
Abstract
Poverty and poor health are closely linked in a complex relationship. The prevalence of poverty in the UK is growing, resulting in widening health inequalities. Poverty affects the social determinants of health on multiple levels, compromising economic stability, education, social and community contact, lifestyle and healthcare access, and the physical environment. It is associated with an increased prevalence of a range of physical and mental health disorders, with some groups particularly sensitive to the health impacts of poverty, including children, pregnant women, the elderly, refugee and asylum seekers, gypsy and travelling communities, and the homeless. GPs have an important role in identifying the health risks associated with poverty and in supporting individuals and families.
The GP curriculum and poverty and health
Analyse and identify the health characteristics of the populations with which you work, including the cultural, occupational, epidemiological, environmental, economic and social factors and the relevant characteristics of ‘at-risk’ groups Explore the impacts and interactions of these characteristics on the health needs and expectations of your community and its use of the services you provide Acknowledge your professional duty to help tackle health inequalities and resource issues Appreciate the value of health in its broadest sense, as being not only the absence of disease but also a resource that enables a person to adapt successfully to the challenges of living Recognise that factors predisposing to poor health operate across the whole life course from pre-birth to old age Understand that health inequalities are important determinants of health
What is poverty?
Poverty definitions used in the UK.

Relative poverty denotes a basic level of goods and services that an individual living in a society should have access to, compared to others living in the same society: Relative poverty is when someone’s resources are so seriously below those commanded by the average individual or family that they are, in effect, excluded from ordinary living patterns, customs and activities (Townsend, 1979).
In 2014, the threshold for being at-risk of poverty was a disposable income of £9956 for a single-person household without children and £20 907 for a household with two adults and two children under 14 years in age (Office for National Statistics, 2014). However, poverty is more than simply a lack of money and material resources, and reductionist approaches relying on monetary thresholds ignore wider factors that create and perpetuate poverty. The World Development Report 2000 on ‘Attacking Poverty’ uses a more multi-dimensional approach to take into consideration some of these wider factors and identifies four main dimensions of poverty:
Income Health and education or human capital Vulnerability Voicelessness and powerlessness
Figure 1 shows the ‘Web of poverty’; it highlights poverty’s mutually reinforcing dimensions. Poverty is closely linked with social inequality, with direct and indirect effects on physical, mental and social well-being, which will be explored further in this article.
The web of poverty.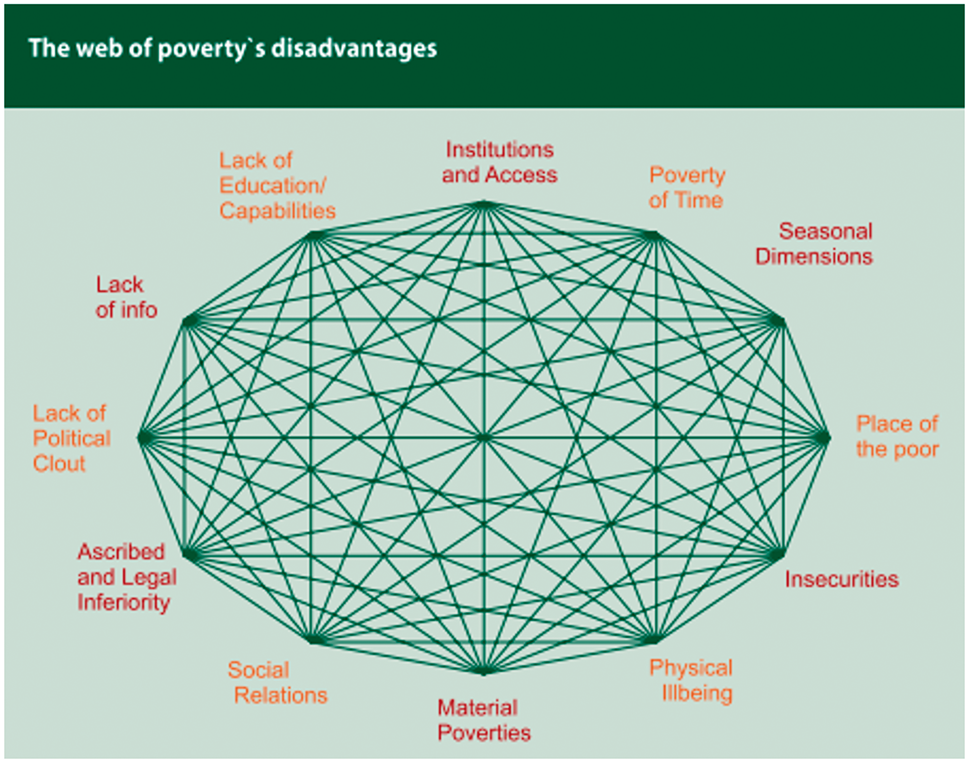
Poverty in the UK
Despite being one of richest countries on the planet, poverty levels in the UK are rising. It is estimated that between 2011 and 2014, almost one-third of the UK population experienced poverty on at least one occasion in their lives (Office for National Statistics, 2014). Poverty is a public health problem, and as GPs we are likely to consult with patients and families experiencing the adverse health effects of poverty.
Groups that are particularly vulnerable to poverty include women, single households, households with dependent children, those leaving education without formal qualifications, the elderly, people with disability, certain ethnic groups, and those living in certain areas such as inner London (Office for National Statistics, 2014). These are the same groups that are recognised as being more vulnerable to ill-health, both physical and mental, as well as facing barriers to accessing healthcare when they need it. One can see how the relationship between poverty and ill-health is both interdependent and complex, trapping vulnerable people in a vicious cycle.
Health impacts of poverty
The UK has an exemplary health system that provides health care that is free at the point of use and guarantees universal health coverage. Despite this, health inequalities are growing. The Marmot Review (Marmot, 2010) showed that only 30% of health outcomes are determined by clinical interventions, with the rest being determined by social factors. Differences in health are ‘extraordinarily sensitive’ to socioeconomic circumstances, and as social inequalities continue to grow, illustrated by the widening gap between the rich and poor, health inequalities are likely to continue to increase (Wilkinson, 1996). Critics point out that under-investment in physical and social infrastructure in deprived neighbourhoods contributes to poorer health outcomes and ‘spill over’ effects in society, such as family disruption and higher rates of crime, homicide and violence (Wilkinson, 1996). The recent Grenfell Tower tragedy in London is an example of the most vulnerable and socially excluded being most affected by social inequalities, with poor housing and safety checks resulting in avoidable deaths, injuries and mental trauma.
Health inequalities
Health inequalities are important, as there are huge differences in health that are closely linked with social disadvantage; these are avoidable and should never exist (Marmot, 2010). Health inequalities arise due to the ‘circumstances in which people grow, live, work, age and the systems out in place to deal with illness’ (Marmot, 2010). Numerous theories and models have been proposed to explain what causes health inequalities (Hay & Peet, 2014). One of these models is Dahlgreen and Whitehead’s ‘rainbow’, as shown in Fig. 2, which groups determinants into three ‘layers’: general socioeconomic, cultural and environmental conditions, social and community networks, and individual lifestyle factors. The common message in all these models is to encourage us to think about how health and health inequalities are affected by macro, meso and micro factors in society that go beyond the health system and the individual.
The social determinants of health.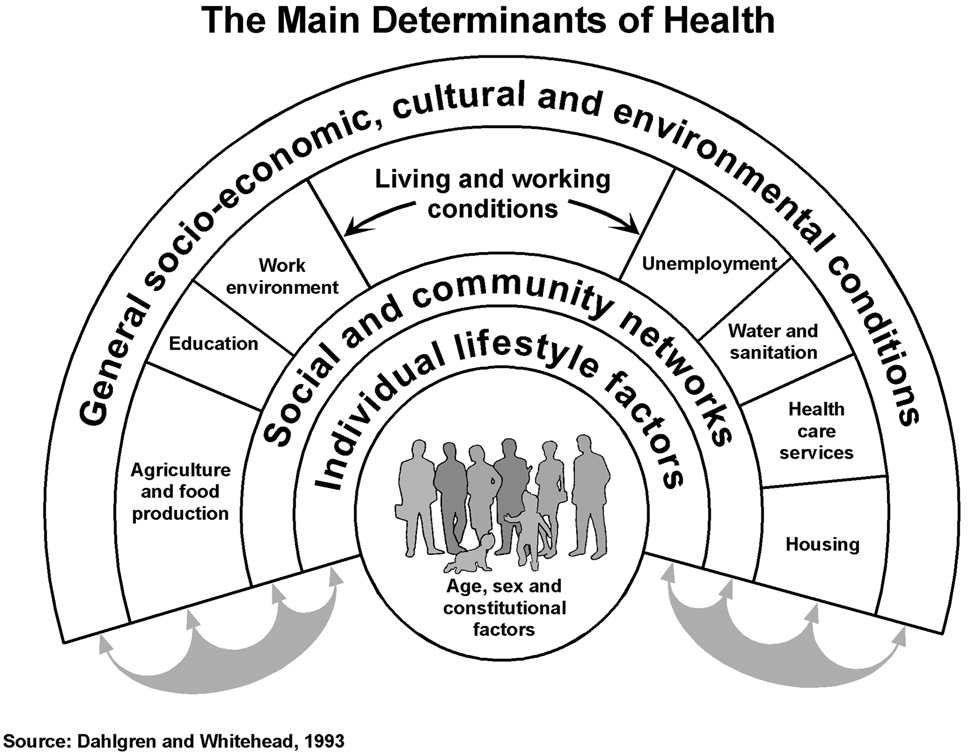
The term ‘Inverse Care Law’, first coined by Julian Tudor Hart in 1971, states that those with the most needs are least likely to use services. Broadly speaking, this can be at three levels: access to healthcare, quality of services and wider external factors, as identified in a King’s Fund report (King’s Fund, 2001). At the general practice level, it is well -recognised that areas with high levels of deprivation are not well supplied with doctors, and patients perceive opening hours as being inconvenient. Patients are also sicker, have lower engagement with health-screening and immunisation programmes, higher rates of cancer mortality, and worse management of chronic disease with increased hospital admission rates for exacerbations of chronic conditions (King’s Fund, 2001; Mercer & Watt, 2007). Also, patients in deprived areas have more problems to discuss within consultations, especially psychosocial issues. They are likely to have shorter consultation times with higher GP stress, lower levels of satisfaction for the patient and variable patient enablement; this in part related to diminished GP empathy and severity of deprivation, all of which perpetuate the Inverse Care Law in general practice (Mercer & Watt, 2007).
Life expectancy and disability
Poverty is associated with a shorter life expectancy and increased burden of ill-health as highlighted in the Marmot Report (Marmot, 2010). Those living in the most deprived areas die almost 10 years earlier than those living in affluent areas, and spend almost 20 more years in poor health, affected by illness and disability earlier, and for longer. As well as an increased risk of chronic disease and mental illness, there is the continued threat of tuberulosis and pandemic flu, as well as infections such as human immunodeficiency virus, hepatitis B and C and sexually transmitted infections (Marmot, 2010). A higher prevalence of disability, long-term work incapacity and lower perceived general health has also been reported among socially deprived individuals (Mackenbach, 1992).
Chronic illness and multi-morbidity
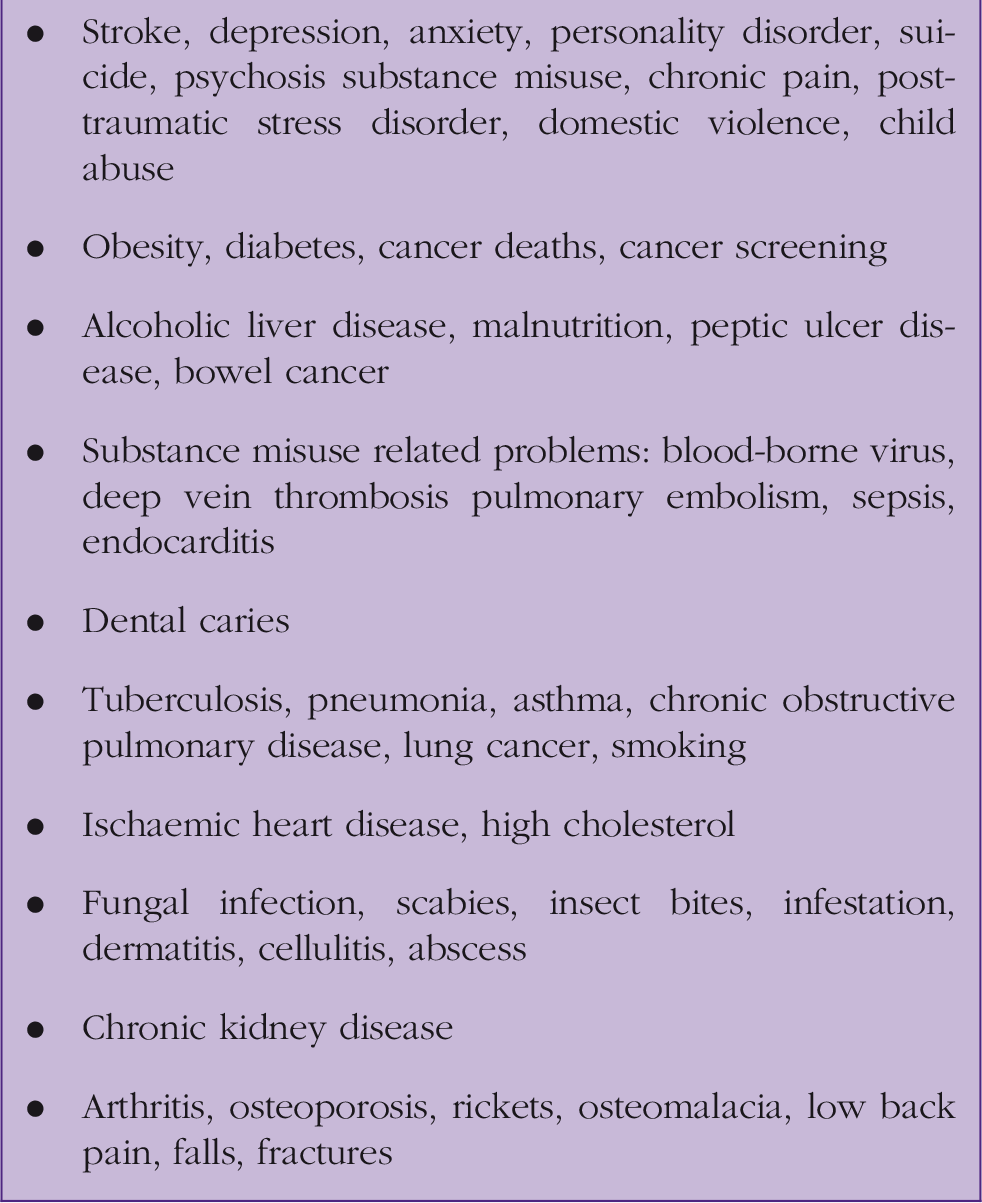
Health impacts of poverty.
The higher co-morbidity of physical and mental health is attributed to increased vulnerability to adverse lifestyle behaviours (such as poor nutrition, obesity, tobacco, substance misuse), unfavourable material living conditions and physical working conditions, along with psychosocial stress, lack of social support and less adequate supply and use of healthcare (Mackenbach, 1992). Food poverty is growing in the UK, affecting groups who are already more vulnerable, such as the disabled, elderly and ethnic minorities (Faculty of Public Health, 2005). The impact of poor nutrition on obesity, cardiometabolic disorders and cancer is well-documented and contributes to the higher chronic disease burden (Shahid & Shahid, 2016).
Mental health
Socioeconomic factors that influence mental health.
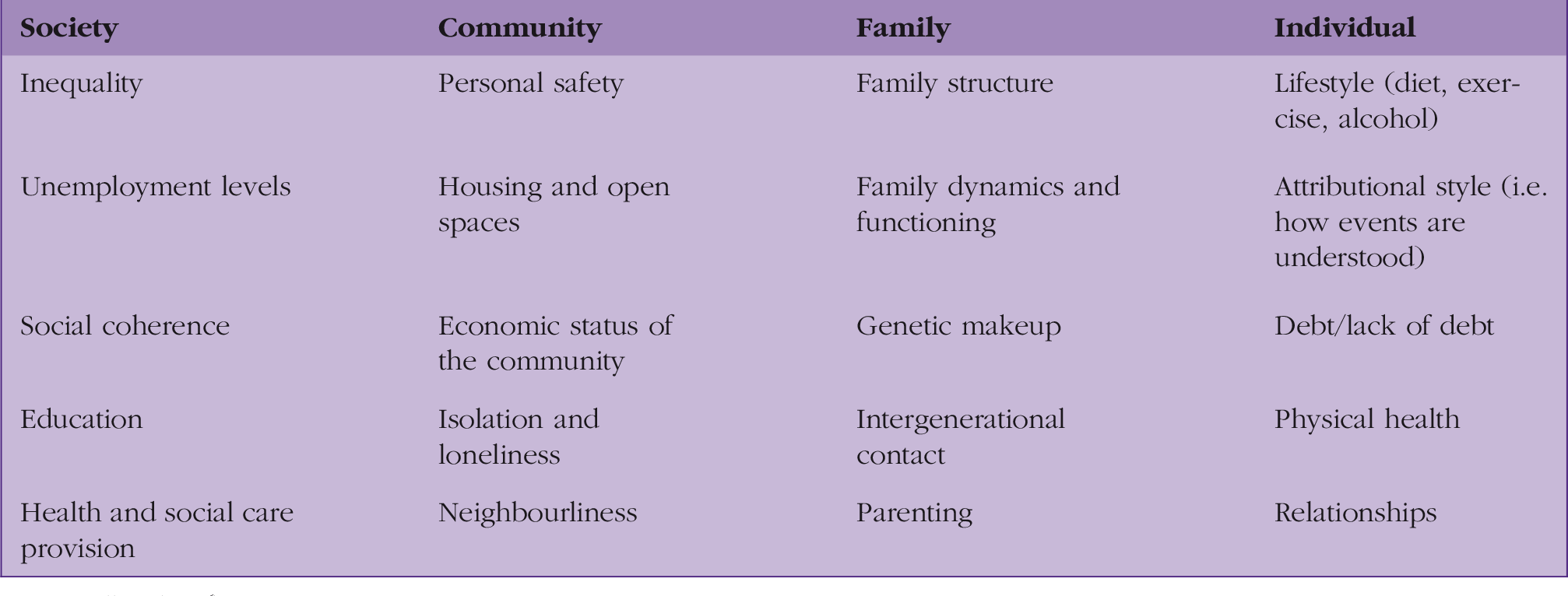
Source: Elliot (2016).
Major depressive and psychotic disorders, suicide, phobic disorders, alcohol and substance misuse are shown to be associated with social deprivation and psychiatric admissions (Murali & Obeyede, 2004; Myers, McCollam, & Woodhouse, 2005). There is also emerging evidence that personality disorders are more prevalent in socially deprived inner city areas (Murali & Obeyede, 2004; Myers et al., 2005).
Children from disadvantaged backgrounds demonstrate poorer cognitive function, with higher rates of common and severe mental illness, and twice the prevalence of emotional and behavioural disorders (Elliot, 2016). Of concern, only one-quarter of patients with long-term mental illness are in employment, one-third are in debt and one in four have problems with housing, creating a vicious cycle of social deprivation and mental illness (Myers et al., 2005).
Specific vulnerable groups
In addition to the general effects of poverty on morbidity and mortality, there are specific vulnerable groups that experience more potent effects of poverty on their health.
Children
Children growing up in poverty have a higher risk of death across almost all conditions in adulthood, which may be due to exposures at sensitive or critical periods of development and/or cumulative harmful exposures. Households with poverty experience a higher prevalence of sudden infant deaths and childhood accidents, obesity, asthma, tooth decay, failure to thrive and chronic disease, as well as a higher prevalence of childhood abuse and neglect (Wickam, Anwar, Barr, Law, & Taylor-Robinson, 2016). This is attributed to exposure to harmful risk factors that contribute to ill health, such as bad housing, overcrowding, fewer safe areas, poor sleeping pattern, poor nutrition, passive smoking and parental mental health problems (NHS Wirral, 2012).
Pregnant women
Pregnant women living in poverty have worse outcomes including higher rates of miscarriage, prematurity, intrauterine growth restriction, placental abruption and maternal mortality. These may be due to factors such as lower maternal education and health literacy, poor help-seeking behaviour, poor nutrition, smoking, stress and mental health problems (NHS Wirral, 2012). Socioeconomic inequality is strongly associated with poor perinatal mental health, including antenatal depression, anxiety and serious mental illness such as major depressive and psychotic disorders, phobic disorders, suicide, and postnatal mental health disorders (Ban et al., 2012).
Elderly
The strongest and most consistent determinant of poor health in the elderly is poverty. Poor elderly patients were more likely to report overall poor health, chronic illness, psychiatric morbidity and multi-morbidity (Grundy & Holt, 2001). Cuts to social care have been implicated in hospital admissions for ‘social reasons’ and delayed discharge (due to inadequate package of care and safety concerns). Poorly performing pension funds, changes to taxation and the universal benefit system will influence how elderly people access care, and the disposable income available for food and fuel. Poverty is also a risk factor for malnutrition, a growing problem in the elderly and associated with more frequent and longer hospital admissions, dependency on carers and family, as well as premature mortality (Hickson, 2006). Socially disadvantaged elderly people are also at risk of fuel poverty and excess winter deaths.
Refugees and asylum seekers
The Faculty of Public Health (2008) provides an excellent overview of the health needs of asylum seekers. In this group, it is even more important to consider the patient’s story and circumstances to contextualise and empathise with their problems. Asylum seekers may be victims of torture, rape and imprisonment in their home country. They may arrive from areas with weak health systems or from refugee camps with poor nutrition and sanitation. Their migration journey exposes them to severe physical and mental stress. They are at risk of trafficking and modern-day slavery, and on arrival in the UK, may feel a loss of status, social support, cultural shock and social exclusion; all of which increase health needs. Difficulty in accessing health care services, limited awareness of entitlements, problems with GP registration, and language barriers can cause health to deteriorate.
Specific health problems known to be higher among refugees and asylum seekers include: communicable diseases, due to very poor immunisation coverage; low uptake of family planning services; chronic disease; dental disorders; consequences of injury and torture; post-traumatic stress disorder; depression; and anxiety. Women’s health issues in this group are grim. Asylum-seeking pregnant women are seven times more likely to develop intrapartum complications, and have a three-fold higher mortality rate. There are also concerns around low uptake of cervical and breast cancer screening and female genital mutilation.
Gypsy and travelling communities
When compared with other socially excluded groups and ethnic minorities, gypsy and travelling communities experience high poverty levels and significant health inequalities. They are more likely to report long-term illness, disability, respiratory problems, cardiovascular problems, miscarriage, infant and childhood mortality, arthritis, problems with mobility, self care, activities of daily living and work, chronic pain, anxiety, depression, substance misuse and suicide. These health inequalities are exacerbated by racism, discrimination and exclusion from social and civic life, the labour market and other ‘multiple and complex forms of exclusion’ (Cemlyn, Greenfields, Burnett, Matthews, & Whitwell, 2009). These communities are also less likely to be registered with a GP, present with acute crises and have over-dependence on A&E. These communities also have low uptake of immunisation and cancer screening, resulting in disease outbreaks, such as measles. GPs often have little awareness of gypsy and traveller culture and social background, and how this impacts access to primary care services. Specific issues include gender roles, mental health stigma, fear of being referred to social services, the significant role of the family, very low literacy rates, and problems with homelessness (Atterbury, 2010).
Homeless communities
Homeless people experience a multitude of complex physical, psychological and social needs. About 4 in 10 homeless people are estimated to have a long-term physical health problem and half a mental health problem. Over one-third of homeless people have a substance misuse problem, two thirds consume harmful levels of alcohol, and almost 8 in 10 smoke; over one-third do not consume at least two meals a day (Homeless Link, 2014). Common and severe mental illnesses in this population are higher, including depression, anxiety, drug-induced psychosis, schizophrenia, personality disorder and dual diagnoses (Wright, Tompkins, Oldham, & Kay, 2004). The misuse of drugs and alcohol can cause associated physical health problems, including hepatobiliary disorders, blood-borne infections venous thromboembolism and abscesses.
Conclusion
We can see how poverty adversely impacts health, in particular among vulnerable groups, but the converse also holds true, which can trap individuals and households in a vicious cycle of poverty and poor health. With austerity measures and cuts to public and welfare services, this scenario is becoming more common, and is worsening health disparities. Working at the intersection of public health, policy and personalised clinical practice presents opportunities for GPs to identify potential problems and risks early and to offer support and intervention through a holistic multi-disciplinary approach. These will be explored in a separate article.
KEY POINTS
Poverty in the UK is increasing, which is worsening health inequalities There are different definitions of poverty People living in poverty are exposed to adverse social, economic and environmental factors that negatively impact health Poverty is associated with reduced life expectancy, disability, chronic physical and mental illnesses and multi-morbidity Specific groups vulnerable to the effects of poverty include children, pregnant women, the elderly, the homeless, refugees and asylum seekers