
Abstract
Each year, breast lumps are the feature of concern for many thousands of patients presenting to primary care. Due to the major publicity regarding breast cancer, many patients present promptly, concerned that the lump is cancerous. However, a few women present late, resulting in delayed diagnosis of cancer and poorer outcomes. It can be difficult to evaluate symptoms and clinical findings to distinguish between potentially malignant and benign conditions, however, by using the information in this article GPs should be able to improve their ability to manage patients locally and judge when a referral to secondary care is required.
The GP curriculum and breast lumps
Demonstrate knowledge of women’s health problems, conditions and diseases Provide information to patients on possible local support services, referral services, networks and groups for women (e.g. breast cancer nurses) Have knowledge of breast pain, breast lumps and nipple discharge Demonstrate a reasoned approach to the diagnosis of women’s symptoms in a manner that is comfortable for both the patient and the GP, using history, examination, incremental investigations and refer appropriately Perform a competent and sensitive breast examination, paying attention to explanation, informed consent, professional etiquette and comfort Describe the issues relating to the use of chaperones (e.g. the added embarrassment that can come from the presence of a third person; your protection from malicious complaints and safeguarding issues for the patient) Intervene urgently with suspected malignancy and have a low threshold for the referral of breast lumps Demonstrate an understanding of the importance of risk factors in the diagnosis and management of women’s problems, e.g. is a patient who presents with a breast lump on hormone replacement therapy? Use screening strategies relevant to women (e.g. cervical, breast, other cancers, postnatal depression) and advise patients on their advantages/disadvantages Discuss the psychosocial component of women’s health and the need, in some cases, to provide women patients with additional emotional and organisational support (e.g. in relation to pregnancy options, hormone replacement therapy, breast cancer and unemployment) Be familiar with and implement the key national guidelines that influence healthcare provision for women’s problems
More than 90% of patients who attend their GP due to breast problems have benign conditions. It is important for GPs to be able to recognise the signs and symptoms that may represent malignancy, and to have the skills to compassionately manage benign disease.
Lumps in the breast are a common primary care presentation. The majority are benign, but referral is recommended for discrete breast lumps. The chances of a woman with a discrete breast lump having breast cancer are significantly higher than that for those with simply lumpiness of the breast (no specific focal breast lump). This distinction is difficult, but most important to judge, and a sensible cautious approach is recommended.
This article focuses on the management and referral to secondary care of patients with breast lumps, working on the principle that cancer should be considered and excluded in all cases. The differential diagnosis of breast lumps and other related breast conditions are considered later in the text.
Primary care evaluation of a patient with breast problems
The basis of a primary care assessment is, as always, the history and examination of the patient. The aim of the assessment is to determine if a breast lump is present, and if a referral to secondary care is required or if management in primary care is sufficient.
Clinical history certainly assists with the assessment of any breast symptoms. A history of a lump may indicate a number of differential diagnoses. Lumps that have very rapidly appeared are most likely to be cysts; this history is often elicited when patients regularly self-examine and know for sure that the lump has suddenly appeared. Breast cancers are far more insidious; however, along with fibroadenomas and other benign tumours (phylloides tumours) they will become palpable to the patient at some point. Breast tumours will rarely spontaneously reduce in size (unlike cysts).
Breast pain is not usually a feature of breast cancer and is further considered below. Nipple discharge, unless it is bloody and/or unilateral, is an unusual isolated symptom of breast cancer and more frequently represents papillomata, periductal mastitis or duct ectasia. Bilateral nipple discharge as a result of malignancy is extremely unusual, as is bilateral synchronous breast cancer. In female patients, the relationship of the symptom with her menses should be discussed. Cyclical breast pain may be temporally related to menses, and hormonal therapy (should the patient be diagnosed with breast cancer) is in part determined by the presence or absence of regular menses. All female patients of reproductive age should be asked if they could be pregnant!
Any family history and personal history of breast cancer should be explored, as should a prior history of cystic or other benign conditions. However, if the patient has a personal history of benign breast disease (e.g. cysts) it cannot be assumed that a further lump is simply a recurrence of this event. Drug history, such as use of hormone replacement therapy (HRT), is helpful as this, as well as nulliparity and lack of breast- feeding, are relative risk factors for the development of breast cancer.
Systemic enquiry will rarely change the management plan; however, clearly there may be weight loss or bone pain in advanced malignancy. A view of the patient’s ideas, concerns and expectations is very useful - sometimes a patient’s health beliefs can be challenged and their view of their presenting features understood, should they report, for example, a story of a dear friend who has recently died of breast cancer. Any history of smoking should be elicited, since it is a risk factor for periductal mastitis.
After obtaining the history, an examination of the breast is performed. This is best achieved with the patient lying on a couch at an angle of 45° with her arms behind her head. The examiner should use the flats of the fingers (not the tips). The axillary tail of the breast and axillae themselves should also be examined. A chaperone should be offered. If a tumour is palpable, it is more likely to be irregular with skin changes; however, these features alone cannot distinguish the benign from the malignant lump.
The key aim of a primary care assessment of patients with a breast lump is the exclusion of, or onward referral for, suspected breast cancer. Therefore, this condition will be considered before further discussion of other causes of breast lumps and their symptoms. In secondary care, triple assessment is the method by which all breast lumps are evaluated and it is discussed in the following section.
Breast cancer
Around 42 000 new breast cancers are diagnosed each year in the UK and breast cancer is the second- commonest cause of female cancer death (Public Health England, 2015). Three quarters of these cancers are identified symptomatically. GPs regularly see patients with breast symptoms and each year are likely to diagnose approximately one or two patients with new breast cancer.
Breast cancer occurs in both sexes; however, 99% of cases occur in women, with male breast cancer identified in about 250 cases per year in the UK. There is no evidence to suggest that breast cancer presents differently in women than in men and the National Institute for Health and Care Excellence (NICE) referral guidelines for suspected cancer refer to ‘people’ as opposed to men and women (NICE, 2015).
Breast cancer is predominantly detected either through symptomatic presentation or after breast screening. Overall 5-year survival is 85%, and this level improves for those whose cancer is detected and treated at an earlier (often asymptomatic) stage. As a result of this, huge efforts have been made to encourage earlier detection of malignancy by rapid referral of patients to secondary care if they have symptoms suggestive of breast cancer, or a significant family history of the disease (multiple family members or fewer young first-degree relations with breast cancer), as well as screening asymptomatic women via the National Health Service Breast Screening Programme (NHSBSP).
The publication of The Forrest Report in 1986 was instrumental in the implementation of the NHSBSP in 1988. This national 3-year rolling programme screens 1600 000 women each year and, following The Cancer Reform Strategy in 2010, the age range of women eligible for breast screening has been extended to 47–73 years, from the previous range of 50–70 years. There is no doubt that breast screening leads to early diagnosis of breast disease.
The National Awareness and Early Diagnosis Initiative is also aimed at promoting earlier detection of breast disease. It was developed from Improving Outcomes: A Strategy for Cancer 2011. As invitations for breast screening cease when a woman reaches 70, some women may (falsely) believe that their risk of breast cancer may be lower beyond that age; in reality it increases. The initiative for earlier detection is part of a broad agenda to try to improve survival rates for older people by ensuring early and sensible levels of intervention.
Presenting features of breast cancer
The most common presenting feature for breast cancer is a breast lump, which is generally painless. Other less frequently seen but suspicious symptoms include a change in breast shape, or skin changes such as tethering and peau d’orange.
Nipple symptoms such as unilateral discharge (especially if blood-stained) or retraction are possible symptoms of breast cancer, particularly in women older than 60 years in age, and warrant an urgent referral to secondary care. Bilateral multiduct nipple discharge is more likely to be physiological or related to inflammatory conditions such as periductal mastitis or duct ectasia, and most unlikely to be bilateral breast cancer. These patients can be managed at least initially in primary care.
Axillary lumps may be a symptom of breast cancer and breast examination is advised if this is a presenting symptom. In those over 30 years of age the NICE Guideline Development Group suggests that this is a further symptom warranting consideration of early referral. However, this symptom is much less specific for breast cancer.
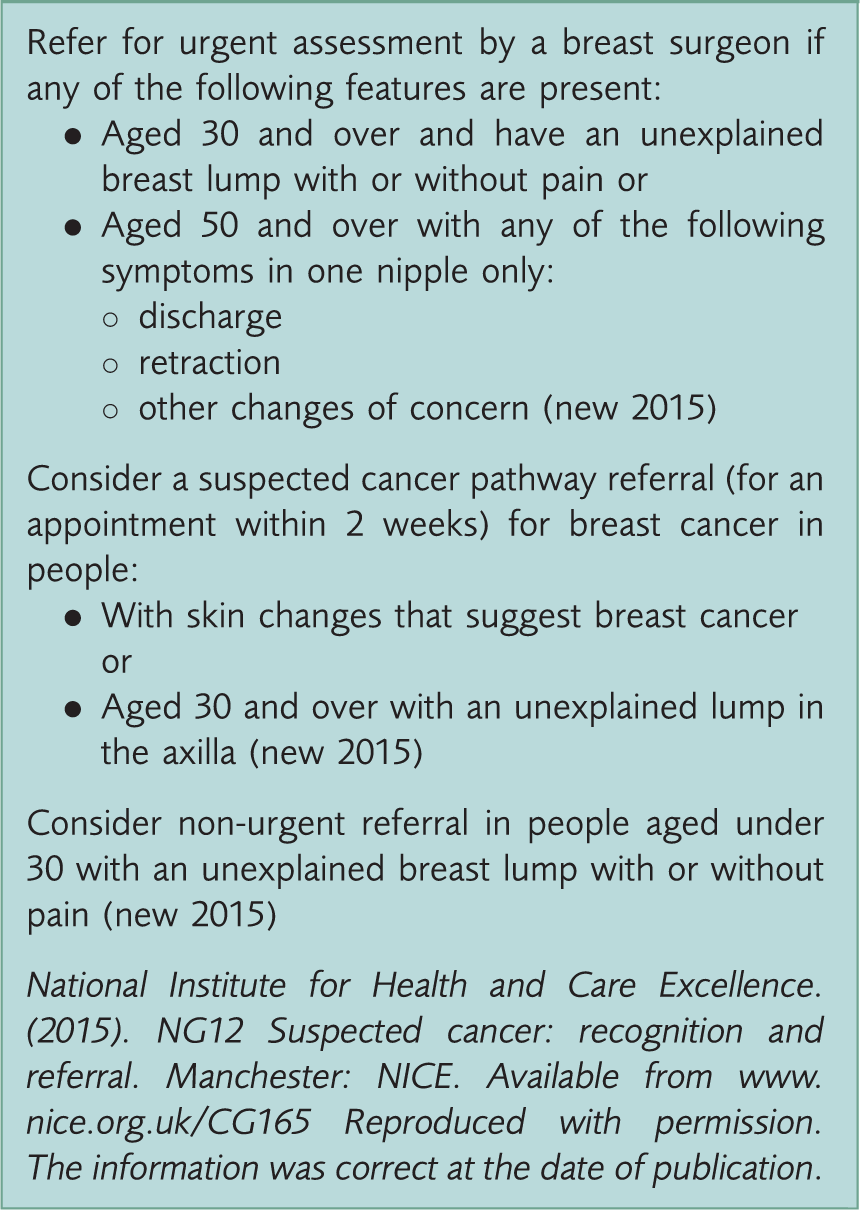
NICE symptoms for urgent referral of suspected breast cancer.
Referral and investigation of breast cancer
The new NICE guidelines recommend referral for those symptoms with a positive predictive value (PPV) for cancer of 3% or above, stating that at this level the advantages of rapid referral outweigh the disadvantages (NICE, 2014). Their cited research identified that any patient over the age of 40 years who presents to a GP with a breast lump has a PPV of more than 3% for breast cancer. The PPV increases proportionally with age, as one might expect. Below the age of 40 years, the PPV is under 3%; however, to simplify the criteria and avoid missing a diagnosis of breast cancer in patients with a less typical presentation, all referrals for breast symptoms must be seen by secondary care within 2 weeks of GP referral, regardless of whether they fulfil the criteria for urgent referral. This has spawned significant increases in referral rates to secondary care, however, it is hoped that this will translate into earlier diagnosis for the proportion of these patients who do indeed have breast cancer.
Despite the need for secondary care breast units to see all patients within 2 weeks of referral, it is recognised as helpful if those with suspected cancer can be discriminated from those thought to have benign conditions. This enables secondary care clinicians to see patients with suspected cancer in a clinic where radiological tests are immediately available (a one-stop clinic) and other referrals in a non-urgent clinic but still within 2 weeks, with radiology appointments booked subsequently.
It can be difficult for GPs to recommend referral for the ‘right’ symptoms, in order to minimise the number of people that in fact do not have breast cancer but are urgently referred; thus, also avoiding the creation of unnecessary anxiety for patients. The NICE guidance can help in identifying those who more likely to have cancer. Currently between 1 in 12, to 1 in 18 patients who are referred to breast clinics are diagnosed with breast cancer.
When a patient is seen in secondary care, following a clinical evaluation (history and examination), imaging (mammography and/or ultrasound) and pathological assessment (core biopsy or fine needle aspiration) are performed. This is termed triple assessment and is the diagnostic workup for all patients with breast lumps who are seen in secondary care.
Breast cancer management
Breast neoplasia is subdivided into two major categories: in situ disease, mainly in the form of ductal carcinoma in-situ (DCIS), and invasive breast cancer. Invasive breast cancer has the potential to spread throughout the body, whereas DCIS is restricted to the breast itself. Since DCIS is believed to eventually develop into invasive disease, it was felt that if breast neoplasia was identified and treated at the stage of DCIS, the prevalence of invasive breast cancer would decrease some years after. This has not happened and the incidence of invasive breast cancer and DCIS continues to increase in the UK.
The natural history of DCIS may differ dependent upon the grade of the DCIS (some DCIS is now thought not to develop into invasive cancer). This is now being studied through a UK randomised controlled trial of standard surgical treatment against active monitoring of impalpable low grade DCIS (LORIS trial).
The management of breast cancer is primarily surgical. This is either by wide local excision of the tumour (with a margin of healthy tissue) or mastectomy along with evaluation of the axillary lymph nodes. Further adjuvant management is with radiotherapy (to reduce the risk of local recurrence) or systemic therapy for distant disease control. The latter includes chemotherapy, hormonal therapy (for those tumours that are oestrogen receptor positive) and anti-HER2 therapy (for tumours that are HER2 receptor positive).
Other breast lumps
Differential diagnosis of breast lumps.

Fibroadenomas are benign growths of the stroma of the breast and are most commonly identified within the first two phases of breast growth. Patients with fibroadenomas will have a mobile rubbery mass on examination. The vast majority of fibroadenomas stay the same size or decrease in size. Diagnosis, as with any breast lump, is based on triple assessment in secondary care. Once they have been histologically confirmed, fibroadenomas may be removed or left in situ depending on the patient’s choice.
Phyllodes tumours are also growths of stromal tissue. However, they are less common and tend to occur in slightly older patients than fibroadenomas. They have a spectrum of cellularity, ranging from benign to frankly malignant and sarcomatous (these can metastasise). If a phyllodes tumour is diagnosed on triple assessment excision is recommended.
‘Lumpiness’ in the breast is common and may be labelled fibroadenosis, breast nodularity or fibrocystic disease. It may manifest as breast pain or discomfort, changes in global breast size, or lumpiness, and again is most commonly seen within the first two phases of breast growth. The cause is related to the glandular tissue of the breast responding to circulating female hormones, which may or may not be cyclical in nature. Breast pain is not a symptom typically associated with breast cancer but is frequently seen in patients with fibrocystic change.
Breast cysts are very common (affecting up to 7% of women (Haagenson, 1986)), and almost always benign. They may appear rapidly (they can appear in some patients overnight) and tend to be rounded and slightly softer than solid lumps. The diagnosis, as with all breast lumps, is made following triple assessment.
Cysts may be safely aspirated in secondary care. They are often recurrent and should be considered for excision if the same cyst repeatedly and rapidly refills. HRT not only predisposes to the development of breast cysts but also is a risk factor for the development of breast cancer if the duration of use exceeds 5 years.
Breast intraductal papilloma may be identified following a history of bloody single duct nipple discharge. They are benign and may produce a small periareolar lump and are most commonly seen in the second and third phases of breast growth. These require review in secondary care with triple assessment to confirm their nature and are usually treated with excisional biopsy.
Fat necrosis is usually the result of an injury to the breast, although the patient may report only minor trauma or have no recollection of an injury. It can be associated with breast discomfort and mild inflammation, but again may produce a breast lump. It is a diagnosis that is best made after cancer is excluded in secondary care.
Non-ANDI conditions include breast abscesses. These may develop as a result of pregnancy/breast-feeding (lactational) or in non-lactational women. The latter are typically seen in middle-aged women who smoke and have developed periductal mastitis. This is a chronic relapsing condition of the breast involving pain, redness around the nipple areolar complex, often with nipple discharge and sometimes inflammatory lumps and or abscesses and even fistulae and nipple inversion. Lactational breast abscesses are typically the result of Staphylococcus aureus infection, and present with focal pain, redness and swelling. Antibiotics and continued breast-feeding/expression of milk (in lactating women) is sensible initial management, however, urgent same-day referral to the emergency surgical team for ultrasound-guided aspiration is often the management of choice. All breast abscesses (that produce a lump) are best managed in secondary care, again following the principles of triple assessment
Diabetic mastopathy is an uncommon benign inflammatory process found mainly in (type 1) diabetics. It produces lumpy areas in the breast composed of fibrotic and inflammatory elements that are often painless. The pathogenesis of diabetic mastopathy is unknown; it requires triple assessment to exclude the presence of breast cancer (as for all lumps). The management, after exclusion of cancer, is non-operative, since there are high rates of recurrence after excision.
Finally, sebaceous cysts and lipoma may be identified in the breast. Once more the diagnosis of any lump in the breast should be made in secondary care, since even a diagnosis of atypical sebaceous cysts within the breast may truly be a breast cancer.
Breast pain
Most women will at some point experience breast pain (Dixon, 2006). It is not a symptom typically associated with breast cancer, particularly in women under 70 years in age.
Mastalgia is typically spontaneously resolving, but it is often recurrent and a nuisance, and in some women the pain may be severe. There are multiple theories with regard to the causation.
Management of breast pain follows a full history and careful examination. If a breast lump is found then onward referral through the standard pathway is essential. Generally, however, reassurance and recognition of the symptoms being real, benign and self-limiting is useful. Advice to establish that the patient is wearing the correct bra size is a good first step along with advice to stop smoking, and to reduce any consumption of red wine, caffeinated and coca products from the diet. Evening primrose oil has not been shown in randomised studies to significantly benefit patients, however, it has a strong placebo effect. In secondary care the use of tamoxifen, bromocriptine and danazol is occasionally employed.
Recommended web sites for further information.
Key points
Rapid referral under 2-week wait rules is appropriate for any breast lump and also other suspicious symptoms Breast lumps must be proven non-malignant by triple assessment in secondary care following urgent referral Breast cancer is increasing and up to one-in-eight women will develop the disease in their lifetime Breast pain is not a presenting feature of breast cancer