For organisations to remain successful they must adapt and change when necessary. Many GPs are not directly employed by the NHS, and work as independent contractors to provide services for the NHS. Changing demands from various stakeholders impact the work of individual general practices, and these demands, together with the economies of scale, have led to the development of new models of care. More GPs are now working collaboratively in GP federations or ‘super partnerships’. At scale working has been described by the RCGP for over 10 years and three quarters of GPs are currently estimated to be working collaboratively (Nuffield Trust, 2015). The Five Year Forward View presented ambitious plans for transforming services provided in the community (NHS England, 2015). Changes to the delivery of general practice are considered necessary to achieve the aim of transforming services in the face of projected shortfalls in funding (Deloitte, 2014).
Scale models
Many terms have been used to describe large-scale collaborations between GP practices such as ‘super-partnerships’, federations, networks, and multi-site practice organisations (Addicott and Ham, 2014; Curry and Kumpunen, 2015). The terms may reflect the different levels of financial and administrative ties between practices. For example, networks of practices may be loosely connected around common goals, but are otherwise independent of each other. Federations consist of two or more practices cooperating via a separate legal body (often with limited liability) but remain independent of each other, pooling part of their profits to support shared activities. The ‘super-partnership’ consists of two or more practices merged to form a new partnership, and although individual practices may run their own GP contract, responsibility lies with the larger umbrella partnership. Partners may be jointly liable for the actions of other members of the super-partnership. This model may allow the company to be limited by shares, hold contracts and limit the liability of individual partners. In multi-site practice organisations, practices are taken over by another practice or organisation and hold many GP contracts. The different models come with varying legal rights and responsibilities, financial liability and scope for profits (Pettigrew et al., 2016). The RCGP holds favourable views on health systems that keep a strong focus on primary care and provide high-quality outcomes at lower cost. The RCGP states that as professionals we should be adaptive to changing models of health care including ‘at scale’ delivery (RCGP, 2017). Quality improvements may involve many parameters of care, variations in care and different levels of health care. Any improvements should be sustainable.
Opportunities
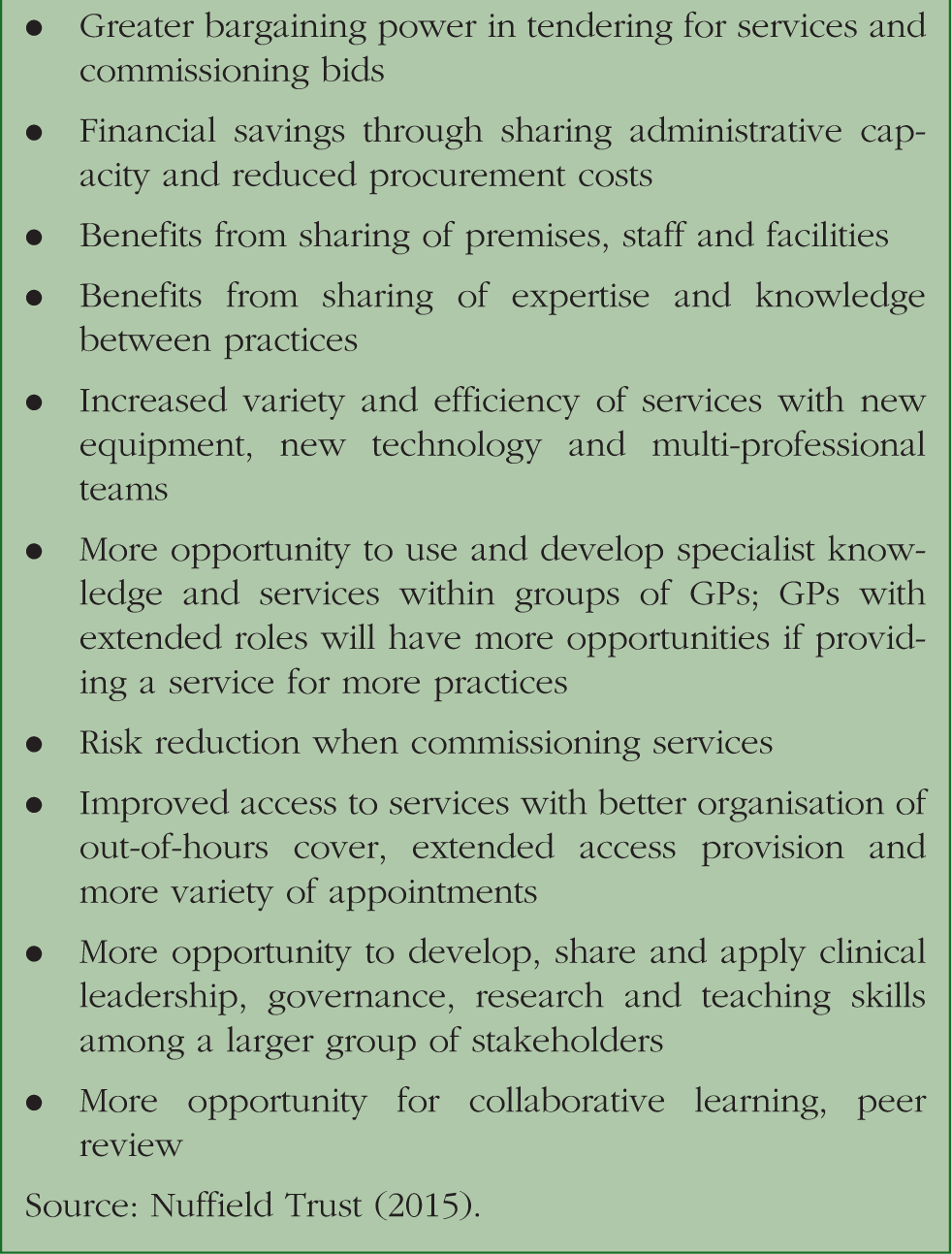
Change can offer opportunities. Box 1 outlines some of the opportunities of working at scale.
Possible advantages of working at scale.
• Greater bargaining power in tendering for services and commissioning bids
• Financial savings through sharing administrative capacity and reduced procurement costs
• Benefits from sharing of premises, staff and facilities
• Benefits from sharing of expertise and knowledge between practices
• Increased variety and efficiency of services with new equipment, new technology and multi-professional teams
• More opportunity to use and develop specialist knowledge and services within groups of GPs; GPs with extended roles will have more opportunities if providing a service for more practices
• Risk reduction when commissioning services
• Improved access to services with better organisation of out-of-hours cover, extended access provision and more variety of appointments
• More opportunity to develop, share and apply clinical leadership, governance, research and teaching skills among a larger group of stakeholders
• More opportunity for collaborative learning, peer review
The GP Forward View (NHS England, 2016) suggests that £500 000 000 of additional funding by 2020–21 is required to improve extended access through Primary Care Access Hubs, offering additional clinical capacity across groups of practices (NHS England, 2016). With practice closures increasingly frequent, and 93% of GPs expressing concern over financial sustainability (Future focussed finance and HFMA, 2017) change towards collaborative working may seem inevitable. The GP Forward View (NHS England, 2016) encourages scale working, suggesting that almost £250 000 000 is available for Clinical Commissioning Groups to support practices in transforming and implementing service redesign. With fewer GPs, rising workloads and a necessity to evolve multi-professional clinical teams, choosing not to work at scale may become increasingly difficult. Box 2 gives an outline example of a federation of practices.
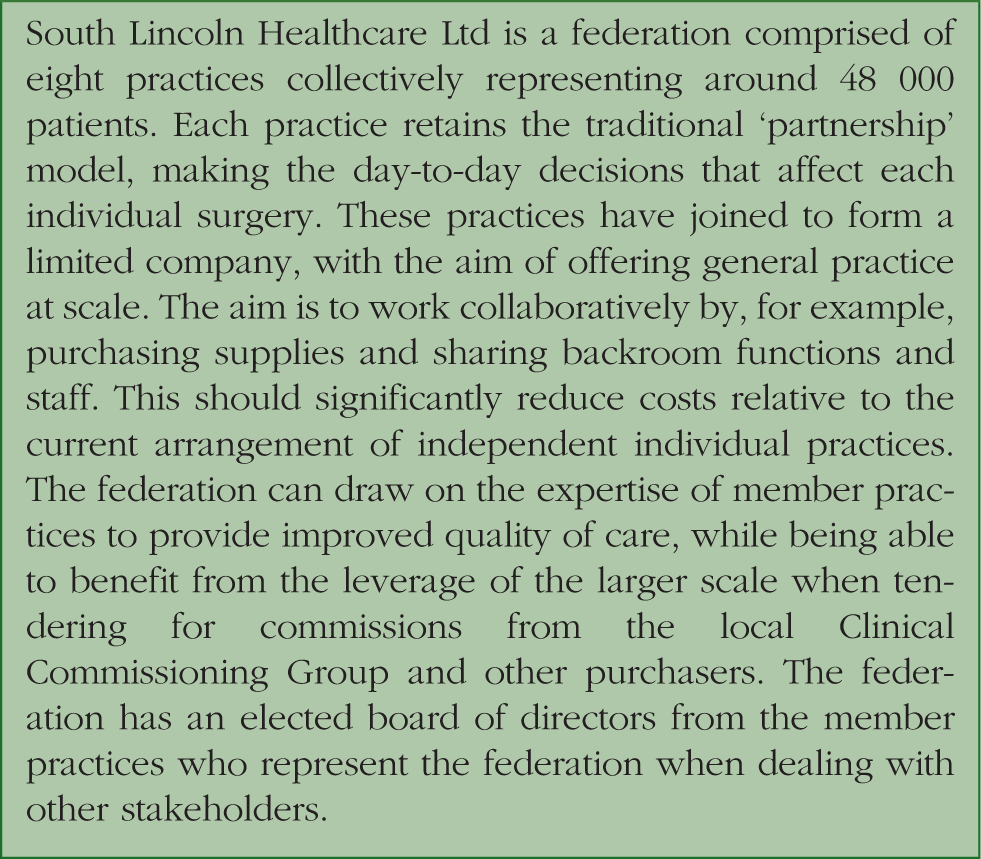
Example of a federation.
South Lincoln Healthcare Ltd is a federation comprised of eight practices collectively representing around 48 000 patients. Each practice retains the traditional ‘partnership’ model, making the day-to-day decisions that affect each individual surgery. These practices have joined to form a limited company, with the aim of offering general practice at scale. The aim is to work collaboratively by, for example, purchasing supplies and sharing backroom functions and staff. This should significantly reduce costs relative to the current arrangement of independent individual practices. The federation can draw on the expertise of member practices to provide improved quality of care, while being able to benefit from the leverage of the larger scale when tendering for commissions from the local Clinical Commissioning Group and other purchasers. The federation has an elected board of directors from the member practices who represent the federation when dealing with other stakeholders.
Challenges
Change brings challenges. Delivering general practice at scale presents challenges. At a practice level, staff and patients may find changes to working practices difficult, citing, for example, concerns about loss of a ‘personal touch’, continuity of care and knowledge of patients. Staff may have concerns about employment status, terms and conditions of employment, contract variations, training costs and professional indemnity. If a number of practices agree to pool resources and buy equipment or employ new staff, how will they share the costs between practices of differing size and organisational complexity? How will practices accommodate practices joining or leaving the organisation? With more clinical staff and more patients will practices have more influence on the configuration of services? Can this generate conflicts of interest? Box 3 summarises some of these issues. Such change might be seen as requiring a leap of faith, and practices may, understandably feel that they are venturing into the unknown. Help and advice is available from the British Medical Association, RCGP and Nuffield Trust. Robust professional, legal and accountancy advice is recommended for practices considering such arrangements.
Possible disadvantages of working at scale
• Reduced continuity of care and loss of ‘personal touch’ for patients
• Demotivating effect caused by dilution of effort and reward
• Loss of a sense of responsibility; ‘collusion of anonymity’
• Loss of partnership autonomy and ownership
• Weakening of the partnership model with fewer partners and more employed, less engaged GPs
• Domination of one practice over another
• Problems arising from sharing staff and facilities: Professional indemnity, insurance, cost-sharing, etc.
• Problems arising from practices leaving or joining the group
• Increased potential for conflicts of interest
• Performance review: Who is responsible for a struggling practice in the group?
• Risks posed by the failure of bigger practices, groups of practices
The NHS is 70 years old, but the primary care model has barely changed. How new models of care and Sustainability and Transformation Partnerships may look is uncertain, but the current landscape offers an opportunity for GPs working at scale to evolve their contractual relationship with the NHS, working with other health care professionals and providers in a much more integrated way. Any decision to work at scale requires the development of trust, new working relationships and consideration of how collaboration might benefit the parties involved.
Changes
Constant cycles of change within the NHS can give rise to cynicism and questions about the cost of reorganisation. GPs must not only update clinical knowledge, but also maintain an understanding of political and organisational changes that affect the delivery of primary care.
Federations, super-partnerships and other at scale models may provide opportunities to improve health care. Working at scale will affect most, if not all, GPs. It will impact on clinical work and patients as well as having financial and legal implications. It may offer an opportunity to improve the sustainability of the GP profession and improve and evolve the type of care offered to patients. New ways of working at scale are being developed. No single model will suit all practices. There are possible disadvantages and challenges posed by working at scale. Proposed new models of care cannot be ignored and engagement with change may help address challenges and shape the future of general practice.
Curry N and Kumpunen S (2015) Network, federation, super-partnership or multi-practice organisation? A guide to GP provider organisation terminology. Nuffield Trust. Available at: www.nuffieldtrust.org.uk/health-and-social-care-explained (accessed 24 October 2018).