
Abstract
Osteoarthritis of the knee is a degenerative condition that is commonly seen in the elderly population and sometimes occurs earlier in the athletic population. Pain and stiffness are common features, which can be debilitating. Clinical assessment of the knee joint requires consideration of its associated muscles, ligaments, tendons, bursae and menisci. The aim of this article is to provide an overview of knee pain assessment, to discuss the diagnosis of knee osteoarthritis, and to review some evidence-based management options.
The GP curriculum and osteoarthritis of the knee
Communicate health information effectively to promote better outcomes Use simple techniques and consistent advice to promote activity in the presence of pain and stiffness Agree treatment goals and facilitate supported self-management, particularly around pain, function and physical activity Assess the importance and meaning of the following presenting features:
Pain: nature, location, severity, history of trauma Variation of symptoms over time Loss of function: Weakness, restricted movement, deformity and disability, ability to perform usual work or occupation Understand that reducing pain and disability rather than achieving a complete cure could be the goal of treatment Understand the challenge that many musculoskeletal conditions might be better and more confidently managed by other healthcare personnel rather than GPs because most GPs do not gain the necessary treatment skills during their training Be aware of the burden of treatment for patients with long-term musculoskeletal conditions like osteoarthritis
Epidemiology
Knee osteoarthritis is a degenerative condition that is characterised by progressive articular cartilage loss and remodelling of subchondral bone. It affects 27% of women and 21% of men, with an increase in incidence for both groups from the age of 45 years (Pereira et al., 2011). Painful knee osteoarthritis associated with mild-to-moderate disability affects up to 10% of adults over the age of 55 years, accounting for 0.5% of primary care consultations in this age group, rising to 1% for those aged over 70 years (Peat, McCarney, & Croft, 2001). Early onset knee osteoarthritis can also present in the young athletic population, due to repetitive impact loading on the articular cartilage and sports-related knee injuries (Amoako & Pujalte, 2014).
Basic knee anatomy
The knee joint is a synovial hinge joint (Fig. 1) that enables mainly flexion and extension movements with limited rotational movements. It can be divided into the medial tibiofemoral compartment, lateral tibiofemoral compartment and the patellofemoral compartment. The articular surfaces of the femur, tibia and patella are covered by hyaline cartilage. Osteoarthritis can affect one or more compartments, however, it typically starts in the medial compartment, as 70–75% of load distributes to that side during the stance phase of gait (Scott, Nutton, & Biant, 2013).
A sagittal section through the knee joint.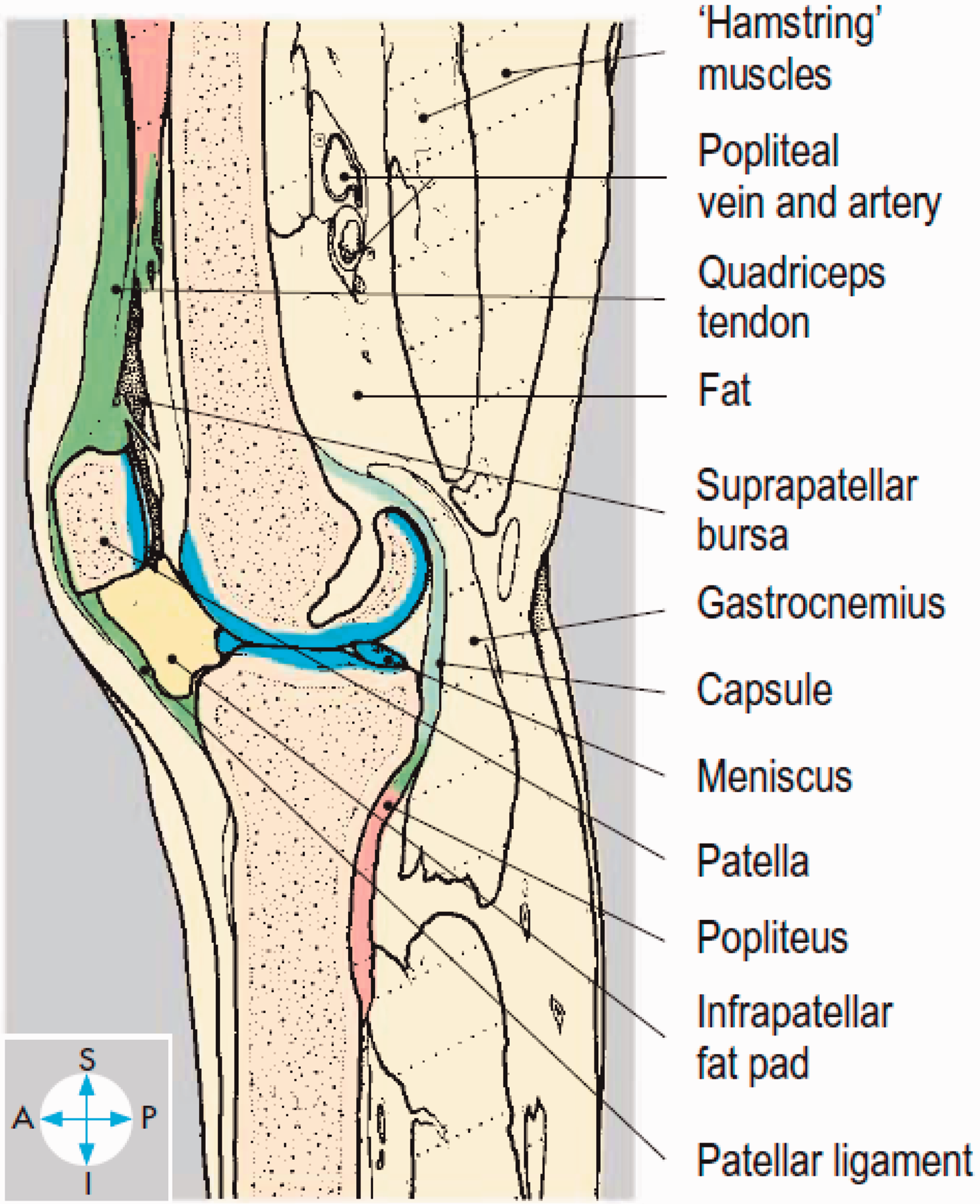
The two ligaments within the joint capsule are the anterior cruciate ligament (ACL) that prevents anterior displacement of the tibia relative to the femur, and the posterior cruciate ligament (PCL) that does the opposite. The medial collateral ligament (MCL) prevents valgus forces on the knee with its origin at the medial femoral epicondyle and insertion at the medial tibial condyle. The lateral collateral ligament (LCL) prevents varus forces on the knee and originates from the lateral femoral epicondyle to insert on the fibular head.
There are two C-shaped menisci (medial and lateral) that attach to the intercondylar eminence of the tibia and the borders of the joint capsule. They function to distribute load, absorb shock and provide stability.
There are many other structures to consider around the knee, such as bursae (prepatellar, suprapatellar, infrapatellar, pes anserinus), tendons (quadriceps and patellar) and muscles (quadriceps, hamstrings, and popliteus).
History
Knee osteoarthritis typically presents with a chronic progressive history of knee pain exacerbated by movement that worsens towards the end of the day. Knee pain can be localised (e.g. anterior knee) or generalised. Stiffness is another prominent feature and crepitus can be associated. Joint swelling develops secondary to synovitis (soft) and or osteophyte formation (hard).
Other knee osteoarthritis symptoms may include instability and locking. Instability (‘giving way’) can develop when the quadricep and hamstring muscles weaken due to underuse. True locking is a physical obstruction inside the knee that becomes stuck during movement (usually extension) and often requires the patient to move or shake the knee around for a few minutes to free it up again. The causes of true locking associated with knee osteoarthritis include degenerative meniscal tears and loose fragments of bone or calcium deposits. Pseudo-locking, in contrast, refers to irritation of the knee joint (e.g. from swelling or inflammation) causing a brief pain-induced muscle spasm, which presents as a sudden ‘catching’ sensation that quickly resolves. It is very important to differentiate pseudo-locking from true locking, as true locking requires knee arthroscopy to remove the obstruction.
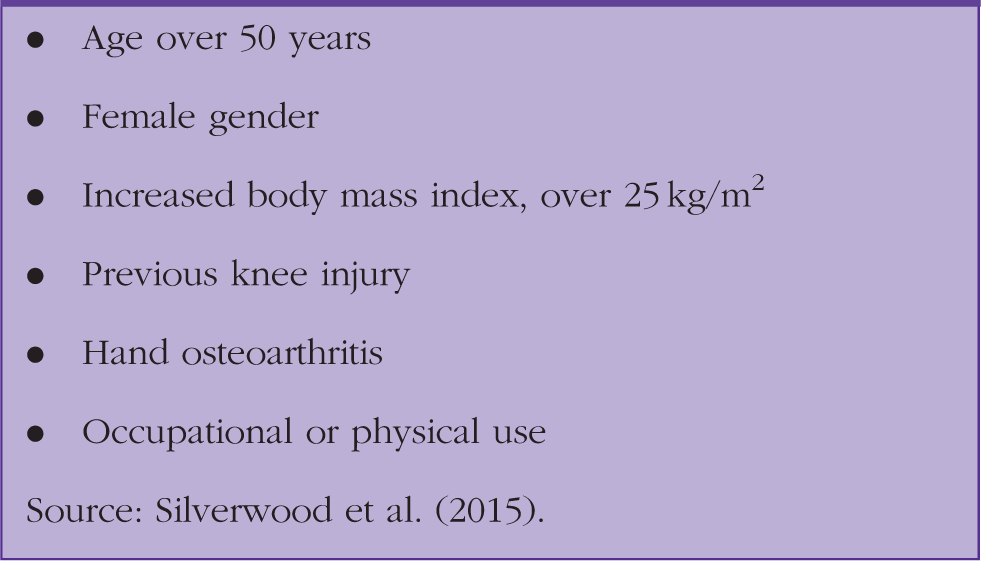
Risk factors for knee osteoarthritis.
Furthermore, referred pain from the back, hip or ankle should be considered, and sinister features such as night sweats, fevers, weight loss and history of cancer needs to be covered.
Knee structures associated with osteoarthritis
Ligaments
There is evidence that ligament instability increases the risk of developing osteoarthritis, because it can alter mechanical-loading patterns, and therefore, damage the extracellular matrix of articular cartilage (Blalock, Miller, Tilley, & Wang, 2015). ACL tears are common injuries in the young athletic population and a review has found that 50% of those with ACL tears develop osteoarthritis 10–20 years later (Lohmander, Englund, Dahl, & Roos, 2007).
Menisci
Knee osteoarthritis shares many similar risk factors and biological processes to degenerative meniscal tears (Howell, Kumar, Patel, & Tom, 2014). An arthroscopic study has shown a 40% coincidence rate of meniscal injuries in those with knee osteoarthritis (Wang, Cai, Liu, Wang, & Gao, 2005). Furthermore, those who have previously had partial or complete meniscectomy operations (e.g. secondary to an acute injury) are at risk of developing osteoarthritis in later life (Papalia, Del Buono, Osti, Denaro, & Maffulli, 2011).
Examination
The knee should be examined using a ‘Look, Feel, Move and Special Tests’ approach. Depending on the extent of the knee symptoms, clinical examination maybe limited.
Look
Inspect the knee from the front, side and back with the patient standing, walking and then supine. Look for any swelling, asymmetry, muscle-wasting, deformity or scarring. Medial compartment knee osteoarthritis may create a knee varus deformity and lateral compartment knee osteoarthritis may create a knee valgus deformity. Quadriceps muscle-wasting and joint-swelling maybe present.
Feel
First, palpate the skin for warmth then palpate the quadriceps tendon and the borders of the patellofemoral joint for any tenderness. With the knee extended, palpate the medial and lateral tibiofemoral joint lines followed by the MCL, LCL, and patellar tendon. Check for an effusion by sweeping fluid at the medial aspect of the knee towards the suprapatellar pouch then applying pressure laterally to look for a bulge in the medial compartment as fluid re-accumulates.
The posterior knee structures, such as the hamstring tendons and gastrocnemius origins, can be palpated in the prone position. A Baker’s cyst is commonly associated with knee osteoarthritis, as it directly communicates with the joint.
Move
Flexion and extension of the knee should be performed actively and passively. Normal range of movement is typically 0o in extension and 130o in full flexion, but there are individual variations. Knee crepitus and locking maybe detected.
Special tests
The MCL and LCL can be tested by applying valgus and varus forces, respectively, to a knee flexed at 30o. The ACL can be tested with Lachman’s test or the anterior drawer test. The PCL can be tested with reverse Lachman’s or posterior drawer test.
There are a number of tests for meniscal pathology. The most common test is McMurray’s test, where the knee is flexed and the examiner internally and externally rotates the tibia while extending the knee and feeling for a palpable ‘clunk’. Another test is Thessaly’s test, performed with the patient standing on the affected leg with the knee flexed at 20o, hands supported by the examiner, and then asked to rotate the knee internally and externally three times to reproduce symptoms. Simple joint line palpation tenderness can also be suggestive of a meniscal injury.
Differential diagnosis
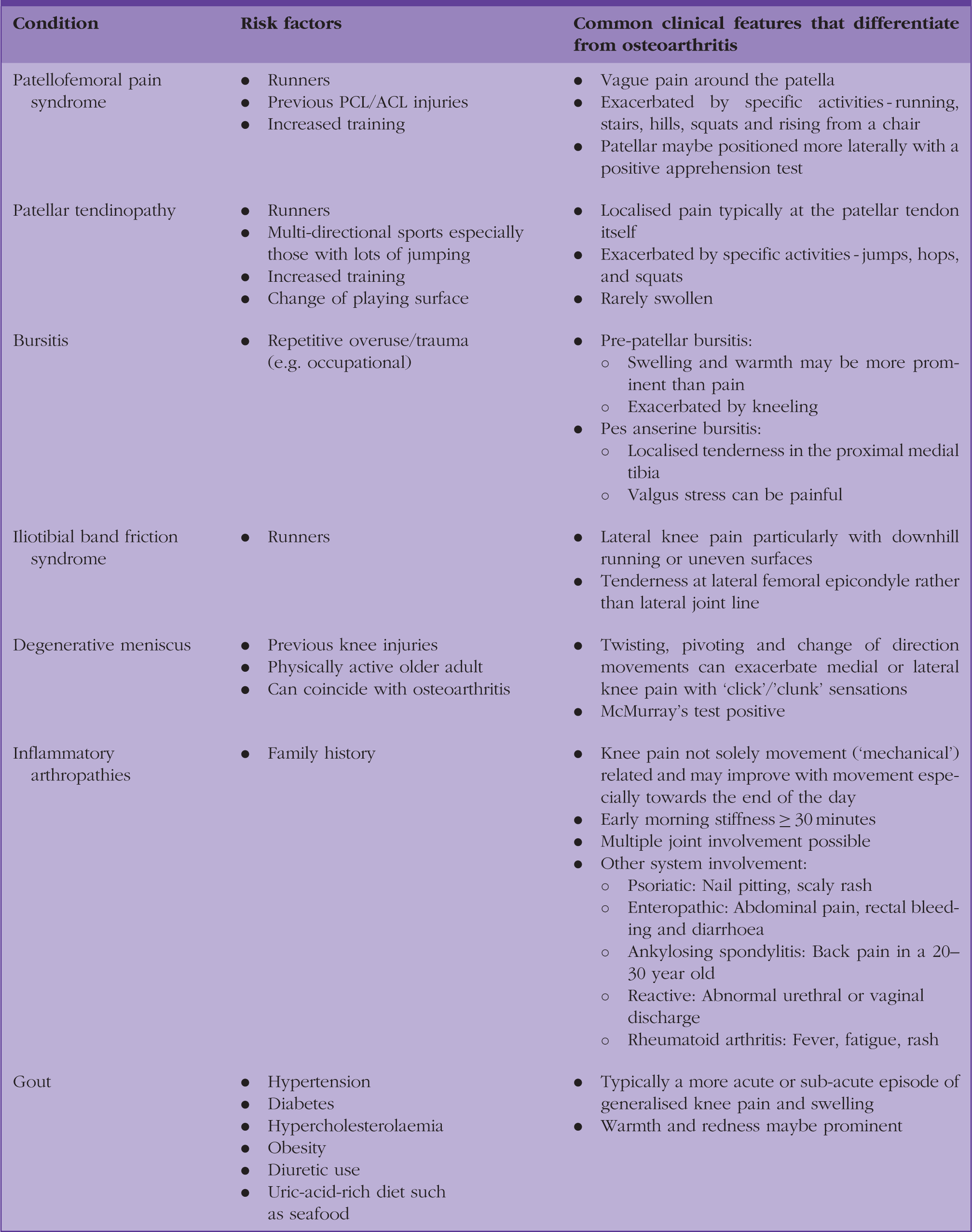
Differential diagnosis of chronic non-traumatic knee pain.
Investigations for knee osteoarthritis
The National Institute for Health and Care Excellence (NICE) guidelines (NICE, 2014) recommend that a diagnosis of osteoarthritis can be made clinically without investigations if a patient fulfils all of the following:
Is aged 45 years or over Has activity-related joint pain Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30 minutes
Plain X-rays
The radiographic features of osteoarthritis include osteophytes, joint-space narrowing, and subchondral bone sclerosis. The severity of osteoarthritis classified radiologically does not correlate with symptoms and disability (Bedson & Croft, 2008). An X-ray should therefore only be considered as an adjunct to confirm osteoarthritis if, for example, clinical examination is limited by pain, or if there is suspicion of other bony pathology (e.g. tumours).
Magnetic resonance imaging
Magnetic resonance imaging (MRI) should not be routinely requested for knee osteoarthritis, because it is too sensitive and costly. A cohort study of 710 people with no radiographic evidence of knee osteoarthritis found that MRI detected abnormalities in 86–88% of painless knees (Guermazi et al., 2012).
MRI of a knee should only really be considered if there are plans to refer the patient onwards to an orthopaedic knee surgeon. Conditions where a knee MRI should be considered include suspected loose body within the joint, ligamentous injury (e.g. ACL) and traumatic meniscal tears in younger patients.
Blood tests
These are not required for osteoarthritis. If there is suspicion of gout, then a urate level can be requested, but it is not diagnostic. For inflammatory arthropathies, erythrocyte sedimentation rate, C-reactive protein, and rheumatoid factor may be appropriate.
Joint aspiration
Any fluid that is aspirated from the knee joint should always be sent off for analysis. In knee osteoarthritis with large effusions, joint aspiration can provide symptomatic relief and improve range of movement. Gout will show the presence of monosodium urate crystals in aspirated joint fluid and pseudo-gout will show calcium pyrophosphate.
Management for knee osteoarthritis
Exercise
There are many health benefits of physical activity in general, as it can help with weight loss, improve mood, joint pain, function and quality of life. A Cochrane review evaluating 32 studies of land-based exercises for knee osteoarthritis found a modest improvement in pain scores with a relative reduction in pain of 27% and an absolute reduction in pain of 12%. It found a similar improvement in physical function with a relative improvement of 26% and an absolute improvement of 10% (Fransen et al., 2015). Another review found that a moderate level of exercise can reduce knee pain and disability in those with osteoarthritis, and it does not lead to progression of disease (Bosomworth, 2009).
The type of exercises for people with knee osteoarthritis should preferentially be low-impact aerobic activities to minimise pain. These exercises include brisk walking, cycling, swimming, use of a cross-trainer and gardening. The Chief Medical Officer’s guidelines on physical activities for an adult recommend the following for major health benefits (Department of Health, 2011):
150 minutes of moderate-intensity aerobic activity per week; or 75 minutes of vigorous intensity aerobic activity per week
As a rough guide for patients, moderate intensity can be considered as exercise where you can still talk but not sing due to increased breathing. Vigorous intensity can be considered as exercise where you will have difficulty talking. A ‘start low’ and ‘go slow’ approach should be adopted for safe exercise. In addition to this, muscle-strengthening activities (e.g. resisted bands, weights), flexibility exercises (e.g. yoga, stretches) and balance exercises (e.g. walk backwards, stand on one foot, Tai Chi) two to three times per week should be incorporated. Figure 2 summarises this information.
Physical activity benefits for adults and older adults.
Physiotherapy
The main physiotherapy management for knee osteoarthritis, regardless of which compartment is affected, involves stretching and strengthening the quadricep, hamstring and calf muscles. A randomised controlled trial found that hydrotherapy classes and Tai Chi provided benefit in pain and function at 12 weeks in older patients with chronic hip or knee osteoarthritis (Fransen, Nairn, Winstanley, Lam, & Edmonds, 2007). Simple home exercises can be offered to patients as part of self-management (Fig. 3). However, some patients benefit from a physiotherapy referral, as they require more guidance and supervision.
Knee exercises.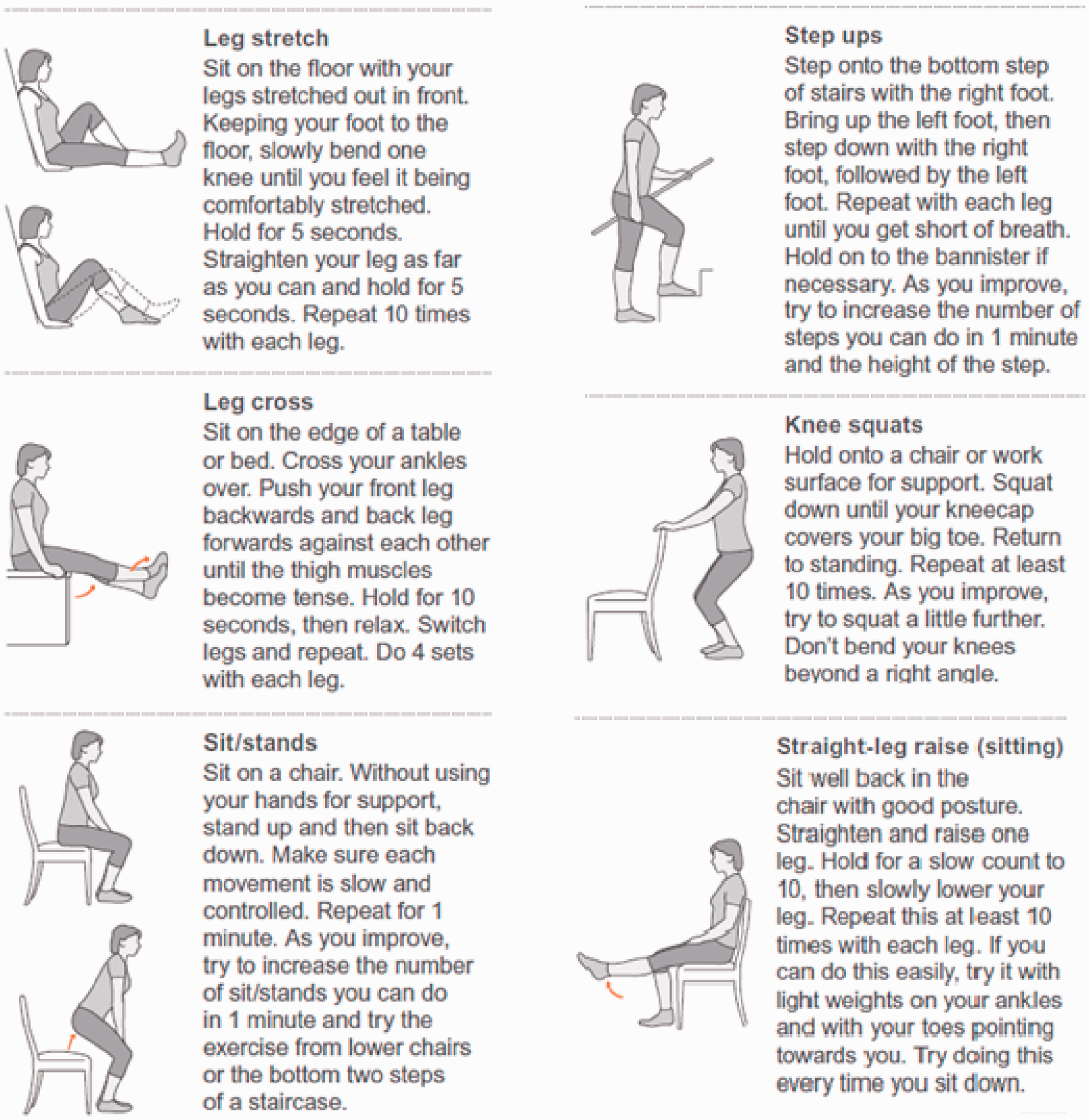
Analgesia
Paracetamol and or topical non-steroidal anti-inflammatories (NSAIDs) should be offered first line. Oral NSAIDs or opioids such as codeine can be considered if additional analgesia is required. Topical capsaicin can be used as an adjunct as recommended by NICE.
Intra-articular corticosteroid injections
NICE currently recommends intra-articular corticosteroid injections (CSIs) as an adjunctive treatment for moderate-to-severe knee osteoarthritis. A meta-analysis of CSIs for the treatment of knee osteoarthritis found evidence of short-term improvements in symptoms for up to 2 weeks, as well as a 16–24 week benefit in two high-quality studies (Arroll & Goodyear-Smith, 2004). However, a more up-to-date Cochrane review found unclear benefits of CSIs for knee osteoarthritis after 1–6 weeks and no evidence of an effect after 6 months (Juni et al., 2015). Therefore, it is important to counsel patients who wish to consider CSIs that it may not work at all, or it may only provide short-term benefit for pain and function.
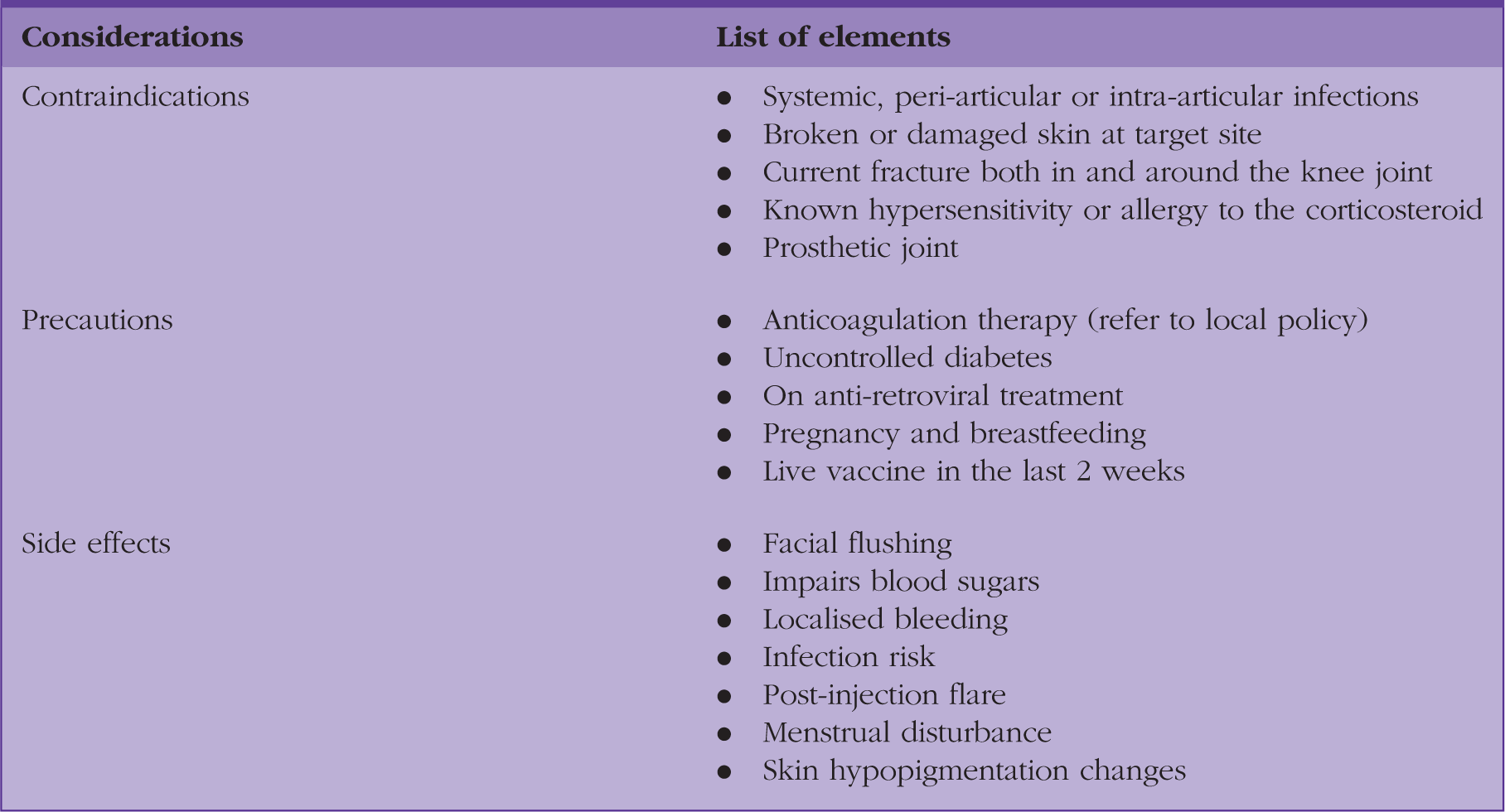
Contraindications, precautions and side effects of intra-articular CSIs.
Intra-articular hyaluronic acid
It is important to know about intra-articular hyaluronic acid (IAHA), as it has actually been in clinical use in some countries for 20 years or more and there is growing evidence for its use, so patients may enquire about it. Hyaluronic acid (HA) is a naturally occurring substance present in normal synovial joint fluid to help lubricate the joint. It is thought that patients with knee osteoarthritis have lower concentrations of HA that contributes to joint pain and stiffness, so therefore, injecting the joint space with exogenous HA (viscosupplementation) may reduce these symptoms (Wright, Maurer, & Di Cesare, 2000).
IAHA for knee osteoarthritis is currently not available on the NHS in the UK, but is widely used in the private sector and among some sportspeople. NICE guidelines state that the treatment is not cost-effective with various confounders in existing clinical trials.
An original Cochrane review found IAHA to be effective for pain, function and global assessment in knee osteoarthritis, especially 5–13 weeks post-injection (Bellamy et al., 2006). A more up-to-date meta-analysis of eight homogenous high-quality randomised controlled trials (2199 patients) found IAHA to reduce pain and improve function at 3 months in knee osteoarthritis (Richette et al., 2015).
Surgery
Arthroscopy
The arthroscopic procedures for knee osteoarthritis include lavage (joint irrigation) and debridement (removal of frayed cartilage or partial meniscectomies). A systematic review in 2015 found that debridement for knee osteoarthritis only offers a small inconsequential improvement in pain for up to a year and no statistically significant benefit in physical function (Thorlund, Juhl, Roos, & Lohmander, 2015). The review also highlighted that knee arthroscopy is associated with risks of deep vein thrombosis, pulmonary embolism, infection and death.
NICE does not currently recommend arthroscopy for knee osteoarthritis, due to lack of good evidence. Nevertheless, patients that present with true locking should be considered for arthroscopy solely to investigate and remove the underlying obstruction.
Osteotomy
Osteotomy is a procedure that involves breaking and then realigning bone. It can be performed in patients with medial unicompartmental knee osteoarthritis to offload the medial side of the joint and potentially correct any varus deformity.
Joint replacement
Referral for joint replacement surgery should be considered in patients whose symptoms significantly impact on their quality of life (e.g. persistent night pains) and they have not responded to non-operative interventions. NICE guidelines specify that patient-specific factors such as obesity should not be barriers to referral although the orthopaedic surgeon will take into consideration individual patient risk factors and suitability for surgery. For total knee replacement as many as 20% of patients might continue to endure knee pain (Carr et al., 2012), but on the whole it is a highly successful operation on selective patients.
Case study
Mrs JS, a 63-year-old lady, has attended your surgery with 2 years history of non-traumatic right-sided anterior knee pain that has gradually worsened over the course of 6 months. She has found it more difficult to climb stairs and feels that it sometimes gives way. She told you her knee swells up intermittently, particularly after prolonged walking. Her knee always feels stiff, but she did not describe any locking. She takes paracetamol and naproxen as required for the pain. Her past medical history includes hypertension and hypercholesterolaemia that are both well-controlled with medications. A GP colleague of yours saw the patient 6 weeks previous and organised a right knee MRI scan.
You reviewed the MRI report, it stated that all her ligaments are intact but there is evidence of moderate-to-severe osteoarthritis changes in the tibiofemoral compartments and a complex degenerative tear in the posterior horn of the medial meniscus. The report recommended an orthopaedic referral.
On examination of the patient: she had a body mass index of 31 kg/m2. There was no evidence of an antalgic gait. There was some loss of right quadricep muscle bulk. She has a mild effusion in the right knee. Her right knee actively flexed to about 100o (limited by pain and stiffness) but extension movement was full. Her power was 5/5 throughout. Her knee ligaments are all intact and she has a positive McMurray’s test on the right knee.
You explained to her about the diagnosis of right knee osteoarthritis and advise that she also has some degenerative changes to her meniscus, which helps to ‘absorb shock’ in the knee. You advised that the degenerative meniscus may require arthroscopy if locking symptoms develop.
You proceeded to discuss about management of knee osteoarthritis. The patient was quite happy with her current analgesia and did not want any additional medications. She was keen to start losing weight, but was worried about exercising with her knee pain. You advised her on strengthening and stretching the muscles around her right knee, and provided her with a knee exercise leaflet. Then you advised her on some low-to-moderate intensity exercises starting off with exercises that have less impact on the knee, such as swimming. You recommended at least 150 minutes per week of exercise.
Eight weeks after the initial consultation Mrs JS attends a follow-up appointment with you. She has managed to lose 3 kg of weight. She feels her knee is ‘stronger’ and no longer has any giving way sensations. Her stiffness has also lessened. Her pain is now more tolerable and she has less functional limitations. You discuss increasing her exercise levels further and other management options such as referral for physiotherapy knee classes and CSIs. She is keen to continue with her self-management and increase her weekly exercise frequency.
KEY POINTS
Knee osteoarthritis can be diagnosed clinically and further investigations are often not necessary Degenerative meniscal tears, muscle weakness, ligament laxity and Baker’s cysts are some conditions that may be associated with knee osteoarthritis Initial management of knee osteoarthritis should be conservative with exercise promotion, weight loss, functional knee exercises and analgesia Intra-articular CSI only provides short-term relief at best There is some evidence for IAHA, however, it is not routinely available on the NHS Orthopaedic referral is indicated if there are symptoms of true locking, or the symptoms of knee osteoarthritis are significant enough to warrant an opinion for corrective knee surgery or replacement