
Abstract
Elder abuse is prevalent and, as the population ages, it is likely to be a growing problem. It frequently goes unrecognised, but is often devastating and sometimes fatal to the victim. It is considered to be both under-funded and under-researched, but early recognition of those at risk and intervention in the primary care setting can reduce harm and sometimes prevent elder abuse occurring entirely.
The GP curriculum and elder abuse
Recognise abuse (emotional, mental and physical) in the elderly and deal with it appropriately Be wary of possible neglect or abuse of the elderly Understand the legal and ethical issues that may arise, e.g. regarding confidentiality, the Mental Health Act, the Mental Capacity Act, power of attorney, court of protection applications, guardianship, living wills Understand the physical, psychological and social changes that may occur with age and relate them to the adaptations that an older person makes, and to the breakdown of these adaptations, e.g. when hearing, vision or cognitive function continue to worsen Ensure that the provision of care promotes the patient’s sense of identity and personal dignity, and that the patient is not discriminated against as a result of their age Recognise the importance of a problem-based approach, taking in the ‘big picture’, rather than a disease-based approach to the care of older people, who often have complex physical, psychological and social problems
What do we mean by elder abuse?
The charity ‘Action on Elder Abuse’ defines abuse as ‘a single or repeated act or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person' (Action on Elder Abuse, 2015). Essentially, older people are subjected to all the forms of abuse seen in other adults, but are at greater risk, due to the higher prevalence of physical illness and cognitive impairment (see Fig. 1). The physical, psychological and social changes that occur with age also mean that abuse can present differently to abuse seen in a younger adult or child, but has equally wide-reaching consequences. Older people who are abused have higher rates of physical and mental health problems, reduced survival rates (even compared with those who suffer from self-neglect), higher rates of institutionalisation, along with suffering the loss of money or possessions seen in financial abuse (Cooper & Livingston, 2009). Although still devastating, in some cases the abuse is not intentional and occurs because the perpetrator lacks the skills or support to care for the victim. Ill-treatment or neglect can be punishable with a prison sentence of up to 5 years.
Types of elder abuse.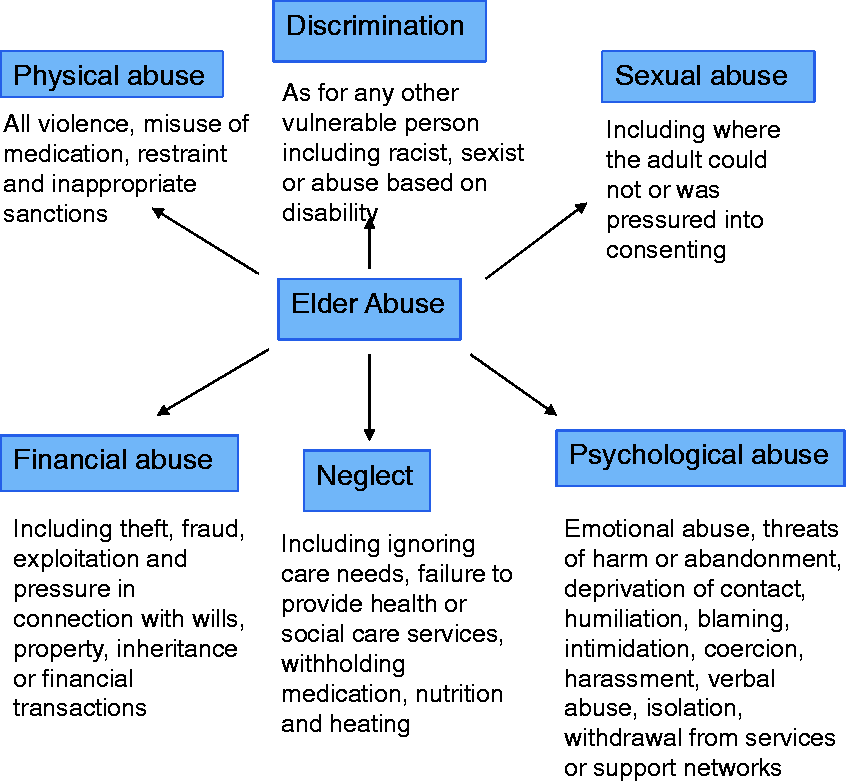
Elder abuse is common and under-reported
Elder abuse is difficult to research, as victims often have cognitive impairment or communication difficulties, are too frightened or embarrassed to admit to being abused, or feel they depend on the perpetrator. Even when abuse is seen it is not always recognised, or barriers, such as reluctance to whistle-blow or the misguided belief that a threshold for intervention is not met, mean that it goes unreported. The prevalence is therefore difficult to quantify and figures vary depending on definitions, study methods and country of research. A large UK survey of older adults without cognitive impairment and living in their own homes found that 4% reported abuse in the past year. This equates to roughly 342 400 people across the country (Department of Health & Comic Relief, 2007). Furthermore, a large systematic review showed that the rates are much higher in more vulnerable older people. They found that nearly a third of family caregivers reported significant abuse towards their relatives with dementia, with 5% admitting to physical abuse. They also found that 16% of care home staff reported significant psychological abuse towards residents (Cooper, Selwood, & Livingstone, 2008). Only a fraction of these episodes are reported. The Health and Social Care Information Centre reported that in 2014–15, there were only 103 900 UK adult safeguarding referrals, of which 63% were for adults aged 65 years or over (Health and Social Care Information Centre, 2015).
Who perpetrates elder abuse?
The abuser is often well-known to the person being abused, commonly being a family member, friend or paid carer. Those inflicting abuse are usually exploiting a position of trust. The type of perpetrator varies depending on the type of abuse. For example, close family members are more likely to perpetrate psychological or physical abuse, and whereas most financial abuse is still perpetrated by family members, it is more likely than other types to involve friends, neighbours or distant relatives (Cooper and Livingston, 2009).
Abuse by families
Being a carer (family or paid) can often be physically and emotionally demanding; those carers who feel stressed are more likely to physically or psychologically abuse those for whom they provide care. Conversely, some carers may be caused harm by the person to whom they are providing care. This may be intentional, but in other cases it is caused by the disability itself, for example, in patients with dementia. Although rates of domestic violence do reduce with age, sometimes the elder abuse is actually a continuation of a long-term abusive relationship, or an abusive partner can become the victim if they become dependent on the person they previously abused (Cooper and Livingston, 2009). The pattern of abuse can be complex, two-way and of several types (Local Government Association, 2015).
Abuse by professionals
Abuse by professionals often goes unreported, due to staff not recognising it, empathising with the perpetrators, not knowing how to report, or fear of recrimination if they do make a report (Kitchen, Richardson, & Livingston, 2002). Only 5% of older people live in care homes, but they make up 23% of the callers to the Action on Elder Abuse Helpline (Action on Elder Abuse, 2015). Health and social care staff were the alleged perpetrators in nearly a third of abuse referrals to social services (Cooper & Livingston, 2009). This abuse, although never excusable, can sometimes be unintentional, as a result of factors such as inadequate care worker time or poor training in the management of challenging behaviour. For example, use of medication to sedate a patient may constitute a form of elder abuse if drugs are not prescribed in the patient's best interests. The unnecessary use of antipsychotic drugs has reduced significantly over the past decade, but prescription without regular review and ongoing psychotic symptoms can also be abusive (Health and Social Care Information Centre, 2012). This is because it puts the person at an increased risk of stroke and overall mortality (Cooper and Livingston, 2009).
The deprivation of an individual's liberty (for example, by the use of a keypad lock to prevent wandering in a care home) can be abusive and, if the proper assessments are not carried out, it is a breach of Article 5 (Right to Liberty) under the European Union Convention on Human Rights. Where this is required to keep the patient safe, the local authority has a responsibility to carry out a Deprivation of Liberty Safeguards Assessment to decide on the correct action. This can only be applied in care homes and hospitals: patients living in their own homes cannot be legally deprived of liberty without the authority of the Court of Protection (Age UK, 2015a).
Who is most at risk?
Abuse can take place in any context, but there are some characteristics of patients and their carers that can help identify those older people at greater risk. Recognition and early intervention with patients and carers at risk may be enough to prevent problems ever occurring.
Patient factors
Any factor that leaves older people less able to protect themselves, to leave the situation, to ask for help or to report abuse puts them particularly at-risk. This is especially the case for people with cognitive impairment, where loss of capacity to make decisions puts them at the mercy of others. It also includes people with physical illness, communication difficulties, social isolation or a lack of access to health services, and those with mental health problems. People with feelings of low self-worth or a prior history of abuse, even as a child, are particularly at-risk; this is especially true if they have negative experiences of reporting abuse in the past. It is not entirely clear why those from lower socio-economic backgrounds have higher rates of elder abuse, but this may be partly as a result of higher detection rates, due to more social services contact (Cooper and Livingston, 2009). Unsurprisingly, the presence of multiple factors increases the risk. A recent North American study showed that compared with older people with no risk factors, older adults with three or four vulnerability factors (see Fig. 2) have four times the risk of being abused and those with five or more factors are at more than 26 times the risk (Dong & Simon, 2014).
Vulnerability index factors that identified individuals at risk of elder abuse in a US study of patients living in the community.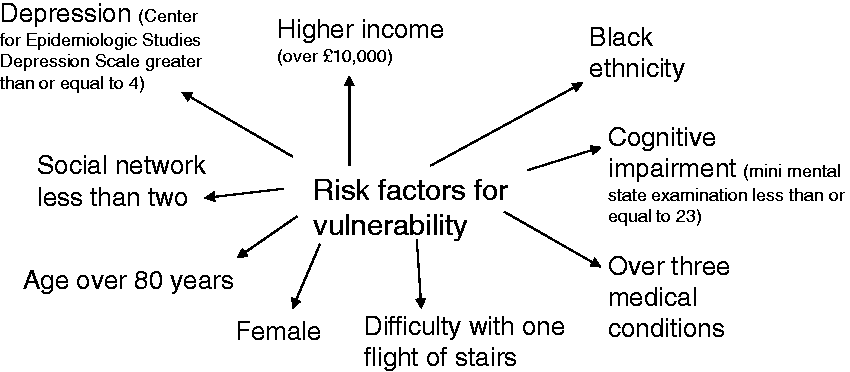
Carer factors
Some characteristics make carers more susceptible to becoming a perpetrator of abuse. Those who are overworked and live with the person for whom they provide care services are at higher risk, especially if they resent their caring role. Mental health problems in the carer, such as anxiety, depression, stress and drug or alcohol use, also increase the risk, as does a carer's personal experience of being an abuse victim. The older person is at high risk if there is a breakdown in the relationship, for example, as a result of abusive behaviour by older people towards their carers (Cooper and Livingston, 2009).
Similar characteristics of unsatisfactory relationships, difficult communication and substance misuse can also make the older carer more susceptible to becoming a victim of abuse. Likewise, overworked carers are at-risk of becoming abused, especially where the person being cared for does not consider their needs, treats them with a lack of respect and resents the situation. Clearly, carers looking after patients with conditions causing abusive, aggressive or frightening behaviours are at higher risk of becoming victims. It is also important to recognise that the carer is at higher risk if the person being cared for refuses to be left alone (by day or night), has rejected help and support from outside agencies or has sought help, but not met the thresholds for this provision. Carers are also at increased risk where the person being cared for has control over financial resources, property and living arrangements (Local Government Association, 2015).
What are the symptoms and signs of elder abuse?
Older people may report abuse directly, but it is easily missed and it is good practice to routinely inquire about risk factors for elder abuse in a non-judgemental way. Even when perpetrators realise the legal and other implications, they sometimes admit to the abuse because they want to access help in order to stop. The Modified Conflict Tactics Scale is a set of 10 questions that can be used with older people or family carers to identify and quantify abuse. It asks about verbal abuse, threats to send into care or abandonment, fear of or actual physical abuse, and food withholding in the last 3 months (Cooper and Livingston, 2009).
Where the older person does not or cannot report the abuse, there are a number of factors that should raise suspicions (Fig. 3). Unexplained injuries or gross neglect should be unmissable, but signs may often be more subtle, especially without a holistic understanding of the patient and his or her social circumstances. For example, the patient might display changed behaviour, becoming scared or more withdrawn, or during a home visit, there might be signs to suggest financial difficulties and lack of money to buy essential items. The home situation may be unsafe, e.g. some well-meaning relatives may leave an older person locked in the home (so they could not get out even in an emergency), which will constitute a deprivation of liberty. It can sometimes be difficult to differentiate between neglect and the person who is refusing care, because features such as poor hygiene, pressure sores, dirty clothes and malnourishment, are common to both.
Signs of elder abuse.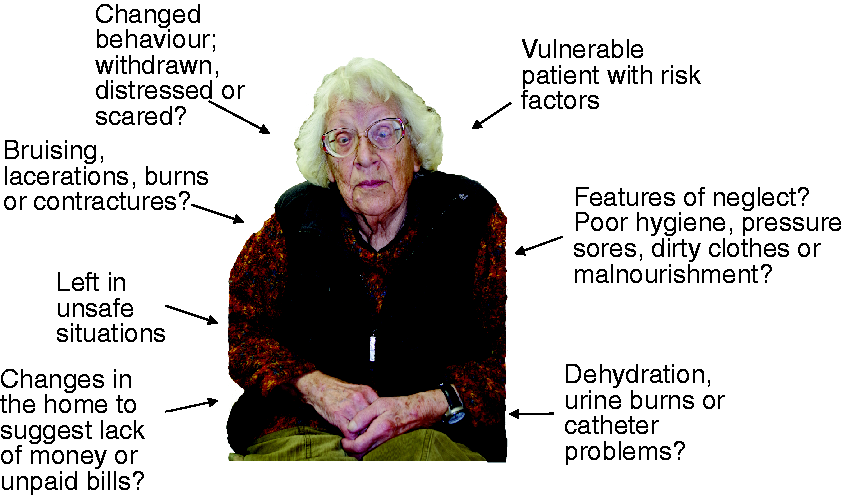
A full examination is essential in all cases of suspected abuse in order to identify any bruising or lacerations (including those about the genitals, rectum or mouth in sexual abuse), signs of malnutrition and dehydration or urine burns. It is important to remember that unexplained catheter problems can be a sign of sexual abuse, as can genitourinary infections.
I suspect elder abuse: What should I do now?
The Care Act 2014 means that all professionals have a responsibility to do their best to ensure that an older person is protected from any risk of abuse or neglect (Age UK, 2015a). It is best (although not always possible) to discuss your concerns with the older person. This can be challenging, and it is paramount that the person is interviewed without the abuser present and allowed to be accompanied by a trusted person if he or she wishes. As with all allegations of abuse, it is vital that vulnerable people are given support to express themselves and that it is explained what will happen to any information disclosed. The details of the consultation must be recorded clearly and accurately in the patient records. There are several organisations that support older people suffering from abuse and their families. The charities ‘Action on Elder Abuse’ and ‘Age UK’ both have free helplines, excellent websites that provide information for patients, families and professionals, and other support for victims such as ‘buddies'.
When is it right to intervene?
Defining elder abuse can be difficult and it is generally felt that the behaviour has to reach a threshold of severity or frequency to be abusive. For example, it probably would not be abusive for a carer to shout at an older person on a single occasion, but if this happened on a regular basis then the behaviour may be abusive. It is not uncommon for people caring for an older person (whether professional or family) to disagree as to whether behaviours constitute abuse, and as a trainee, all potential cases of abuse should be initially discussed with your clinical supervisor and the practice adult safeguarding lead.
It is also important to remember that the full extent of abuse is often not initially apparent so, if a patient or carer reports abuse, or you feel the patient may be at risk of harm, then it is right to intervene and make a referral to the local authority multi-agency safeguarding services. The General Medical Council summarises this saying that: You must take prompt action if you think that patient safety, dignity or comfort is or may be seriously compromised … Whether or not you have vulnerable adults or children and young people as patients, you should consider their needs and welfare and offer them help if you think their rights have been abused or denied (General Medical Council, 2013).
The Care Act 2014 means that the local authority has a legal duty to ‘make enquiries' where there is reasonable cause to suspect either that an adult with care and support needs is being abused or neglected, or is at risk of being abused or neglected (Age UK, 2015a).
Interventions should always be part of a person-centred approach that involves older people and aims to empower them to be in control of their lives as much as possible. Patient safety is paramount, and the first priority should be to ensure the older person is in a place of safety, followed by referral to the local authority for assessment. In serious cases, if there is evidence of a crime, then direct referral to the police can increase the likelihood of conviction. Unfortunately, there is no agreed definition of what constitutes a serious offence and professional judgement is required.
The Department of Health document ‘Confidentiality: NHS Code of Practice' describes serious crimes as including murder, manslaughter, rape, child abuse and crimes that involve substantial financial gain or loss. It advises that theft, fraud and damage to property where loss or damage is less substantial are crimes that are not usually serious enough to warrant disclosure to the police without patient consent (Department of Health, 2003). Deliberate physical assault or imprisonment may also be considered as serious crimes and ill-treatment or wilful neglect of someone who lacks the capacity to care for him or herself is a crime under the Criminal Justice and Courts Act 2015 (Age UK, 2015a). If you feel an offence does require reporting to the police, it is crucial to clearly explain to the patient that confidentiality must be broken and why this is necessary. It is advisable to discuss your planned actions with your medical defence organisation.
All adults with capacity have the right to make decisions about their own care and treatment, and some older people refuse referral. In these cases, it is important to attempt to understand the reasons for the refusal and to offer alternative support as available. It is also important to assess the person’s capacity to make this decision, while respecting the person’s right to make an ‘unwise' decision if he or she has capacity to make it. When the older person does not have capacity, and all has been done to allow that person to demonstrate this, then GPs should act in the patient's best interests. Even in circumstances where the older person has the capacity to refuse referral, it may still be necessary to break confidentiality (Fig. 4), especially if a serious offence has been committed or other vulnerable people are at risk.
What happens if my patient refuses referral to social services?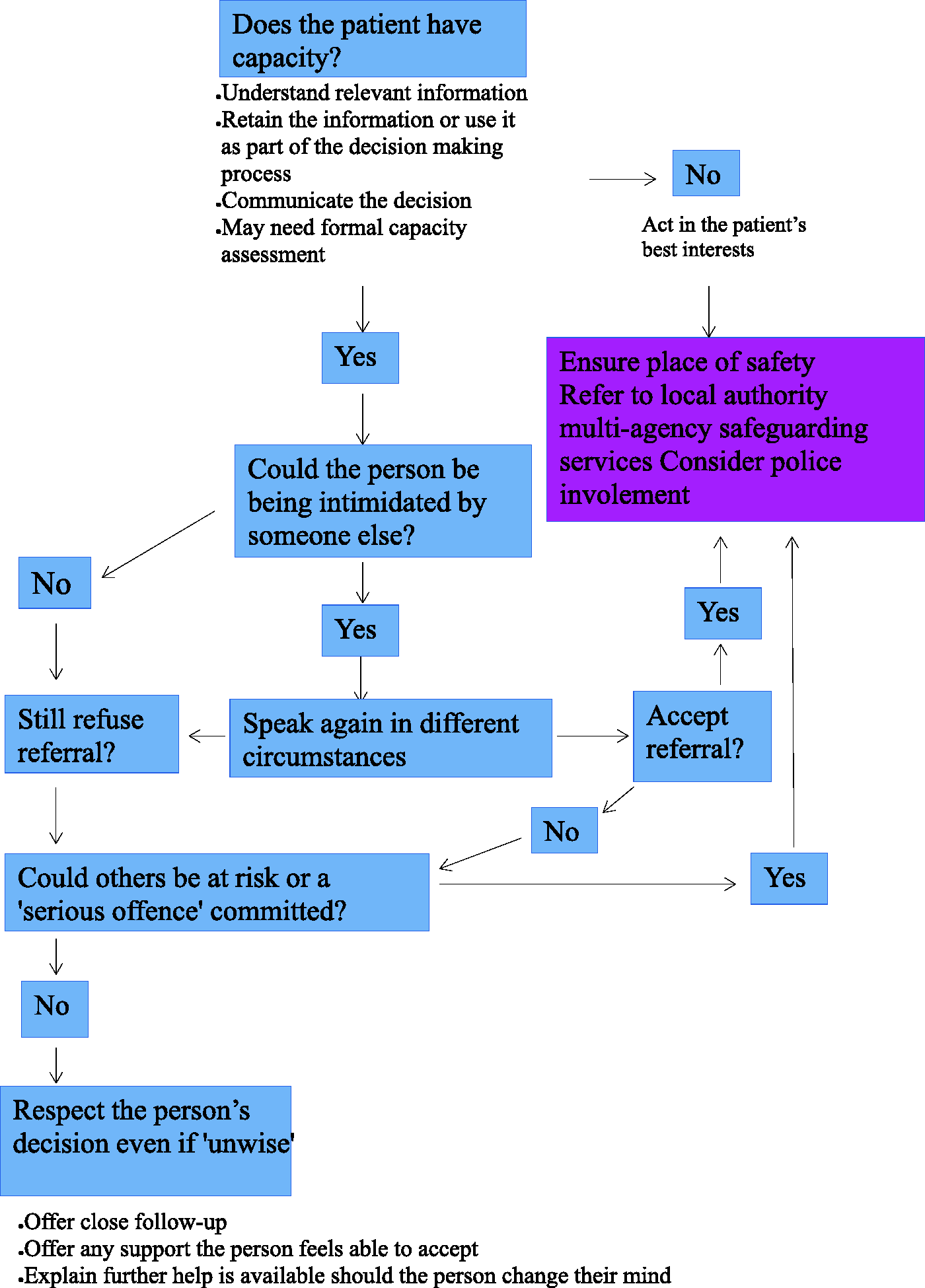
What will happen when I make a referral?
When a referral is made, adult social services will organise an investigation into the alleged abuse and gather information from all those involved, e.g. the GP, care home and family. They will organise a case conference to decide on the best way to proceed and to develop an adult protection plan. The outcomes vary depending on the type and severity of abuse. In less severe cases, increased support, e.g. from external carers or charitable organisations may be sufficient to resolve the problem. In more severe cases, there may be criminal prosecution and, where the abuser is a professional, they may also face disciplinary action, de-registration and referral to the Department of Health Protection of Vulnerable Adults scheme, which can bar them from working with vulnerable adults in the future.
Can elder abuse be prevented?
It is not possible to prevent all cases of elder abuse, but early identification and support of older people and their carers reduces the risk. Some practices have specific systems to highlight vulnerable adults, e.g. the use of flags in electronic patient notes, regular meetings to discuss older people identified as vulnerable, or the allocation of lists of vulnerable people to specific doctors. Preventative interventions should be tailored to the individual, but can include support for the older person to help maintain independence and reduce reliance on others, e.g. with the provision of mobility aids. It can also involve support for carers, for example, through referral to local support organisations, such as Carers Resource.
In organisations (including nursing homes and GP practices) Disclosure and Barring Service pre-employment checks prevent those with criminal records working with vulnerable people and as employers, GPs have the legal responsibility to refer employees who may pose a risk to the Independent Safeguarding Authority. The Care Quality Commission monitor, inspect and regulate adult social care and healthcare to ensure standards of quality and safety are met, but GPs also have a responsibility to report any systematic failures or poor performance that could lead to harm and to promote good safeguarding practice. Well-supervised staff who have received training in elder abuse are less likely to commit abuse and more likely to recognise and report abusive behaviour.
Key points
Older people are a vulnerable group commonly subjected to physical, psychological, financial, sexual abuse, discrimination and neglect It can happen in any situation (homes, care homes, hospitals) and by any perpetrator Those older people with cognitive impairment and high care requirements are most at-risk Elder abuse is easily missed, but routinely questioning those at risk and their carers in a non-judgemental way helps identification Managing a disclosure or suspicions of elder abuse is challenging, and it is crucial that the adult safeguarding multi-disciplinary team becomes involved as early as possible