
Abstract
A common presentation to GPs is by patients with symptoms of scrotal pain, swelling and erythema. Some of these conditions have a benign cause, and therefore, can be managed in primary care. Other causes require urgent referral to secondary services for further investigation and management. The aim of this article is to enable GPs to be able to identify scrotal emergencies based on clinical presentation and examination findings. This will allow appropriate and timely referrals to be made, which will optimise patient care and subsequent outcomes. We discuss common presentations and their management based on suspected diagnosis.
The GP curriculum and scrotal emergencies
Make a sound diagnosis of scrotal emergencies in infants, children, adolescents and adults Refer appropriate cases to secondary care and manage the rest in the community Request appropriate investigations Judge final outcome at follow-up
Acute scrotal conditions (defined as scrotal pain, swelling and erythema) can be divided based on whether they affect paediatric or adult age groups. In all cases, it is essential that the GP thoroughly assesses the patient.
Take a thorough history. Establish the presence of pain, swelling and/or erythema and document the chronology, characteristic, severity and specific location of the pain. Remember to about any history of trauma, previous surgery and their sexual history. In all patients, it is important to elicit any constitutional symptoms: fever and rigor, nausea and vomiting, malaise and lethargy, and lower urinary tract symptoms (LUTS).
Next perform an initial general physical exam, which includes the abdomen and inguinal canal. A thorough examination of the scrotum should follow; looking for signs of infection or skin changes; testes, in particular their position, size and tenderness in comparison with each other; and finally epididymis - examined separately to testis if possible.
The following section of this article will outline potential causes of the patient’s symptoms; first dealing with paediatric patients and then adults. Primary care investigation and management and details on referral will be included in the specific disease sections. To aid with diagnosis, Fig. 1 outlines the scrotal anatomy.
Schematic representation of the layers of the scrotum - swelling in the skin or dartos layers may not be confined to one hemi-scrotum.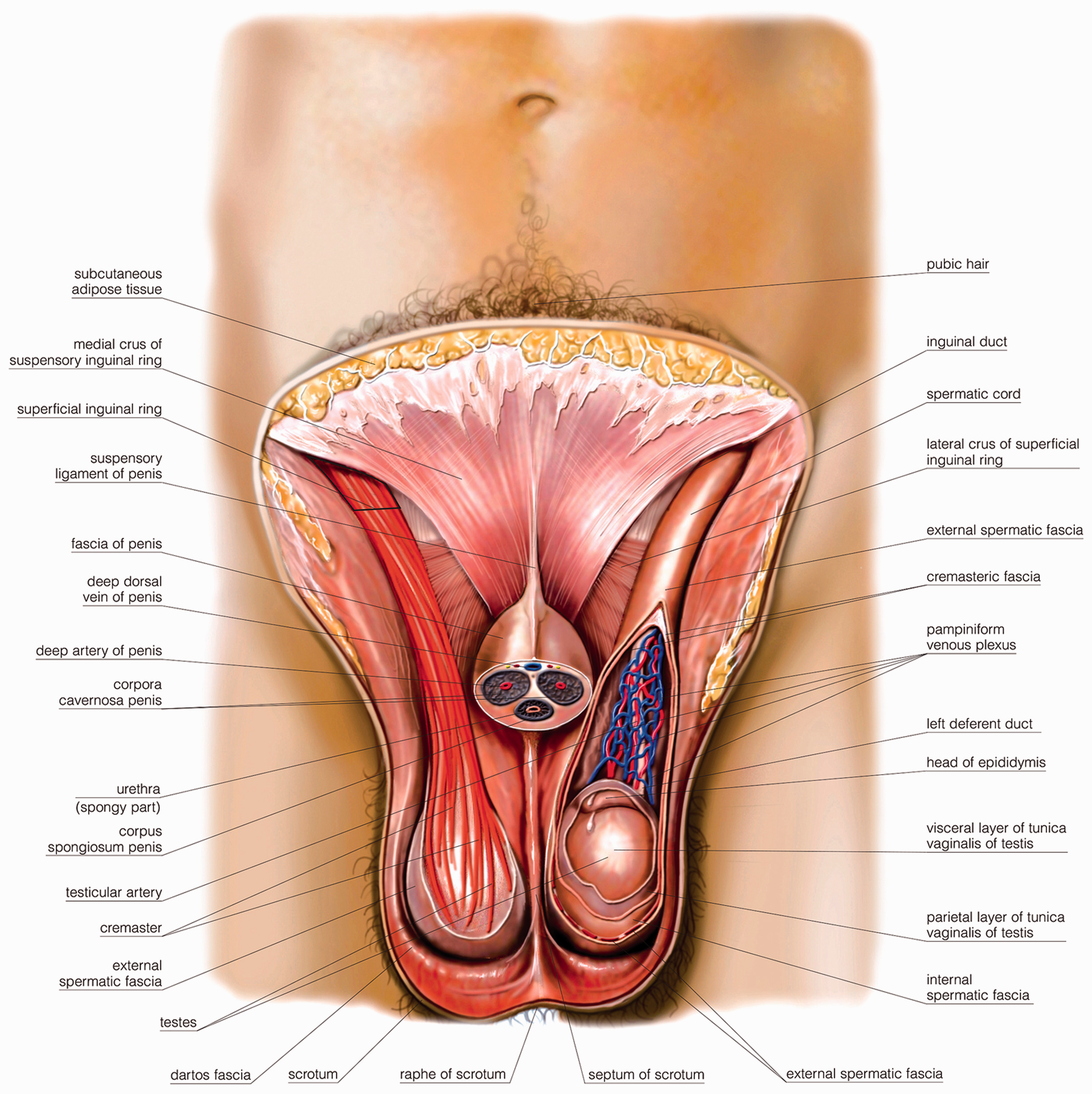
Paediatric
Acute idiopathic scrotal oedema
Qvist first reported the occurrence of an acute, but self-limiting, scrotal oedema that resolves with no lasting sequelae (Qvist, 1956). This is a condition predominantly seen in the younger age group. The presentation consists in redness of the scrotum, swelling and pain; generally in this chronology. The redness occurs in a very short period of time. The swelling, when closely observed, is not restricted to one hemi-scrotum, indicating a dartos, subcutaneous or skin problem as opposed to a testicular problem. Redness may extend into the perineum and the inguinal region, however, this is rare. Pain is present, but not severe. There are no constitutional symptoms, and examination will reveal no primary source of scrotal, perineal or peri-anal infection. The presentation is confusing and the diagnosis challenging in infants. Infants may present as a crying baby. An obstructed inguinal hernia is the differential and GPs should have a low threshold to refer for acute specialist assessment if unsure. Vomiting and refusal to feed is usually present in an obstructed inguinal hernia.
The aetiology of acute idiopathic scrotal oedema is not known, however, it is probably allergic in origin. It is the most common cause of the acute scrotum in boys under the age of 10 years (Najmaldin & Burge, 1987). The condition is self-limiting and resolves within 1–4 days (Klin, Lotan, Efrati, Zlotkevich, & Strauss, 2002). No imaging is required. Ultrasound scans can show clinically insignificant incidental findings, potentially leading to unnecessary exploration. Therefore, an ultrasound should not be used in preference to taking a good history (Breen, Murphy, Chow, Kieley, & O’Regan, 2013). If, as a GP, you are certain of this diagnosis, an explanation of the natural progression of the condition and likely outcome to the parents and child is essential in allaying anxieties and may avoid attendance at an Accident and Emergency (A&E) Department. However, it is important to provide safety netting advice to parents to seek medical attention if symptoms are worsening and, if you have any uncertainty about the diagnosis, refer for immediate specialist assessment.
Testicular torsion
Testicular torsion will be addressed in more detail in the section on adult presentation of an acute scrotum. Although rarer, paediatric testicular torsion should be considered in patients presenting with sudden onset of severe scrotal pain, often accompanied by nausea and loss of the cremasteric reflex on examination. It is important to note that younger children may not present with typical symptoms. For example, they may present just with abdominal pain or vomiting.
Anatomical anomalies, such as a bell-clapper deformity (in which the posterior anchoring of the testis, epididymis and gubernaculum to the vaginalis is incomplete), predisposes to testicular torsion (Schneck & Bellinger, 2007). Supravaginal torsion is more common in infants, with intravaginal testicular torsion being much more common overall, particularly within adolescents (Ciftci, Senocak, Cahit Tanyel, & Buyukpamukcu, 2004). If a GP has any suspicion of torsion in a child, immediate admission for paediatric surgical assessment is essential.
Hydatid torsion
In hydatid of Morgagni torsion, small appendages, which are the embryological remnants of the Müllerian and Wolffian ducts, undergo torsion and become ischaemic, thereby causing intense pain. Presentation is similar to testicular torsion. Due to the pain being experienced by the patient, the diagnosis might be made peri-operatively, as clinically, there is very little to differentiate between a torted testicle and a torted hydatid of Morgagni. It is, therefore, more likely to be an operative finding.
Often patients are referred acutely to secondary care to exclude acute testicular torsion. To establish a differential diagnosis, there are two important findings that may be apparent on examination: often the point of maximal tenderness is palpated directly above the testis and on transillumination a bluish tinge can be seen (known as the ‘blue dot sign’) (Günther & Rübben, 2012). Ultrasound may reveal a twisted hydatid structure located between the testis and epididymis (Sellers & Sidhu, 2003). Management of these cases is bed rest, cool compress and non-steroidal anti-inflammatory drugs (NSAIDs), with operative removal only considered in persistent, severe symptoms (Gatti & Patrick Murphy, 2007).
Mumps orchitis
Mumps is a contagious viral disease; its classic symptom is that causes swelling of the parotid gland. Transmission is via direct contact, airborne droplets and saliva. The introduction of the measles, mumps and rubella (MMR) vaccine in 1988 has led to a large decrease in overall reported incidence. However, 2003 saw a rise in both the number of reported and lab-confirmed cases, with over 90% of cases among those aged 15 and over. This rise in incidence is thought to be a combination of that cohort having had none or only one of the vaccines and a decline in the uptake of the MMR vaccine (Masarani, Wazait, & Dinneen, 2006).
In post-pubertal men with mumps, orchitis is the most common complication - seen in about 20–30% of cases (Bartak, 1973). Up to 30% are bilateral (Masarani et al., 2009). The virus attacks the testicular glands and causes inflammation of the parenchyma. The tunica albugenia acts as a barrier to oedema and causes an increase in intra-testicular pressure (Bartak 1973). Pressure-induced testicular atrophy may occur (Berhman, Kliegman, & Jenson, 2004). Presentation is characterised by testicular pain and swelling accompanied by malaise, myalgia, fever, nausea and headache. The testicular pain has an insidious onset and a rapid rise to a crescendo, as the intra-testicular pressure rises. Parotitis will always precede orchitis.
It is important to obtain a sexual history where appropriate. On examination, the scrotum is tender, oedematous and erythematous. In addition, there will be an initial enlargement of the testicle in the acute phase and enlarged epididymis in associated epididymo-orchitis. Treatment remains conservative with bed rest, use of NSAIDs and scrotal support. Steroids are useful in reducing pain and swelling, however, they do not alter the clinical course. There is currently no convincing evidence for the use of antibiotics in these cases (Masarani et al., 2006). Impact on fertility is still of great concern in those patients suffering from orchitis, with an estimated 30–87% of patients with bilateral symptoms becoming infertile (Casella, Leibundgut, Lehmann, & Gasser, 1997). Data regarding the use of systemic interferon to inhibit viral replication, and hence, testicular atrophy and infertility, has produced mixed results (Masarani et al., 2006) and is not currently recognised in the treatment of mumps orchitis.
Herniae
Although not a scrotal emergency, herniae may present as acute scrotal pain. During fetal development an out-pouching of the peritoneum, the processus vaginalis, follows the testicle, attached posteriorly, as it descends into the scrotum. An inguinal hernia can occur when obliteration of this tract fails (Brandt, 2008). Generally a child with an inguinal hernia presents with parents who have noted an obvious bulge at the internal or external ring or scrotum. Commonly, there is no obvious associated pain and parents may note that it appears after straining or crying, but resolves while the child is sleeping. It is more common to see right-sided indirect hernias (60%) due to delay in the descent of the right testicle during development (Hebre, 2014).
Consider obstruction and strangulation when the parents provide a history of a painful bulge, often accompanied by a child who refuses to feed and cries inconsolably. Examination reveals a tender, non-reducible firm mass with oedema and erythema of the overlying skin. In these cases, urgent referral to the paediatric surgical team is warranted.
Adult
Trauma
Trauma to the scrotum is often blunt and due to direct trauma, for example, sporting injuries, fights or road traffic accidents. The mobility and anatomical location of the scrotum means that it accounts for less than 1% of all trauma-related injuries (Deurdulian, Mittelstaedt, Chong, & Fielding, 2007). In these instances, an accurate history, knowledge of progression of symptoms, and a thorough physical exam are essential when differentiating between those cases where conservative management is appropriate and those requiring surgical intervention. Patients will often present with acute pain, swelling and obvious haematoma to the area. Scrotal wall abrasions or small superficial haematomas can be managed conservatively with symptomatic relief (Srinivaso Rao & Arjun, 2012). Anything more severe needs further assessment by a specialist urologist. Historically, all patients were surgically explored, as there was no well-defined method of determining the level or extent of damage. Today, high-resolution ultrasound with Doppler colour flow is the investigation of choice (Srinivaso Rao & Arjun, 2012). Nevertheless, this relies on the sonographer being familiar with the appearance of common scrotal injuries.
Injuries such as traumatic hydroceles, haematoceles, epididymal injuries and intra-testicular haematomas can all be identified on ultrasound; however, the injury presenting a threat to testicular survival is testicular rupture. Only imaging will reveal a disruption to the tunica albuginea and presence of testicular contents in the scrotal sac - warranting urgent surgical exploration. Buckley and McAninch (2006) demonstrated a sensitivity of 100% and specificity of 93.5% in the use of ultrasound for detecting rupture to the tunica albuginea.
Testicular trauma is an urgent clinical situation, as opposed to an emergency. If a case presents itself outside of working hours, the ultrasound scan can be performed first thing the following morning. There is considerable variability in access to urgent ultrasound scanning across the country in the community; therefore, the investigations might need to be undertaken in secondary care. If in doubt, speak to the urology specialist who is on call. However, due to the possibility of antisperm antibody production secondary to trauma, a delay of more than 24 hours is not advisable.
Torsion
Characteristic features in torsion compared with those for epididymo-orchitis.

Eliciting key features from the history is essential, as is establishing the temporal course of symptoms, particularly pain (see Fig. 2). The presenting complaint is a sudden onset of severe pain, often accompanied by vomiting. The patient remains systemically well and does not report lower urinary tract symptoms (LUTS). On examination, the tender testicle can be palpated high in the scrotum, due to shortening of the cord, and there may be associated loss of the cremasteric reflex (Günther & Rübben, 2012). In these instances in the acute phase, if torsion is clinically suspected, then immediate referral to the appropriate surgical team is warranted - ultrasound is not indicated and must not delay the patient from emergency surgical exploration. In 2006, a review reported successful salvage of the testicle in 90% of patients at 6 hours, in comparison with just 10% at 24 hours (Ringdahl & Teague, 2006). Once delayed beyond 6 hours, the rationale for urgent surgery becomes less apparent, largely due to the pathophysiology of torsion.
Temporal representation of pain severity in torsion compared with that for epididymo-orchitis.
Torsion of the testicle is essentially a non-infective vascular event. It follows the pathology principles of other avascular events such as myocardial infarction and cerebrovascular accident. If re-vascularisation is not achieved within 4–6 hours after the start of the event, an inflammatory response starts with the invasion of macrophages and later by fibroblast. Twenty-four hours later the pain is usually significantly reduced and tolerable. The pain completely subsides within 2 to 3 days when the process of fibrosis starts. In 3 weeks, the testicle is small, non-tender, and has a woody feel. There is no infective process, and therefore no intervention is required, however, it is presumed that the same anatomical abnormality exists on the opposite side, and therefore an elective fixation of the opposite side is essential. The torted testis can be left in situ, as it is believed that it may still retain its hormonal function.
Epididymo-orchitis
Patients who you suspect have epididymo-orchitis should still be assessed carefully, and clinicians should always have a low threshold for excluding testicular torsion. A sexual history is required when considering management options. Patients often present with acute scrotal pain, but further questioning will reveal a more insidious onset over the preceding few days, with non-specific constitutional symptoms such as malaise and lethargy. It is much more likely that they will complain of fever and LUTS and GPs should be aware of patients who may be more susceptible to becoming acutely unwell, such as those with diabetes or who are immunocompromised. Patient factors determine likely causative organism as stated in guidelines by the British Association for Sexual Health and HIV (British Association for Sexual Health and HIV (BASHH), 2010): In sexually active adolescents and men younger than 35 years of age, the causative organism is likely to be Chlamydia trachomatis or Neisseria gonorrhoea. In men 35 years or older and adolescents and men younger than 35 years of age who are not sexually active, the causative organisms are typically enteric organisms found in lower urinary tract infections, such as Escherichia coli.
Patients should have their progress monitored and be advised to seek advice if symptoms do not begin to improve within 3 days of commencing treatment. All should be followed up at 2 weeks - this is to assess adherence to treatment and improvement of symptoms. In those who have a confirmed STI, contact tracing needs to be discussed, this is usually coordinated by a sexual health specialist. In those who have a urinary tract infection confirmed, consider the need for a referral to urology as an outpatient for investigation - current guidelines state that these patients are more likely to have functional or anatomical abnormalities of the urinary tract (BASHH, 2010).
Advice to patients should stress the fact that with the best available antibiotics, 95% will show evidence of improvement within 48 hours. A few patients may not respond and the inflammation will change to an intra-testicular abscess. Pain, swelling and fever will increase. An ultrasound scan is required to confirm formation of an abscess and the correct treatment then is an orchidectomy. It is, therefore, good practice to organise an ultrasound scan and a review in 3 to 4 weeks from the onset of epididymo-orchitis.
Key points
A detailed history, with emphasis on the temporal course of events and characteristics of pain is essential when trying to establish a diagnosis in a patient presenting with acute scrotal pain Ultrasound is not recommended for the emergency differentiation between torsion and epididymo-orchitis In cases of testicular torsion of greater than 12 hours duration, in a systemically well patient, emergency surgical intervention is not always clinically indicated and the acute surgical team may opt to manage the patient conservatively An ultrasound scan and follow-up at 3 to 4 weeks after the onset of initial symptoms is recommended