
Abstract

Aetiologies of B12 deficiency.

Not all causes of B12 deficiency require IM injections and some patients may be managed using oral cyanocobalamin tablets, an approach supported in recent guidelines on a low vitamin B12 (Devalia, Hamilton, Molloy, 2014). In order to identify whether a patient is suitable for oral B12 replacement, the cause of their deficiency must first be investigated. Without investigation there is a risk that patients will be routinely started on hydroxocobalamin injections, subjecting them to life-long invasive procedures when oral replacement may be adequate. I have audited patients of York Medical Group (YMG) to identify whether the cause of a low serum B12 has been appropriately investigated before starting long-term IM injections.
Set standards
The standards audited against were the recommendations of the British Committee for Standards in Haematology (BCSH) (Devalia et al. 2014), as follows:
All patients with anaemia, neuropathy or glossitis, and suspected of having pernicious anaemia, should be tested for anti-IFAB (anti-intrinsic factor antibodies) regardless of cobalamin levels. Patients found to have a low serum cobalamin level in the absence of anaemia and who do not have food malabsorption or other causes of deficiency, should be tested for anti-IFAB to clarify whether they have an early/latent presentation of pernicious anaemia. Anti-GPC (anti-gastric parietal cell antibody) testing for diagnosing pernicious anaemia is not recommended.
These recommendations encompass the need to test for anti-IFAB when the diagnosis of pernicious is being considered. Unless there are other clear causes of a low serum B12 requiring IM injections, patients should not be on injections unless anti-IFAB has been tested.
Design
A cohort of patients were identified who were due to attend for a B12 injection between 14th September and 11th October 2015. Patients were excluded from audit if they had a clear cause of deficiency, other than pernicious anaemia, that required IM injections. The medical notes of the remaining cohort were analysed to ascertain whether they had been tested for anti-IFAB or anti-GPC.
Results
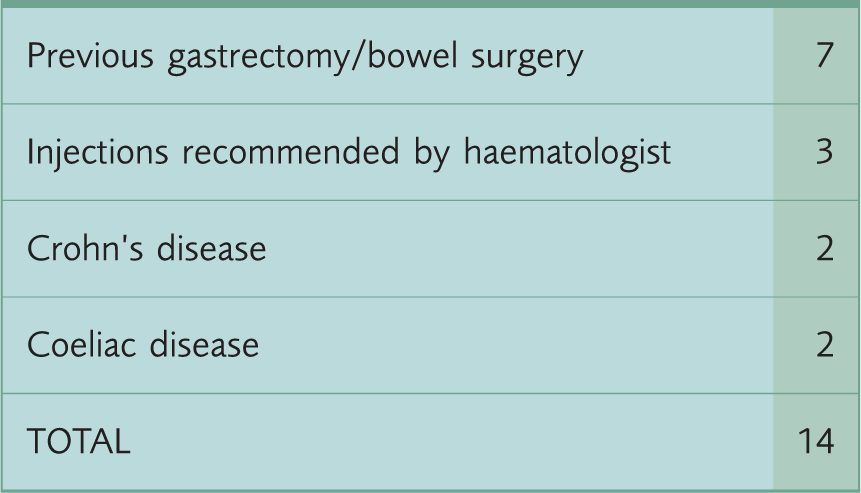
There were 81 patients due to have an injection of hydroxocobalamin between 14th September and 11th October 2015. Of these, 14 patients were excluded due to a pre-existing clear cause of B12 deficiency (see table 1), leaving 67 patients in the audit. Of these 67 patients, 25 had been tested for anti-IFAB and 26 had been tested for anti-GPC; 13 had been tested for both antibodies. 29 patients had not been tested for either anti-IFAB or anti-GPC (see figure 1).
Demonstrating auto-antibodies tested in patients receiving IM hydroxocobalamin. Demonstrating reasons for exclusion from audit.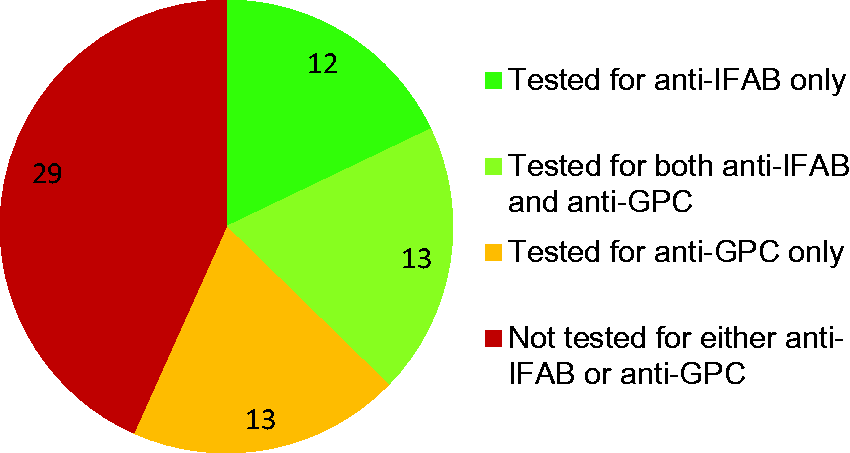
Findings
57% of patients had been tested for auto-antibodies before starting IM injections, but often not in accordance with BCSH guidance. A significant proportion (43%) of patients receiving injections had not been investigated for auto-antibodies.
Discussion
Reflecting on these findings, I do not believe that doctors are fully aware of the reasons behind anti-IFAB testing and its importance in B12 deficiency management. There are 377 patients registered with YMG receiving IM hydroxocobalamin injections, whilst only 5 are receiving oral cyanocobalamin. I worry that a proportion of these patients may be suitable for oral cyanocobalamin replacement and so I feel that it is important to raise awareness of the recent BCSH guidelines and the principles behind them. There are a number of factors that can contribute to a patient being unnecessarily started on IM B12 injections, and I will cover some of them here.
Serum B12 levels: a reliable investigation?
A ‘serum B12 level’ is the widely-used standard measure of a patient’s B12 state but it does not have the sensitivity nor specificity to be used as a robust diagnostic test in isolation. A serum B12 less than 200 ng/L has a 95% sensitivity of detecting a true B12 deficiency but a specificity of only 50%; a serum B12 less than 150 ng/L is more specific but has a sensitivity of only 75% (Devalia et al. 2014). This means that a serum B12 less than 200 ng/L is unlikely to miss a true B12 deficiency but will have a high false-positive rate, whereas a serum B12 less than 150 ng/L is likely to identify true deficiencies but with a higher false-negative rate. B12 levels are best interpreted in the context of the clinical picture – commencing treatment in an asymptomatic patient with a marginally low B12 level would not be appropriate without further investigation. However it would be acceptable if the same patient presented with glossitis and neuropathy.
Adjuncts to a low serum B12 level
Given the difficulty in interpreting ‘indeterminate’ serum B12 levels between 150 ng/L and 200 ng/L, there are supplementary tests that can be considered to aid diagnosis. ‘Plasma total homocysteine’ (tHcy) and ‘plasma methylmalonic acid’ (MMA) are both biomarkers detectable in the blood that are raised in vitamin B12 deficiency and can be requested, where available, when there is clinical suspicion of deficiency but an indeterminate serum B12 level. Holotranscobalamin (HoloTC) is the ‘active’ form of serum vitamin B12. Currently it is measured in combination with ‘inactive’ serum B12 to provide a ‘serum B12 level’. It is possible to measure the level of HoloTC alone and is thought to have better sensitivities and specificities than current ‘serum B12 levels’ but more studies are required before its application in clinical practice (Devalia et al. 2014). HoloTC does represent a future diagnostic test that may hopefully reduce the number of patients inappropriately started on B12 replacement.
Starting treatment
When faced with diagnostic uncertainty it may be difficult to decide when to initiate life-long B12 replacement. Given the risk of neurological impairment associated with vitamin B12 deficiency, IM hydroxocobalamin should not be delayed when there is strong clinical suspicion of deficiency (ie. glossitis, neuropathy, anaemia). In patients where serum B12 levels have been tested in the presence of non-specific symptoms, guidelines recommend investigating and managing as pernicious anaemia when the serum level is below 150 ng/L. This leaves a group of patients who present without strong clinical evidence of deficiency but an indeterminate serum B12 level between 150 ng/L and 200 ng/L. For these patients, guidelines recommend repeating blood tests in 1–2 months, after which a proportion of patients will have normal levels. For those with an indeterminate level after 2 months, anti-IFAB should be tested, and if negative, a 4 week trial of oral cyanocobalamin 50micrograms daily can be given, with repeat bloods taken in 3–4 months. If serum B12 rises above 200 ng/L then food-bound cobalamin malabsorption is a leading differential diagnosis and life-long oral cyanocobalamin therapy may be needed. If levels remain intermediate, tHcy or MMA can be tested to confirm a true deficiency, but these patients may need to be treated with injections as antibody-negative pernicious anaemia (Devalia et al. 2014).
Importance of appropriate B12 management
There is no denying the benefit of IM injections - irrespective of aetiology they replenish vitamin B12 stores without the need for monitoring. Injections are however an invasive procedure and carry risks of injection site reactions and infection. They are also uncomfortable and are distressing for patients with cognitive decline unaware of their need, a genuine issue given the rise in B12 deficiency (Andres et al. 2008) and dementia with advancing age. Importantly, B12 injections are administered by trained doctors or nurses; taking oral replacement empowers patients to manage their own medical condition. Financially, both treatments carry similar costs; the annual price of cyanocobalamin is £65.63 compared with £9.64 for a year of hydroxocobalamin injections (Joint Formulary Committee, 2015), but this does not factor in nursing time required to administer injections, which impacts not only financially but on time available to spend managing other chronic conditions.
Conclusion
This audit has highlighted that we can improve our practice by following guidance on investigating patients with a low serum B12, as patients are often started on IM injections without prior diagnostic tests. Patients who could be managed with oral cyanocobalamin supplementation are not being identified which impacts not only on patients’ quality of life but also the resources that the practice has to offer. I plan on re-auditing in 6 months’ time to ensure new patients started on IM hydroxocobalamin have been tested for anti-IFAB, and that we are no longer testing for anti-GPC.