
Abstract
Lower intestinal bleeding covers a spectrum of intestinal bleeding originating distal to the ligament of Treitz. In 11% of cases, the source of bleeding will be found in the upper gastrointestinal tract. Lower intestinal bleeding can occur either in the form of fresh blood, also known as haematochezia, or in the form of black, tarry and foul-smelling stools, also known as melaena. It can be chronic and mild or severe and life-threatening. This article will focus on the common causes of lower intestinal bleeding, clinical presentation, assessment and management, as well as providing guidance for referral to secondary care.
The GP curriculum and lower gastrointestinal bleeding
Know how to interpret common symptoms in general practice, including lower intestinal and rectal bleeding Be aware that due to social and cultural factors some patients might find it embarrassing to discuss digestive problems Understand the National Institute for Health and Care Excellence referral guidelines for suspected cancer and the indications for urgent referral for suspected gastrointestinal cancer Be able to provide an appropriate environment for abdominal and rectal examination with dignity and under chaperoned conditions
Epidemiology
The annual incidence of acute massive lower intestinal bleeding has been estimated to be 20–30 cases per 100 000 of the population. The incidence increases with age, and is significantly higher in men than women (Strate, 2005).
Lower intestinal bleeding is associated with significant morbidity and mortality, especially in the elderly. This may be related to a variety of factors including comorbid conditions and the influence of polypharmacy (Zuckerman & Prakash, 1998).
Causes of lower gastrointestinal bleeding
Causes of lower intestinal bleeding.
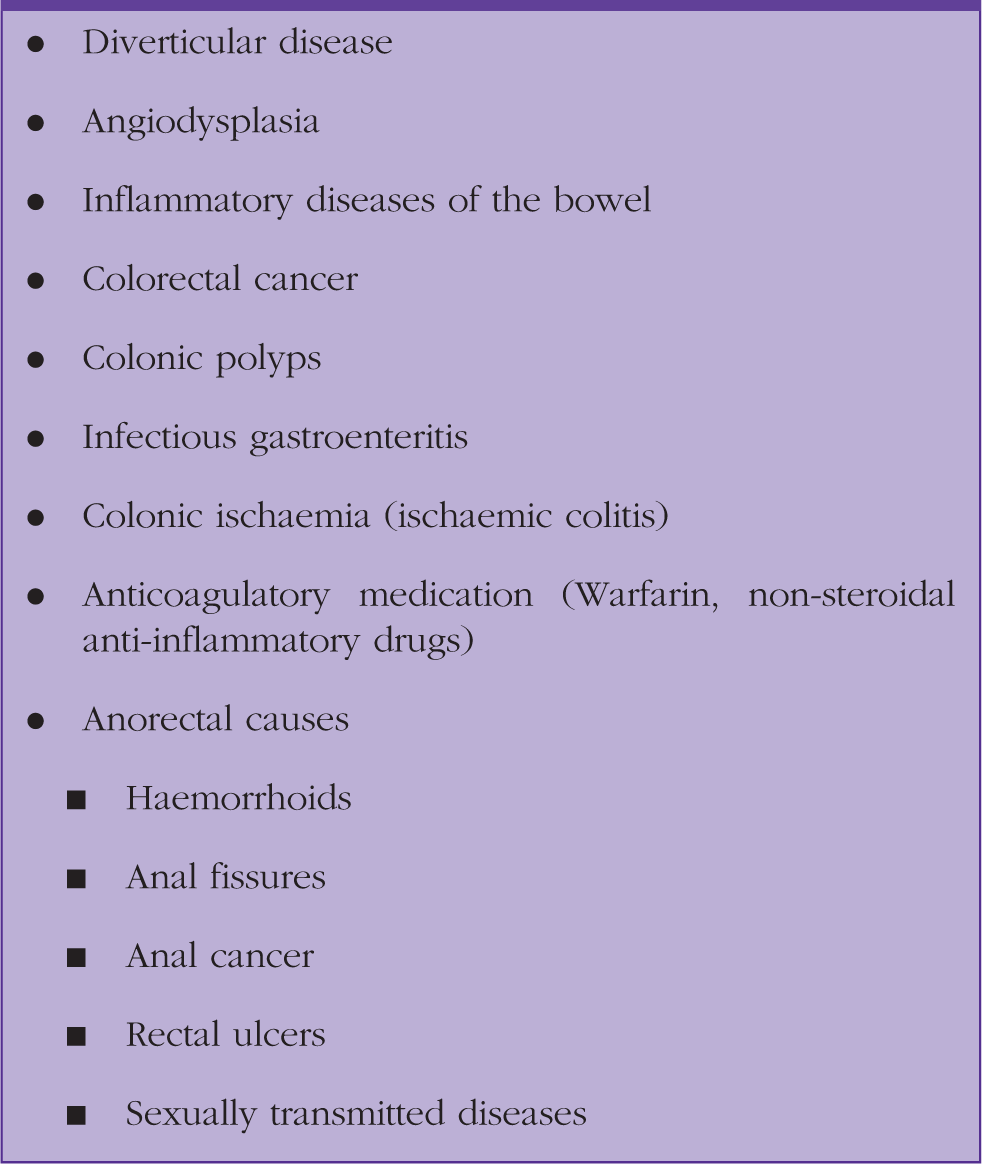
Diverticular bleeding
Although diverticular bleeding is a rare event, diverticular disease is common and the leading cause of lower intestinal bleeding, accounting for 20–55% of all cases. It is rare in patients under the age of 40 years, but it affects more than 65% of patients aged over 85 years (Strate, 2005).
Factors promoting the risk of bleeding are constipation and hard stools. The use of blood thinners, such as non-steroidal anti-inflammatory drugs (NSAIDs) or warfarin, also increases the risk of diverticular bleeding (Chait, 2010).
Although 90% of diverticula are located in the left colon, 50–90% of diverticular bleeding occurs from right-sided colonic diverticula. Diverticular bleeding is painless and usually ceases spontaneously (Stollman & Raskin, 2004).
However, the risk of re-bleeding after an episode of bleeding is 25%. This can increase up to 50% in those patients, who have had more than two episodes of diverticular bleeding (Finne, 1992).
Angiodysplasia
Angiodysplasia is a vascular abnormality of the gastrointestinal tract that predominantly occurs in the elderly. Its aetiology is not fully understood, but it is thought to occur as a result of degenerative lesions of the submucosal venules associated with increases in intraluminal pressures. Colonic lesions most commonly occur in the right colon (Strate, 2005).
This disorder, as a source of lower intestinal bleeding, accounts for up to 40% of cases. Bleeding is painless and can be subacute, chronic or recurrent (Chait, 2010).
Inflammatory diseases of the bowel
Inflammatory diseases of the bowel include:
Inflammatory bowel disease (Crohn’s disease, ulcerative colitis) Ischaemic colitis Radiation proctitis Infectious enteritis
Inflammatory bowel disease comprises Crohn’s disease and ulcerative colitis. Although Crohn’s disease can affect any part of the gastrointestinal tract, it most commonly affects the terminal ileum. Clinically, patients will complain of diarrhoea mixed with blood (Chait, 2010).
Ulcerative colitis starts in the rectum in the form of proctitis and progresses proximally. All patients suffering from ulcerative colitis will present to their GP complaining of bloody diarrhoea and rectal bleeding (Ghosh, Shand, & Ferguson, 2000).
Ischaemic colitis accounts for 3–9% of all cases of lower intestinal bleeding; it results from impaired blood supply to the colon along the watershed areas, which are regions, characterised by impaired blood flow. These include the splenic-flexure and the recto-sigmoid junction. Factors such as hypotension or embolic events can promote ischaemic colitis and patients can clinically present with cramping abdominal pain followed by haematochezia or bloody diarrhoea (Chait, 2010).
Examples of infectious enteritis and colitis include pseudomembranous colitis, typhoid colitis, Escherichia coli O157:H7 infections and cytomegalovirus colitis. However, these types of colitis rarely cause significant lower intestinal bleeding (Zuckerman & Prakash, 1999).
Radiation proctitis is an inflammation of the distal rectum, which occurs in patients treated for genitourinary or gynaecological malignancies. Symptoms can include bloody diarrhoea and cramps that can develop within weeks to years after initiation of radiotherapy of the pelvic region (Mitra et al., 2015).
Neoplasm
Malignancies of the colon and rectum account for 10–20% of cases of lower intestinal bleeding, and can be the initial presenting symptom in 26% of colorectal malignancies. Bleeding is painless and can be occult or mild (Chait, 2010).
Anorectal causes
Haemorrhoids are the most common anorectal cause of rectal bleeding. Haemorrhoidal bleeding can present with either fresh painless bleeding covering the stool or large bleeding into the toilet bowel during defecation (Kaidar-Person, Person, & Wexner, 2007).
Further pathologies include anal fissures, which are tears in the mucosa of the anal canal, localised in the midline anteriorly or posteriorly in 90% of cases. Fissures affect mainly young adults and are associated with constipation or repetitive trauma. The hallmark of fissures is a sharp pain on defecation associated with fresh bleeding on the toilet paper or mixed with the stool (Babakhanlou, 2016). There are various other pathologies that can present with rectal bleeding. These are less common and include anal cancer, sexually transmitted diseases or dermatological conditions (Box 1).
Clinical presentation of lower intestinal bleeding
Lower intestinal bleeding can be acute, occult or obscure. Occult bleeding refers to the presence of a positive faecal occult blood test, but without any evidence of visible blood loss. Obscure bleeding is defined as bleeding from the gastrointestinal tract without any identified source despite diagnostic evaluation (Chait, 2010).
In most patients lower intestinal bleeding will stop spontaneously. However, 10–40% of patients will experience recurrent bleeding episodes; between 5 and 50% of patients with persistent bleeding require surgical intervention (Strate, 2005).
Chronic blood loss can occur from anywhere in the gastrointestinal tract without any obvious signs of bleeding and result in iron-deficiency anaemia.
Hence, common presenting symptoms may be fatigue, weakness, shortness of breath, light-headedness, pallor or symptoms of angina in patients with pre-existing ischaemic heart disease (Mehta, 2009).
Diagnosis
It is crucial for the assessing physician not to miss serious causes of lower gastrointestinal bleeding. One of the challenges in the evaluation and assessment of intestinal bleeding is the lack of uniformity in clinical presentation and variability of acuity on presentation.
Hence, the assessment of a patient presenting with intestinal bleeding should include taking a thorough history and a physical examination as the initial evaluation (Strate & Gralnek, 2016).
An appropriate environment with chaperoned conditions should be provided.
History
History should explore duration, frequency and colour of blood. The presence of red-flag signs and symptoms should be sought, including weight loss, abdominal pain, and change in bowel habit or pain and bleeding on defecation.
A detailed medication history should be obtained. Drugs such as aspirin, warfarin and NSAIDs can increase the risk of bleeding. A history of travel abroad may be significant, and any hospital admissions or courses of antibiotics within 90 days prior to presentation should be documented.
The past medical history should evaluate the presence of:
Diverticular disease Inflammatory bowel disease Peptic ulcers Previous pelvic radiation Recent removal of polyps Previous gastrointestinal malignancy Presence of cardiovascular problems (ischaemic heart disease, atrial fibrillation)
Examination
Assessment includes inspection of the patient, general examination and a digital rectal examination. During inspection the examiner should pay attention to signs of weight loss, cachexia or muscle wasting. A general examination should include measurement of the vital signs (blood pressure, pulse). Signs of shock and haemodynamic stability should be obvious, but clinically significant bleeding can lead to less obvious postural changes in blood pressure or heart rate.
A more detailed physical examination should assess organomegaly in the abdomen, the presence of ascites or abdominal masses.
An inspection of the anal and perianal area should identify excoriation marks, fissures, visible haemorrhoids or papillomata.
Unless refused by the patient, all patients presenting with rectal bleeding should have a digital rectal examination, in order to check for the presence of a mass, look for visible blood and pus on the finger. The examiner should provide an environment where rectal examination can be performed with dignity and under chaperoned conditions.
Investigation
A laboratory work up depends on the age of the patient, the past medical history, and the findings on clinical examination. Initial laboratory investigations in primary care should include full blood count, a full metabolic profile and clotting studies, if coagulopathy is suspected. Haemoglobin may be normal or minimally decreased even with severe bleeding.
If there is suspicion of inflammatory bowel disease (IBD) or inflammatory conditions, C-reactive protein and erythrocyte sedimentation rate should be checked. Faecal calprotectin can be measured to detect colonic inflammation and to differentiate from irritable bowel syndrome (IBS). Levels of < 40 µg/g exclude IBD in patients with IBS symptoms (Menees, Powell, Kurlander, Geol, & Chey, 2015).
If the patient reports a history of recent travel abroad, use of antibiotics or infectious colitis, then a stool sample should be sent for stool culture and a stool assay testing for Clostridium difficile toxin A and B.
Management
The management of intestinal bleeding depends on the severity of symptoms and the cause of bleeding. Patients presenting with heavy rectal bleeding and signs of shock need an immediate referral to hospital for resuscitation, further investigation and management.
In the majority of cases bleeding stops spontaneously.
Risk factors for poor outcome in patients with lower intestinal bleeding.

Diverticular disease comprises 20–55% of all cases of lower gastrointestinal bleeding and it is estimated that 3–15% of patients with diverticulosis will experience bleeding (Adams & Margolin, 2009).
The aetiology of diverticular bleeding is poorly understood, and since it has been attributed to repetitive trauma, the primary management of asymptomatic diverticulosis remains high-fibre diet, increased fluid intake and the use of bulk laxatives to avoid constipation (Aldoori & Ryan-Harshman, 2002).
Treatment of patients with infectious colitis depends on the type of infection. This includes specific antimicrobial therapy upon identification of the organism (Chait, 2010).
In most patients, lower intestinal bleeding will stop spontaneously, but around 25% will need intervention. In patients with severe bleeding and those not responding to conservative treatment within 48 hours, hospital admission is indicated (Strate, 2005).
Due to the increased risk of re-bleeding, and especially for those patients taking anticoagulation, the American College of Gastroenterology has made the following recommendations (Strate & Gralnek, 2016):
NSAIDs should be avoided in patients with acute lower intestinal bleeding, particularly due to diverticular disease and angiodysplasia In patients with cardiovascular disease and history of lower intestinal bleeding, aspirin used for secondary prevention should Aspirin for primary prevention of cardiovascular events in patients with lower intestinal bleeding should be avoided
Referral guidelines
Patients with lower intestinal and rectal bleeding who are haemodynamically unstable should be referred to hospital immediately. In patients where cancer is suspected, a negative faecal occult blood test or a negative rectal examination should not rule out a referral to secondary care.
Clinical features with an urgent suspicion of cancer referral include (Scottish Cancer Referral Guidelines, 2016):
Repeated rectal bleeding without an obvious anal cause Blood mixed with the stool Persistent change of bowel habit (especially looser stools) for more than 4 weeks Right-sided abdominal mass Palpable rectal mass Unexplained iron-deficiency anaemia Past history of lower gastrointestinal cancers with the above symptoms
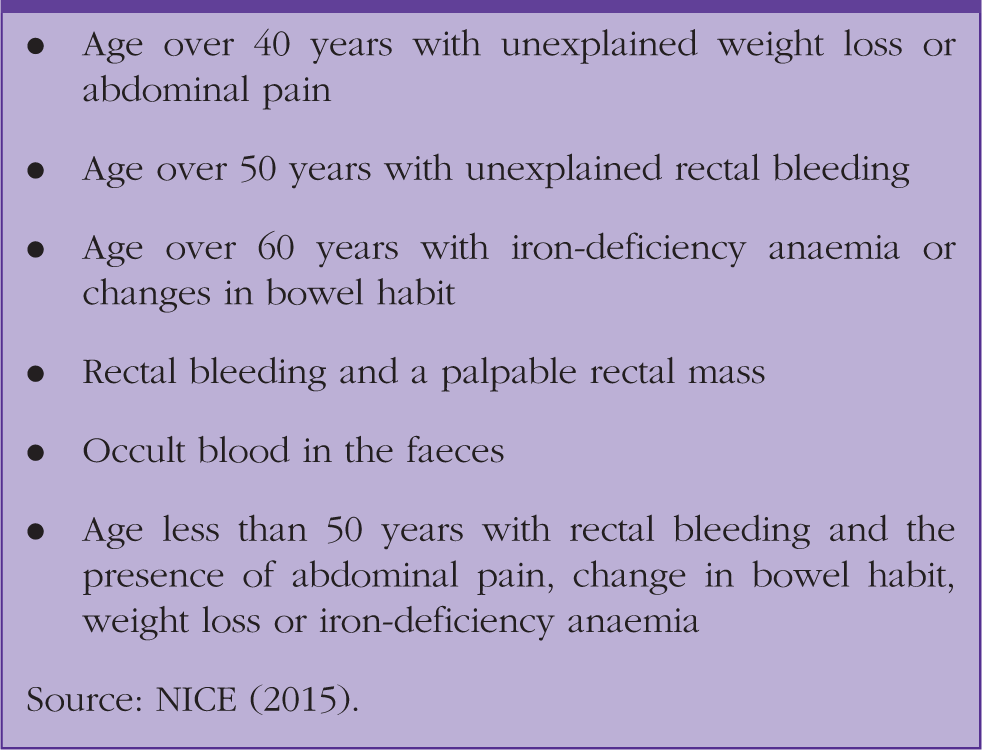
Criteria for suspected lower gastrointestinal cancer (appointment within 2-weeks).
Conclusion
Lower intestinal and rectal bleeding are common presentations in general practice. The incidence of lower intestinal bleeding increases with age. Morbidity and mortality correspond to the presence of comorbidities and polypharmacy that are frequently found in the elderly. Hence, in elderly patients, and in those with poor social support, these factors should be considered when it comes to decision making about hospital admission.
KEY POINTS
Lower intestinal bleeding accounts for 20% of all cases of gastrointestinal bleeding and is a common presentation in general practice In the majority of cases lower intestinal bleeding is self-limiting, but re-bleeding can occur in up to 40% of cases A thorough history and physical examination, including a digital rectal examination should be carried out in all cases Patients with red-flag symptoms should be referred urgently to secondary care for further assessment and investigation