
Abstract
An abdominal aortic aneurysm (AAA) is defined as a localised dilation of the abdominal aorta. It tends to occur in men between 65 and 79 years of age, and is more common in smokers. Although frequently asymptomatic, an AAA can cause abdominal, groin or back pain. The fatality rate for ruptured AAAs is 90%. In the UK, an ultrasound screening programme for AAAs is now offered to men aged 65 years and over. Management involves surveillance, optimisation of cardiovascular risk status and surgical intervention. However, patients should also be made aware of the Driver and Vehicle Licensing Authority rules as these may prevent them from driving.
The GP curriculum and abdominal aortic aneurysm
Demonstrate an understanding of the importance of risk factors in the diagnosis and management of cardiovascular problems Intervene urgently when patients present with a cardiovascular emergency Demonstrate a reasoned approach to the diagnosis of cardiovascular symptoms using history, examination, incremental investigations and referral Be able to manage cardiovascular conditions, including peripheral vascular disease (arterial and venous)
Definition and epidemiology
An abdominal aortic aneurysm (AAA) is defined as a localised dilation of the abdominal aorta to more than one and a half times its diameter at the level of the renal arteries. In most people, any segment of the abdominal aorta 3 cm or more in diameter is considered to be an AAA (Aggarwal, Qamar, Sharma, & Sharma, 2011).
There is an estimated prevalence in the UK of between 1.3 and 12.7%, depending on age and the AAA definition used (National Institute for Health and Care Excellence (NICE), 2009). Around 5–10% of men aged 65 to 79 years have an AAA (Cosford, Leng, & Thomas, 2007) with the prevalence in women for the same age group being lower at 1.3% (Scott, Bridgewater, & Ashton, 2002). In men aged over 65 years, a ruptured AAA accounts for 1 in 50 of all deaths, with 6000 deaths in England and Wales every year (NHS Choices, 2014).
Pathophysiology and classification
Risk factors for AAA.
Diagnosis
Presenting symptoms
Differential diagnosis of AAA.
Screening for an AAA
In the UK, there is a one-off screening programme for men aged 65 years and over. The aim is to reduce mortality from AAA in men aged 65 to 74 years old. Eligible men are directly invited by the local screening office to one of the clinics. Men aged 65 years and above and who have never undergone screening, can also self-refer.
The screening process is by means of ultrasound imaging to identify an AAA. During the clinic, the nurse practitioner or vascular nurse will also check the patient’s weight and height (to calculate body mass index), smoking history and blood pressure. A drug history is also taken regarding statin and antiplatelet use. Smoking cessation and lifestyle advice is provided.
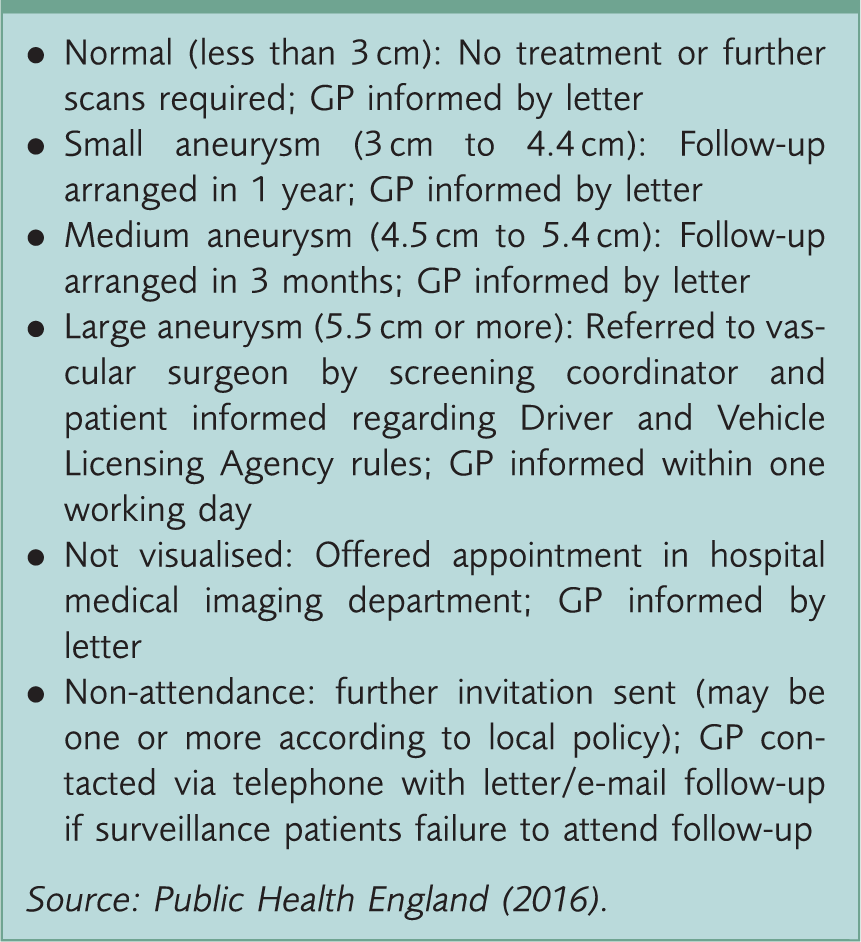
AAA national screening outcomes and follow-up action.
A Cochrane systematic review in 2007 found that screening reduced mortality from AAA, but increased surgical intervention. There was less evidence of benefit for screening women, hence screening is not recommended in women (Cosford et al., 2007).
Investigations
Investigations for AAA.

Adapted from BMJ (2016) and Erbel et al. (2014).
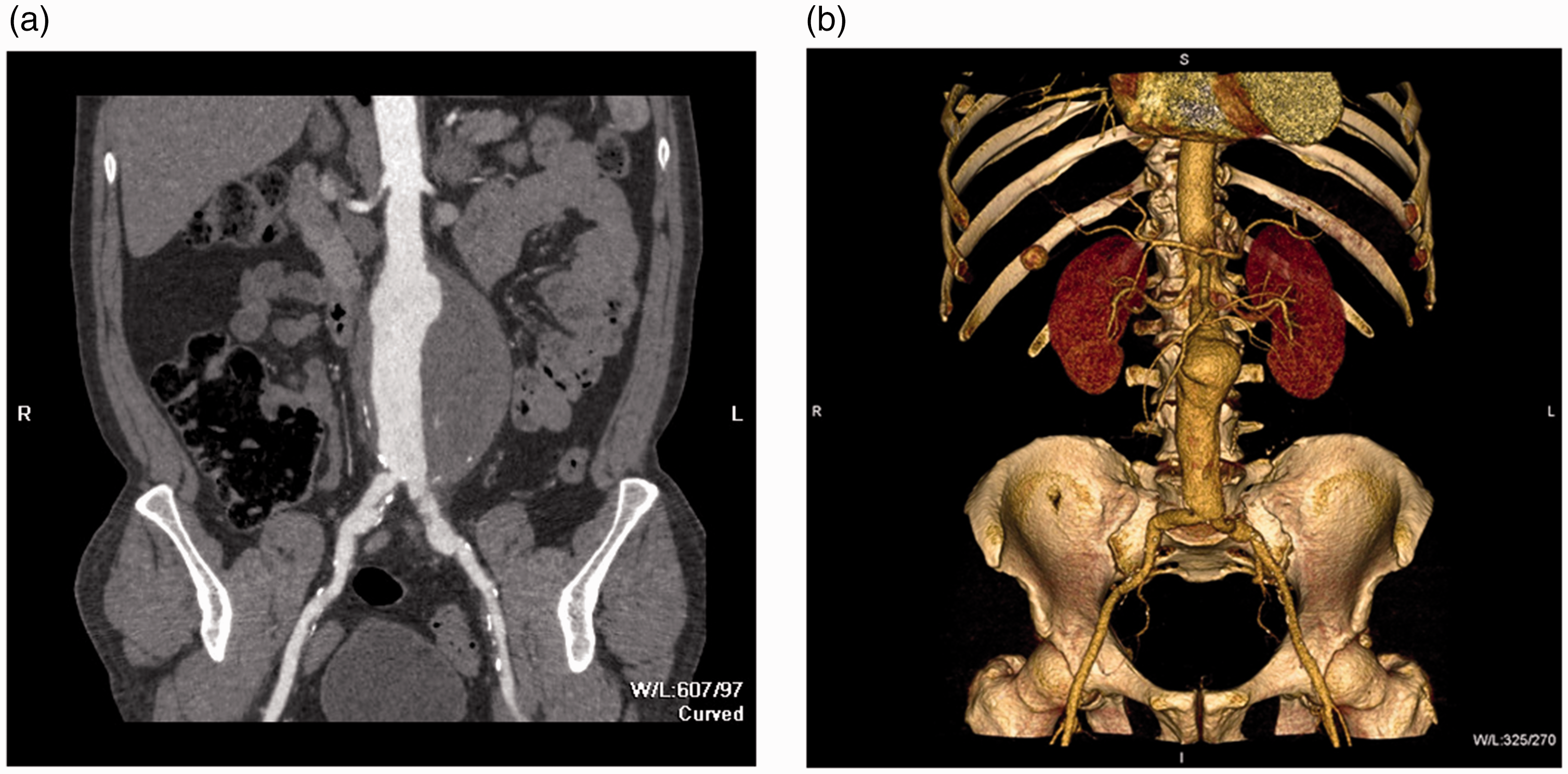
(a) Two-dimensional reconstruction of CT angiogram demonstrating an infra-renal AAA and (b) three-dimensional reconstruction of CT angiogram demonstrating an infra-renal AAA.
Treatment of an AAA
Management of AAA encompasses conservative, medical and surgical treatment. Each of these will be discussed in turn.
Conservative management
Patients with AAA are encouraged to stop smoking and primary care is well placed to offer smoking cessation services. Smoking is associated with aneurysm formation, growth and rupture. Furthermore, stopping smoking 4 to 8 weeks before surgery improves wound healing and cardiovascular mortality (Metcalfe, Holt, & Thompson, 2011; Moll et al., 2011).
Medical management
Although there is limited evidence that medical management of AAA reduces mortality, patients with an AAA are advised on cardiovascular risk reduction. Control of blood pressure and cholesterol with optimal management of cardiovascular disease states and other co-morbidities is recommended.
Antihypertensive medications and beta-blockers
Patients with hypertension should be managed accordingly to reduce their cardiovascular risk. There is mixed evidence about the use of beta-blockers and they may be prescribed for patients with high cardiovascular risk, a month before surgical intervention. Beta-blockers may also be given for angina and other cardiovascular disease in patients with co-existent AAA (Metcalfe et al., 2011; Moll et al., 2011).
Statins
There is some evidence that statins may reduce the risk of AAA rupture, with a lower case fatality when rupture occurs (Wemmelund et al., 2014). Statins also reduce the risk of post-operative myocardial infarction (Metcalfe et al., 2011; Moll et al., 2011).
Antiplatelet medications
There is evidence that the use of aspirin reduces major cardiovascular events, including myocardial infarction and cerebrovascular accidents. Therefore, aspirin is recommended for patients with an AAA to reduce cardiovascular risk (Moll et al., 2011).
Optimisation of other co-morbidities
Cardiac, renal and respiratory impairments will all impact on the outcome of AAA surgical repair. It is recommended that acute or chronic co-morbid diseases are managed optimally, based on best current evidence (Moll et al., 2011).
Surgical management
Elective surgical repair
Surgical management is offered to male patients once the aneurysm has reached 5.5 cm or more in diameter. Patients with small or medium-sized aneurysms are offered surveillance as per the national screening programme discussed in Box 2. In patients with aneurysms 4.5 cm or greater, which have expanded by more than 0.5 cm in a 6 month period, elective repair may also be offered (NICE, 2009). In women with an AAA, there is evidence of rupture occurring at smaller aortic diameters. Accordingly, they are referred for vascular surgery at an aortic diameter of 5.0 cm or more. Any patient with a symptomatic AAA may also be considered for surgical intervention (Moll et al., 2011). There are two types of surgical intervention: endovascular aneurysm repair and open surgical repair.
Endovascular aneurysm repair
Endovascular aneurysm repair (EVAR) is a minimally invasive technique, in which a stent-graft is inserted along the lining of the aorta. This is represented in Fig 2. Access is via the femoral artery in the groin. X-ray-guided catheters and guidewires are used to place the stent-graft in the correct position. The suitability of patients for endovascular repair is determined by age, life expectancy and fitness for surgery. It also depends on aneurysm size and morphology, as well as the relative long-term and short-term benefits of endovascular versus open repair. Discussion about factors affecting suitability between the patient and vascular surgeon will help decision-making.
Diagrammatic representation of endovascular repair of AAA.
The advantages of EVAR include: reduction of pain; trauma; blood loss; general anaesthetic time; and length of stay in intensive care and hospital. EVAR is associated with reduced operative and aneurysm-related mortality. However, endovascular leaks may occur; EVAR is associated with increased rate of complications and re-intervention. There is no difference in the all-cause mortality at medium-term follow-up, between EVAR and open surgical repair. A patient who undergoes EVAR requires annual follow-up surveillance with imaging (NICE, 2009).
Open surgical repair
Open surgical repair (OSR) of an AAA involves an abdominal operation and replacement of the aneurysm with a prosthetic Dacron graft. The repair can be done laparoscopically or with a larger, conventional midline incision (Metcalfe et al., 2011; NICE, 2009). The decision to perform OSR is based on informed patient preference, anatomical unsuitability for EVAR or when patients are unable or unlikely to comply with post-operative surveillance for EVAR (Moll et al., 2011).
Management of a ruptured AAA
Patients with a suspected or confirmed ruptured AAA require urgent resuscitation and surgical evaluation. Surgical repair is the only cure: endovascular repair can be done if the aorto-iliac anatomy allows, otherwise, OSR is done. Overall mortality with a ruptured AAA is 90%, but is 50% in patients who reach the theatre operating table (BMJ, 2016; Erbel et al., 2014).
Complications
Patients with existing cardiac and pulmonary disease, including coronary artery disease and chronic obstructive pulmonary disease, are most likely to experience morbidity following AAA repair. For EVAR, reported complications include vascular injury, inadequate graft fixation, breakdown of graft material, and stent fracture or separation. Endoleaks, graft migration or kinking, thrombosis, rupture and re-intervention are also reported.
The most common morbidities with OSR are myocardial infarction or arrhythmias, and renal failure. Ischaemic colitis and prosthetic graft infection are also reported. Graft infection and aortoenteric fistulas are more common after repair of ruptured AAAs (Aggarwal et al., 2011).
Driver and Vehicle Licensing Agency guidance and AAA
DVLA fitness to drive rules for patients with AAA.

Adapted from DVLA (2016).
Prognosis
The aneurysm size is the strongest risk factor for a ruptured AAA. The estimated risks of rupture based on aneurysm size are (Brewster et al., 2003):
Less than 4.0 cm: 0% 4.0 cm to 4.9 cm: 0.5% to 5% 5.0 cm to 5.9 cm: 3% to 15% 6.0 cm to 6.9 cm: 10 to 20% 7.0 cm to 7.9 cm: 20% to 40% 8.0 cm or greater: 30% to 50%
Furthermore, an aneurysm that expands by 0.5 cm or more over a 6-month period is at high risk of rupture. Smokers and patients with uncontrolled hypertension or wall stress are more likely to have a ruptured AAA (Aggarwal et al., 2011). The mortality rate for a ruptured AAA is approximately 90%, with only half surviving at 30 days in those that undergo emergency surgery (BMJ, 2016).
Key points
AAA is common in men aged 65 years and above and an important cause of morbidity and mortality Smoking is an important modifiable risk factor for developing AAA, and for its progression In the UK, a one-off screening programme is held for men aged 65 years and above, whereby an abdominal ultrasound is performed to measure the aortic diameter Management involves surveillance, cardiovascular risk factor modification and surgical interventions (EVAR and OSR) Patients and GPs should be aware of the DVLA rules for patients with AAA
Footnotes
Acknowledgement
We would like to thank Dr David Roberts for his help with the writing of this article under the InnovAiT ‘buddy’ scheme.