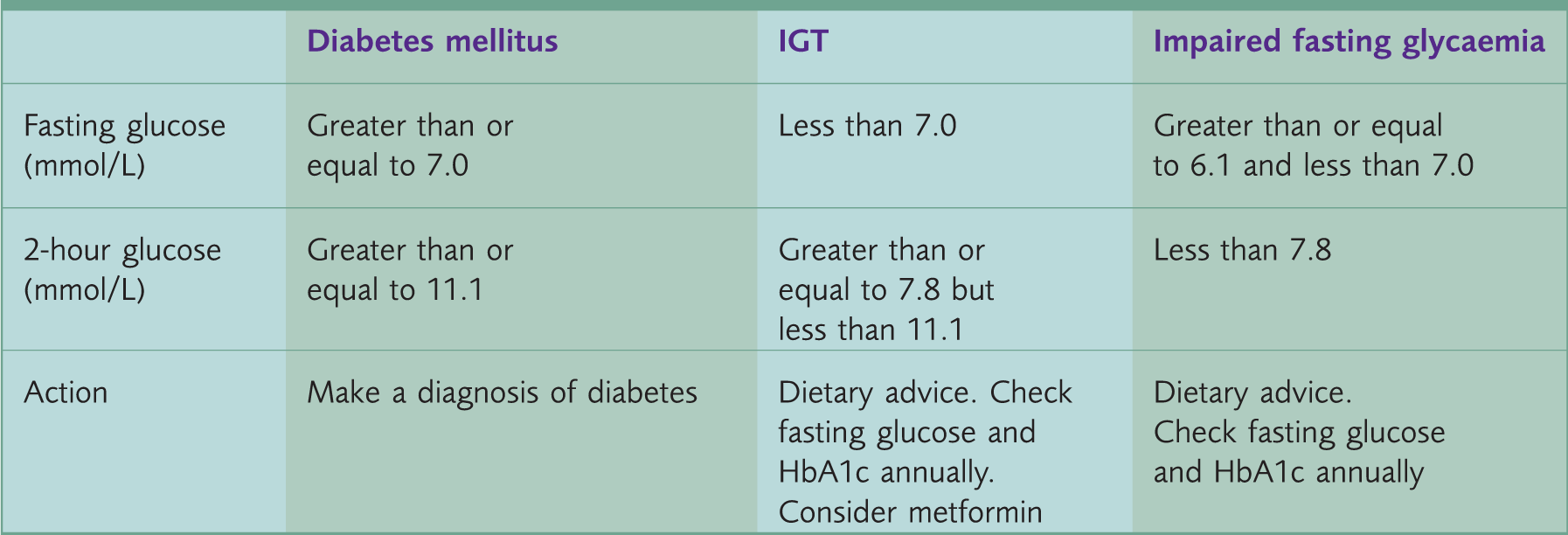
Definitions of glucose tolerance after a 75 g GTT.
There are significant ethnic variations in the degree of insulin resistance (IR) and hence the expression PCOS, with women of South Asian origin having a greater degree of IR at a lower BMI than Caucasian European women (Wijeyeratne, Udayangani, & Balen, 2013). Because of this increased risk of IR it has been suggested that South Asian women should have an assessment of glucose tolerance if their BMI is greater than 25 kg/m2.
Management of PCOS
The clinical management of a woman with PCOS should be focused on her individual problems. However, the symptoms typically associated with the condition have also been shown to lead to a significant reduction in health-related quality of life (HRQoL) (Jones, Hall, Balen, & Ledger, 2008). HRQoL is a multi-dimensional, dynamic concept that encompasses physical, psychological and social aspects that are associated with a particular disease or its treatment. Therefore, management of women with PCOS needs to consider and understand the negative impact this condition may have upon these psycho-social parameters. For example, although the management of hirsutism may be considered as a purely cosmetic issue, excessive facial hair has been shown to be one of the major causes of marked psychological stress in women with PCOS (Jones et al., 2008). Infertility and weight issues have also been found to affect other social and psychological parameters. Infertility can cause tensions within the family, altered self-perception, and problems at work.
Although obesity worsens the symptoms, the metabolic scenario may conspire against weight loss and many women experience frustration in attempts to lose weight and suffer from low-esteem and poor body image. However, diet and physical activity are key to symptom control. Exercise and weight loss are the most physiological way to improve insulin sensitivity and improve the metabolic and reproductive abnormalities associated with the syndrome. In women with PCOS, it has been demonstrated that even relatively modest weight loss improves the hormonal profile and improvement in the reproductive outcome for all forms of fertility treatment (Clark et al., 1995). Since the association between insulin resistance and BMI is stronger in obese women with PCOS compared with weight-matched controls, the benefits of weight loss should be even greater in women with PCOS.
Obesity
Obesity worsens both symptomatology and the endocrine profile; therefore, obese women (BMI more than 30 kg/m2) should be encouraged to lose weight. Weight loss improves the endocrine profile, the likelihood of ovulation, and a healthy pregnancy. Much has been written about diet and PCOS. The right diet for an individual is one that is practical, sustainable and compatible with her lifestyle. It is sensible to reduce glycaemic load by lowering sugar content in favour of more complex carbohydrates and to avoid fatty foods. Meal replacement therapy or low calorie diets may be appropriate: it is often helpful to refer to a dietitian, if available. An increase in physical activity is essential, preferably as part of the daily routine. Thirty minutes per day of brisk exercise is encouraged to maintain health, but to lose weight, or sustain weight loss, 60 to 90 minutes per day is advised. Concurrent behavioural therapy improves the chances of success of any method of weight loss.
Anti-obesity drugs such as orlistat have limited and short-term benefit. Metformin, of which more below, does not enhance weight reduction in women with PCOS (Tang, Lord, Norman, Yasmin, & Balen 2012). For some it is necessary to consider bariatric surgery (gastric bypass or banding).
Menstrual irregularity
Patients with PCOS are not oestrogen deficient; those with amenorrhoea are at risk not of osteoporosis but rather of endometrial hyperplasia or adenocarcinoma (due to the unopposed actions of oestrogen in the absence of progesterone that is usually released after ovulation). An ultrasound assessment of endometrial thickness provides a bioassay for oestradiol production by the ovaries and conversion of androgens in the peripheral fat. If a woman is not having at least quarterly periods, a pelvic ultrasound scan should be considered, and if the endometrium is thicker than 15 mm, a withdrawal bleed should be induced. If the endometrium fails to shed, then endometrial sampling is required to exclude endometrial hyperplasia or malignancy.
The easiest way to control the menstrual cycle and ensure shedding of the endometrium is the use of a low-dose combined oral contraceptive preparation. This will result in an artificial cycle and regular shedding of the endometrium. As women with PCOS are thought to be at increased risk of cardiovascular disease a ‘lipid friendly’ combined contraceptive pill should be used (The Amsterdam ESHRE/ASRM-sponsored 3rd PCOS Consensus Workshop Group, 2012). An alternative is to give an oral progestogen (such as medroxyprogesterone acetate, Provera) for 12 days every 1 to 3 months to induce a withdrawal bleed. It is also important once again to encourage weight loss. An alternative means of providing endometrial protection is the use of a progestogen-secreting Mirena intrauterine system (IUS).
Infertility
Ovulation can be induced with the anti-oestrogen clomifene citrate (50–100 mg), given on days 2 to 6 of a natural or artificially induced bleed. Although clomifene is successful in inducing ovulation in over 80% of women, pregnancy only occurs in about 40%. Clomifene citrate should only be prescribed in a setting where ultrasound monitoring is available (and performed) in order to minimise exposure to the 10% risk of multiple pregnancy and to ensure that ovulation is taking place (Tarlatzis et al., 2008) – this usually means initiation and follow up through secondary care. A daily dose of more than 100 mg rarely confers any benefit. Once an ovulatory dose has been reached, the cumulative conception rate continues to increase for up to 10 to 12 cycles (Balen, 2013).
The therapeutic options for patients with anovulatory infertility and who are resistant to anti-oestrogens are either parenteral gonadotrophin therapy or laparoscopic ovarian diathermy (Balen, 2013), both accessed through referral to secondary care (fertility services). Due to the polycystic ovary being very sensitive to stimulation by exogenous hormones, it is very important to start with very low doses of gonadotrophins and follicular development must be carefully monitored by ultrasound scans. The advent of transvaginal ultrasonography has enabled the rate of a multiple pregnancy to be reduced to approximately 5%, due to its higher resolution and clearer view of the developing follicles. Cumulative conception and live birth rates after 6 months may be 62% and 54%, respectively, and after 12 months 73% and 62%, respectively (Balen, 2013). Close monitoring should enable treatment to be suspended if three or more mature follicles develop, as the risk of multiple pregnancy obviously increases.
Women with PCOS are also at increased risk of developing ovarian hyperstimulation syndrome (OHSS). This occurs if too many follicles (greater than 10 mm) are stimulated during gonadotrophin therapy. It causes symptoms of:
Abdominal distention Discomfort Nausea and vomiting, and sometimes Difficulty breathing
The mechanism for OHSS is thought to be secondary to activation of the ovarian renin-angiotensin pathway and excessive secretion of vascular epidermal growth factor. Ascites, and pleural and pericardial effusions can occur, and the resultant haemoconcentration can lead to thromboembolism. The situation worsens if a pregnancy has resulted from the treatment as human chorionic gonadotrophin from the placenta further stimulates the ovaries. Hospitalisation is sometimes necessary in order for intravenous fluids and heparin to be given to prevent dehydration and thromboembolism. Although OHSS is rare, it is potentially fatal and should be avoidable with appropriate monitoring of gonadotrophin therapy.
Ovarian diathermy is free of the risks of multiple pregnancy and ovarian hyperstimulation, and does not require intensive ultrasound monitoring. Laparoscopic ovarian diathermy has taken the place of wedge resection of the ovaries (which resulted in extensive peri-ovarian and tubal adhesions), and it appears to be as effective as routine gonadotrophin therapy in the treatment of clomiphene-insensitive PCOS, although time to pregnancy is a little slower (Balen, 2013).
Hyperandrogenism, hirsutism and acne
The bioavailability of testosterone is affected by the serum concentration of sex-hormone-binding globulin (SHBG). High levels of insulin lower the production of SHBG and so increase the free fraction of androgens. Elevated serum androgen concentrations stimulate peripheral androgen receptors, resulting in an increase in 5-alpha reductase activity, directly increasing the conversion of testosterone to the more potent metabolite, dihydrotestosterone. Symptoms of hyperandrogenism include hirsutism and acne, which are both very distressing conditions.
Hirsutism is characterised by terminal hair growth in a male pattern of distribution, including chin, upper lip, chest, upper and lower back, upper and lower abdomen, upper arm, thigh and buttocks. A standardised scoring system, such as the modified Ferriman–Gallwey score should be used to evaluate the degree of hirsutism before and during treatments.
Treatment options for hirsutism include cosmetic and medical therapies. Drug therapies may take 6–9 months or longer before any improvement of hirsutism is perceived; thus, physical treatments including electrolysis, waxing and bleaching may be helpful while waiting for medical treatments to work.
For many years the most ‘permanent’ physical treatment for unwanted hair has been electrolysis. This needs to be performed by an expert practitioner. However, it is time-consuming, painful, expensive, and regrowth is not uncommon. There is still no really permanent cosmetic treatment; however, the last few years have seen considerable development in the use of laser and photothermolysis techniques. There are many different types of laser in production and each requires evaluation of dose intensity, effectiveness and safety. The technique is promising, being faster and more effective than shaving, waxing or chemical depilation. Repeated treatments are required for a near-permanent effect, due to only hair follicles that are in their growth phase being obliterated at each treatment. Hair growth occurs in three cycles, so 6–9 months of regular treatments are typical. Patients should be appropriately selected (dark hair on fair skin is best), and warned that complete hair removal cannot be guaranteed and some scarring may occur. At present it is not widely available and is still an expensive option.
Eflornithine (Vaniqa) has been recently developed as a topical treatment for hirsutism. It works by inhibiting the enzyme ornithine decarboxylase in hair follicles and may be a useful therapy for those who wish to avoid hormonal treatment, although it may also be used in conjunction with hormonal therapy. It may cause some thinning of the skin, therefore, a high factor sun block is recommended in the summer.
Anti-androgen therapy for hirsutism aims to stop further progression and decrease the rate of hair growth. Anti-androgen therapy for acne aims to lower sebum excretion, alter follicular cell desquamation, reduce propionibacteria and reduce inflammation. When using anti-androgen therapy, adequate contraception is important in women of reproductive age as transplacental passage of anti-androgens may disturb the genital development of a male fetus (Fauser et al., 2012).
In some cases the combined oral contraceptive pill (COCP) is in itself therapeutic. Oestrogens lower the level of circulating androgens by a combination of a slight inhibition of gonadotrophin secretion and by an increase in hepatic production of SHBG resulting in lower levels of free testosterone. The best contraceptive treatment of proven effectiveness is a combination of the synthetic progestogen cyproterone acetate, which is anti-gonadotrophic and anti-androgenic, with ethinyl oestradiol. Co-pyrindiol (Dianette) contains ethinyloestradiol (35 micrograms) in combination with cyproterone (2 mg). It is licensed for moderate-to-severe levels of hirsutism and severe acne. The anti-androgen effect reduces sebum excretion in 2–3 months and results in clinical improvement in acne in 4–6 months (Fauser et al., 2012).
Cyproterone acetate can in rare cases result in liver damage, and liver function should be checked regularly (after 6 months and then annually). There is thought to be an increased risk of thromboembolism and so once symptom control has been achieved and sustained over 3–4 months, it is recommended that women are switched to a lower-dose COCP.
Spironolactone is a weak diuretic with anti-androgenic properties. It may be used at a daily dose of 25–100 mg in women with either hirsutism and/or acne if the COCP is contra-indicated. Drosperinone is a derivative of spironolactone and contained in the COCP, Yasmin, which also appears to be effective for women with PCOS. Again there have been some concerns about the thromboembolic risk of the newer COCPs, and so care should be taken in their prescription. Other anti-androgens, such as ketoconazole, finasteride and flutamide have been tried, but are not widely used in the UK for the treatment of hirsutism in women due to their adverse side effects (in particular flutamide has been associated with fatal hepatotoxicity). Furthermore, they are no more effective than cyproterone acetate (Fauser et al., 2012).
Topical anti-acne agents can be safely and successfully combined with systemic anti-androgen therapy in an attempt to target as many aetiological factors as possible. However, these topical treatments alone have little effect on sebum production, so are not generally successful when utilised alone in acne associated with PCOS. Topical retinoids impact on the microcomedo, which is the precursor to non-inflammatory and inflammatory acne lesions. They also have direct comedolytic and anti-inflammatory activity. These agents are useful adjuvant therapies in combination with anti-androgen treatments, and can be used as maintenance treatment after discontinuation of systemic therapy. Topical antimicrobials (benzoyl peroxide / antibiotics) have good anti-inflammatory activity, and should help to reduce inflammatory lesions when used alongside anti-androgen treatment.
Oral isotretinoin, a hospital-only prescribed medication, is the single systemic therapy that targets the four main aetiological factors implicated in acne. However, it is currently only licensed for severe or scarring acne not responding to other therapies. A European Directive concerning isotretinoin has enforced a strict pregnancy prevention programme, due to the high risk of teratogenecity with this drug (European Agency for the Evaluation of Medicinal Products, 2003). COCPs can be used safely alongside oral isotretinoin and are recommended by the European Directive. Although clinical clearance of acne lesions with oral isotretinoin is very likely, relapse rates post-therapy are higher than average when acne is associated with PCOS.
Insulin-sensitising agents: metformin
A number of pharmacological agents have been used to amplify the physiological effect of weight loss, notably metformin. This biguanide inhibits the production of hepatic glucose and enhances the sensitivity of peripheral tissue to insulin, thereby decreasing insulin secretion. It was suggested from some initial small studies that it may ameliorate hyperandrogenism in women with PCOS and restore menstrual cyclicity in some cases, although subsequent randomised controlled trials (RCTs) have failed to show a significant benefit. There has been much publicity about the use of metformin. It does not appear to induce weight loss, although coincident weight loss will of course provide additional benefit. Indeed in Leeds we have performed the largest RCT to look at metformin versus placebo and found no benefit from metformin over 6 months with regard to either menstrual control or other symptoms (Tang, Glanville, Barth, Hayden, & Balen, 2006). Those who improved were women who lost weight whether on metformin or placebo. Large RCTs and our Cochrane meta-analysis have also demonstrated no benefit from metformin when combined with clomifene citrate (Tang et al., 2012). Therefore, metformin does not appear to hold the promise that was initially presumed. We only advise metformin therapy in women with impaired glucose tolerance or type 2 diabetes.
Key points
PCOS is a heterogeneous condition, and may be familial There are long-term risks of developing diabetes and possibly cardiovascular disease, particularly in those who are overweight If patients are obese, weight loss should be encouraged to improve symptoms, reproductive function and long-term health Menstrual cycle control is achieved by cyclical oral contraceptives, progestogens, or a Mirena IUS can be used to protect the endometrium Hyperandrogenism can be managed with some COCPs or with spironolactone, although reliable contraception is required with all anti-androgen therapy There is no evidence of benefit from metformin, unless women have impaired glucose tolerance or type 2 diabetes.