
Abstract
Thyroid neoplasms represent the most-common endocrine tumour and constitute an extremely varied spectrum of disease. At the most severe end, they may have a very poor prognosis. Malignant thyroid tumours constitute around 1% of cancers and cancer-specific deaths in the UK, with just under 3000 new diagnoses each year and around 350 deaths annually in the UK alone. Although the incidence has doubled over the last 20 years, the mortality rate among men has not changed, although survival rates have improved in women. Thyroid cancer originates from follicular or parafollicular thyroid cells that can give rise to cancer that is well-differentiated to poorly differentiated. Most tumours retain endocrine differentiation, however, and may cause problematic symptoms from aberrant hormone levels.
The GP curriculum and thyroid cancer
Understand how to recognise rarer but potentially serious conditions such as oral, head and neck cancer Know the epidemiology of head and neck cancers, including the risk factors, and identify unhealthy behaviour Biochemical tests can be diagnostic and often necessary for monitoring metabolic and endocrine diseases, so it is important for GPs to know which tests are useful in a primary care setting and how to interpret these tests and understand their limitations Thyroid diseases including goitre, hypothyroidism, hyperthyroidism, benign and malignant tumours, thyroid eye disease, thyroiditis, neonatal hyper- and hypo-thyroidism
Presentation
Features associated with increased probability of malignancy.

Causes
Thyroid cancers are considered to be due to a combination of environmental and genetic factors, but exposure to ionising radiation, such as increasing use of X-ray and computed tomography (CT) scans, is considered to contribute to a rise in incidence. Following the Chernobyl nuclear disaster, thyroid cancer incidence rose significantly in those affected by the nuclear fallout, especially the paediatric population, and those exposed to radioactive iodine isotopes (Nikiforov, 2010). Genetic contributions include multiple endocrine neoplasia-2 (MEN-2), which is inherited in an autosomal dominant pattern and is associated with a significant risk of medullary thyroid carcinoma by the age of 70 years, alongside risk of phaeochromocytoma and parathyroid tumours (Moline & Eng, 2011).
Referral
The National Institute for Health and Care Excellence (NICE) guidelines suggest that when a patient presents with a thyroid lump and symptoms of tracheal compression, such as stridor at rest, immediate admission to hospital is necessary (NICE, 2016).
An urgent 2-week wait referral to a thyroid surgeon or endocrinologist is indicated if the lump is unexplained, if there are unexplained voice changes associated with a thyroid mass, when there is cervical lymphadenopathy with associated thyroid mass, and with a painless but rapidly growing thyroid mass (British Thyroid Association, 2014; NICE, 2016). Thyroid surgery may be undertaken by ear, nose and throat, endocrine or general surgeons depending on local availability. Children with a thyroid nodule should also be referred urgently (2-week wait) to a general paediatrician or paediatric endocrinologist (NICE, 2016).
Patients with an unchanging nodule or goitre, with no other concerning features (such as lymphadenopathy, breathing or voice changes or family history of thyroid cancer) can be managed in primary care, as well as those with non-palpable, asymptomatic nodules less than 1cm ,AQ3/>found incidentally on a scan without other concerning features (British Thyroid Association, 2014; NICE, 2016). Figure 1 shows an algorithm for a patient presenting with a thyroid lump in general practice.
Algorithm of pathway for a patient with a thyroid lump presenting to a GP.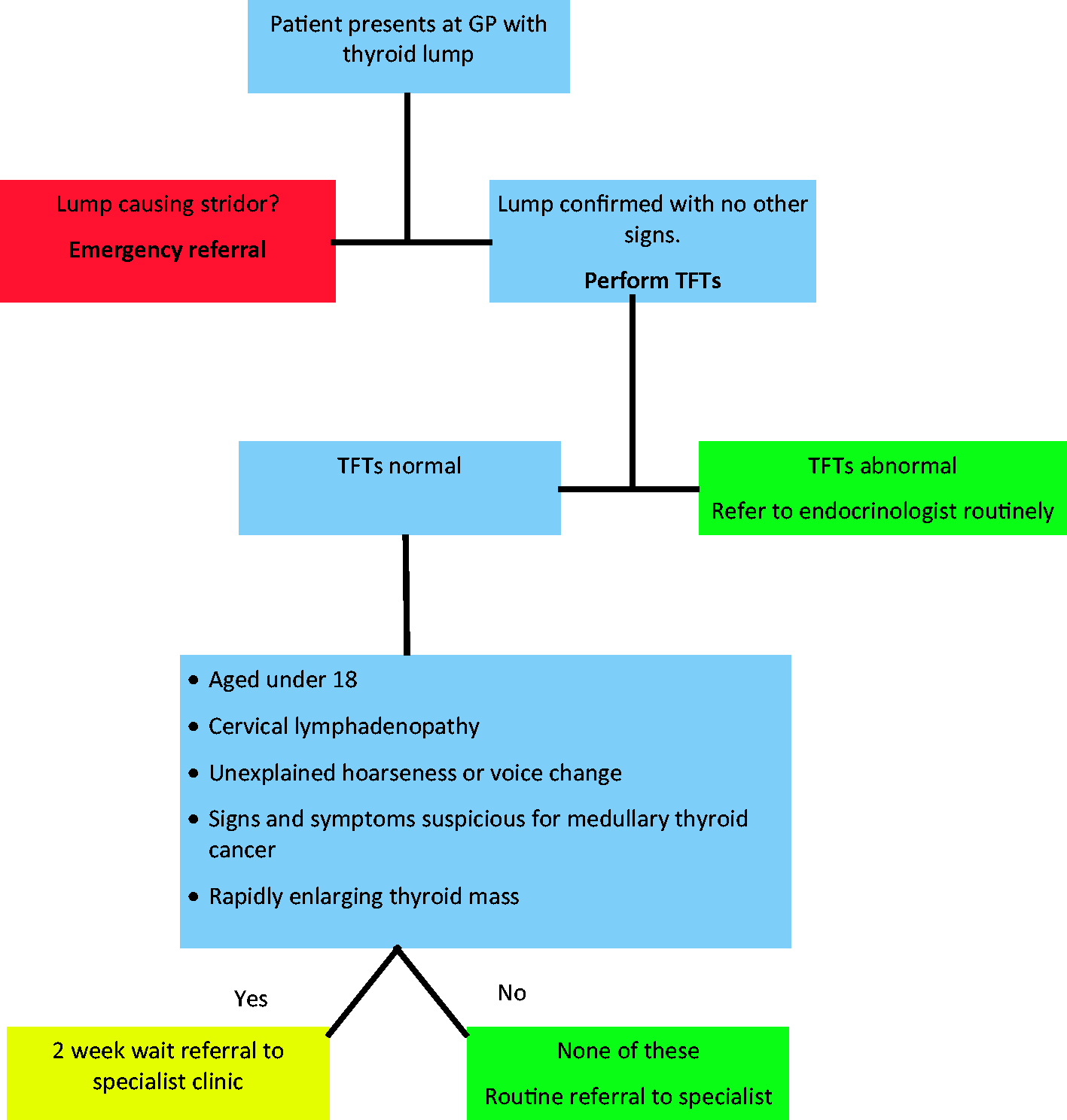
Diagnosis
Following a thorough history and examination, ultrasound is an extremely sensitive investigation with high specificity and increases the quality of diagnostic fine needle aspiration cytology (FNAC) samples (Hambly et al., 2011). Thyroid function tests should be performed, and thyroid autoantibodies if there is suspicion of autoimmune thyroid disease, (British Thyroid Association, 2014) ,AQ2/>as well as calcitonin and carcinoembryonic antigen if medullary thyroid cancer is suspected (Elsei et al., 2004).
Magnetic resonance imaging or CT scanning should be considered if the limits of the goitre cannot be determined, but iodinated contrast media should be avoided, as this can delay iodine-based treatments of malignant thyroid cancer. Cytology by FNAC is the preferred way to obtain a tissue diagnosis. Core biopsy with ultrasound guidance can be used if FNAC does not yield a diagnosis and tissue diagnosis would alter management (particularly where lymphoma is suspected) (British Thyroid Association, 2014).
Use of a ‘one stop shop’ can enable patients with a suspicious neck lump to receive an ultrasound scan, FNAC and review of sample adequacy by a cytopathologist. This reduces the need for patients to return to the clinic, as non-diagnostic cell samples and a repeat can be taken on the same day if necessary. This approach to diagnosis improves patient care and reduces anxiety and delays in diagnosis. The patient and their GP should be informed of any subsequent diagnosis promptly, with appropriate supporting information. Ultrasound images are graded via the ‘U’ classification system, with U1 (normal), U2 (benign), U3 (indeterminate), U4 (suspicious), U5 (malignant) and should be used to determine which thyroid nodules should be subjected to FNAC (British Thyroid Association, 2014).
Thy cytology criteria.

Classification
The classification of thyroid cancers depends on their histological characteristics, with papillary thyroid cancer constituting approximately 80% of all thyroid cancers (Katoh, Yamashita, Enomoto, and Watanabe, 2015). Most papillary thyroid cancers have a good prognosis, although approximately 10% may have lymph node and lung metastasis. Approximately 10% of thyroid cancers are of the follicular carcinoma type, with a worse prognosis than papillary thyroid cancer.
Differentiating follicular adenoma from carcinoma may be difficult histologically; the distinction is based purely on the finding of tumour capsule invasion or vascular invasion, which may be inconspicuous. The appearance of the tumour cells can be very similar in both cases. However, the distinction is important, as follicular adenoma has a very good prognosis whereas the prognosis of follicular carcinoma is poor.
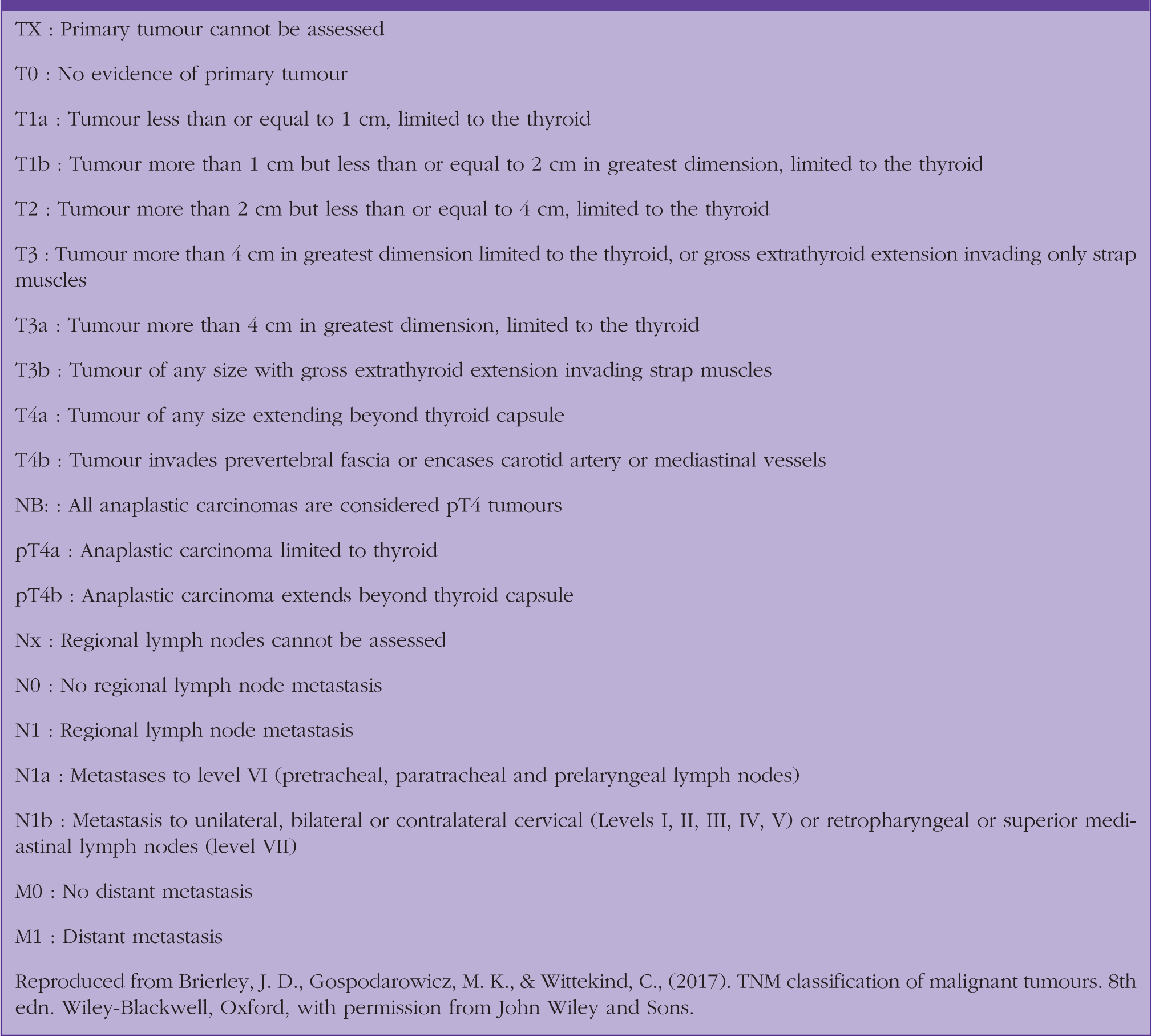
TNM classification of thyroid cancer.
Treatment
Following diagnosis, the initial treatment is a thyroidectomy with or without neck dissection, with total thyroidectomy indicated for large tumours or those considered to have additional risk factors, as this is associated with better survival and reduced recurrence of the tumour (Pelizzo et al., 2007). In tumours (T2 or less) that are 4 cm or smaller (greatest dimension) without additional risk factors, hemithyroidectomy can be considered. Following thyroidectomy, radioactive Iodine (131I) can be used in patients with papillary or follicular thyroid cancer, where the aim is to treat residual, recurrent or metastatic disease (British Thyroid Association, 2014). Although there is possible prolonged survival and reduced risk of local and distant tumour recurrence (Sawka et al., 2004), there are important complications of which to be aware. After radioactive iodine, female patients need to avoid pregnancy for at least 6 months. Male patients should not father a child for 4 months after treatment, and all patients should remain a safe distance from others for a short period of time. Other complications include dry mouth, an unpleasant taste in the mouth, pulmonary fibrosis and increased risk of secondary malignancy. Although there are no licensed medications for thyroid cancer, this is expected to change (British Thyroid Association, 2014). In patients where a palliative approach is required, it is important to have robust advanced care plans in place, particularly as neck compression may lead to airway obstruction by the tumour. Consideration should be given to the need for a surgical airway and whether this is in the best interests of the patient.
Follow-up and prognosis
Thyroid cancer and treatment can cause aberrations in hormone levels, such as TSH and calcitonin. However, patients who have undergone a hemithyroidectomy alone do not require TSH suppression or long- term follow-up (British Thyroid Association, 2014). Those who have undergone a thyroidectomy or are more complicated will require follow up 6 monthly, then yearly after the first year if responding well to treatment. Patients with more significant disease or incomplete response to treatment require more frequent monitoring. Those who received radioactive 131I require lifelong follow up. The treatment of thyroid cancer can cause patients to become hypothyroid and their TSH levels rise. These patients will require lifelong levothyroxine, and the effects of abnormal thyroid hormones require monitoring, due to risks such as atrial fibrillation and osteoporosis (British Thyroid Association, 2014). Calcium levels should also be monitored, particularly where parathyroid glands have been affected by treatment.
As previously discussed, some specific subtypes are associated with a greater rate of mortality. Quality of life for patients post-thyroid cancer has been shown to be impaired (Singer et al., 2012), and may be related to instability in thyroid hormone levels and calcium homeostasis, as well as the psychological, social and financial pressures patients experience following a cancer diagnosis. Avoiding abnormal thyroid levels, treating hypoparathyroidism should it arise, monitoring calcium levels and reducing the risk of osteoporosis are important considerations in the follow-up of patients in general practice (British Thyroid Association, 2014).
Depending on the subtype of thyroid malignancy, TSH may act to promote tumour proliferation, and so an important therapeutic aim is to suppress this effect. The dose of levothyroxine is therefore often higher than in normal replacement, as the therapeutic aim is to suppress TSH to <0.1 mU/L. Although this should be managed by the thyroid cancer multidisciplinary team, the GP must be made aware of target TSH levels. Patients with hypocalcaemia and on calcium supplements should be monitored with the aim of keeping calcium within normal limits (British Thyroid Association, 2014).
Summary
Thyroid cancer constitutes around 1% of all cancer deaths, with variable prognosis depending on the cancer type. The incidence is rising, and is responsible for around 350 deaths in the UK each year. Although treatment options are available, the mainstay is surgery plus radiotherapy. The consequences of treatment can have significant and life-changing effects for the patient. Patients will require lifelong monitoring of thyroid function and calcium homeostasis.
KEY POINTS
Thyroid cancer accounts for around 1% of all cancer deaths in the UK Suspicious thyroid lumps with normal TFTs should prompt urgent referral to a specialist Prognosis is very variable with papillary and medullary carcinomas usually having a good prognosis Follicular carcinomas have an intermediate prognosis and anaplastic carcinomas a very poor prognosis Patients may experience long-term side effects as a result of treatment Patients will require lifelong monitoring of thyroid function and calcium levels
ORCID iD
Dr Jonathan Mills http://orcid.org/0000-0002-5998-8434