
Abstract
It has been suggested that the focused clinical examination should be claimed as a specialist GP skill. Integral to this objective is the ability to select and interpret an examination to accurately support the diagnostic process. This article will introduce you to evidence-based physical examination (EBPE), and how it can be used in your day-to-day work with patients. You will learn how to make evidence-based and efficient use of the physical examination, while also improving your skills in diagnosis. The connection between information gathered in history taking, the development of diagnostic hypotheses, and the choice of specific examinations to confirm or refute these hypotheses will be explored using simple clinical scenarios. You will be introduced to the statistical tools used in EBPE that enable you to make an estimation of the likelihood of a patient having a particular diagnosis once the examination has been performed.
The GP curriculum and physical examination
Formulate a clinical hypothesis and then use the skills of effective consultation and examination skills to prove or disprove a diagnosis or hypotheses.
Why use evidence-based physical examination?
Physical examination remains an important skill for GPs as they work to establish diagnoses in their patients, without having ready access to the imaging and other technologies available in hospitals. With increasing demands in the consultation and patients presenting with a wide range of undifferentiated problems, it is crucial that GPs are able to select and perform examinations and interpret their findings accurately as part of their clinical decision making.
During the consultation, taking a history and employing clinical reasoning results in the development of diagnostic hypotheses. Evidence-based physical examination (EBPE) allows the diagnostic significance of a particular physical examination finding to be calculated, and, armed with this information, the findings from a relevant, focused examination will help to support or refute diagnostic hypotheses.
Statistical tools used in EBPE
EBPE uses the following tools: sensitivity and specificity, likelihood ratios, and pre- and post-test probabilities. When approaching EBPE for the first time, it is helpful to have an understanding of these tools and how they may be used in clinical practice.
Understanding sensitivity and specificity
Sensitivity and specificity describe the discriminatory power of physical signs. They are defined as follows:
Sensitivity is the proportion of patients with the diagnosis who have the finding (i.e. the probability that a finding is present in a person with the disease) Specificity is the proportion of patients without the diagnosis who do not have the finding (i.e. the probability that a finding is absent in a person without the disease)
In practice, the sensitivity and specificity of a test cannot be used to estimate the probability of disease in an individual patient. However, they can be combined into a single measure that is clinically more useful, the likelihood ratio.
Understanding likelihood ratios
Likelihood ratios (LRs) are used to assess the utility of a particular examination (or other diagnostic test) based on how likely or unlikely it is that a patient has a diagnosis (or disease). LRs can be positive or negative.
Calculating likelihood ratios.

LRs can be used to estimate an individual patient’s likelihood of having the diagnosis once the result of the examination is known, but this requires calculation of pre- and post-test probabilities, which are explained below.
Estimating the pre-test probability (before the examination)
Having taken the patient’s history, you may have a diagnosis in mind (your hypothesis) and you need to decide which examination you are going to perform. You will usually have a rough idea of how likely it is that the patient has the diagnosis. This will be based on various factors such as the patient’s history and symptoms, your clinical experience and/or your knowledge of local or national prevalence data. This estimated probability of the diagnosis before the examination is called the pre-test probability. A useful technique to practice this skill is to commit to estimating the probability of the diagnosis as low (20%), medium (50%) or high (80% or above) (Mookherjee et al., 2015).
Estimating the post-test probability (after the examination)
Once the examination has been performed, then if a particular finding is present, the probability of the diagnosis may be increased. If the finding is not detected, the probability may be reduced. The patient’s likelihood of having the diagnosis after the examination is the post-test probability.
LRs can be used in conjunction with pre-test probability for diagnosis, to estimate an individual’s post-test probability of the diagnosis, which is the likelihood of the patient having the diagnosis once the result of the examination is known.
In summary, the pre-test probability is your estimate of how likely it is that the patient has the diagnosis before the examination is performed. Post-test probability is a patient’s chance of having the diagnosis once the result of a test is known. It is calculated using the pre-test probability and a suitable graphical tool.
Estimating post-test probability: Simple tool.
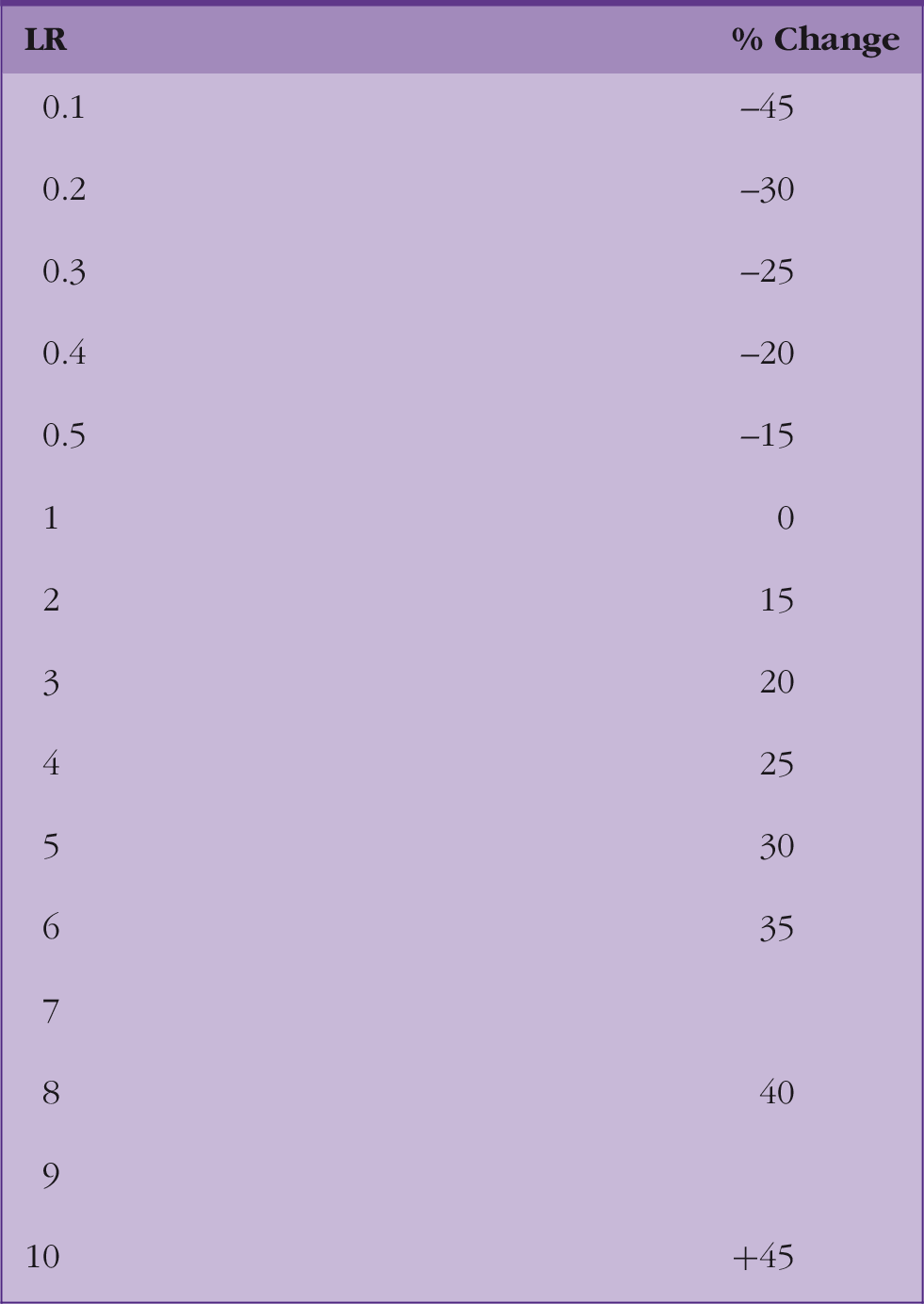
Source: McGee (2002).
Estimating post-test probability.

Some clinical examples to illustrate the use of EPPE
How can EBPE help you in the diagnosis of pneumonia?
Community-acquired pneumonia: likelihood ratios.

Source: Kihlberg and Hammer (2017a).
Finding dullness to percussion on examination will increase the probability of pneumonia by about 25%; but the absence of this finding does not convincingly make the diagnosis any less likely. The presence of a cough adds nothing to the diagnostic process because the LR has a value of one.
Suspected anaemia
Chronic anaemia: likelihood ratios.
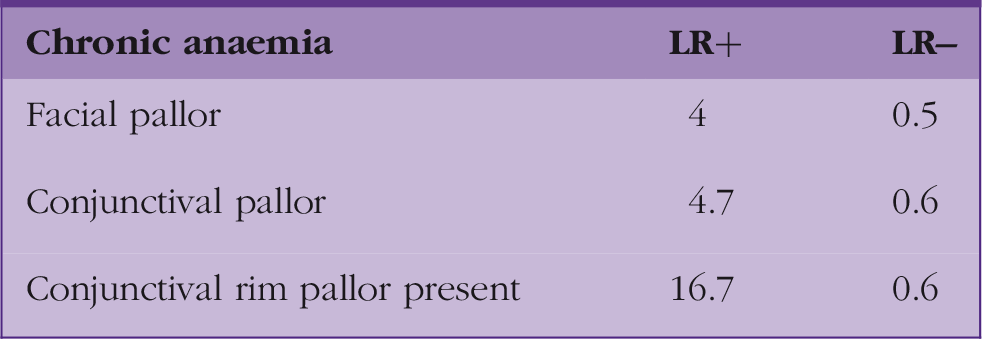
Source: McGee (2012).
Any of these findings increases the probability of anaemia, but finding conjunctival rim pallor is the most useful, increasing the probability by at least 45%. Importantly, none of these physical signs convincingly decreases the probability of anaemia if not present i.e. no LR less than 0.4.
Acute abdominal pain
Appendicitis: likelihood ratios.
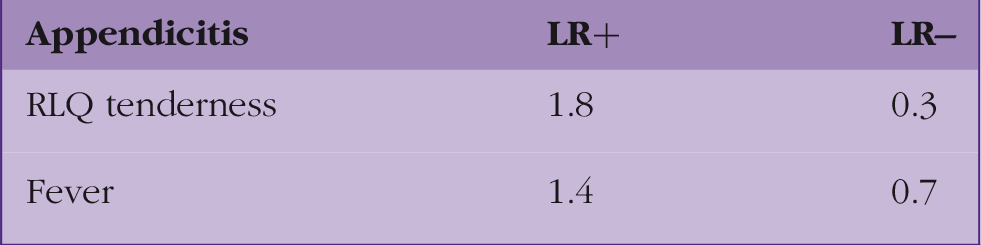
Source: Bundy et al. (2007).
In patients with acute abdominal pain, the absence of RLQ tenderness is more useful in reducing the probability of acute appendicitis (–25%) than a positive sign is in increasing the probability (+15%). The presence of fever is not particularly helpful in either increasing or reducing the probability of the diagnosis.
Sinusitis
Acute sinusitis: likelihood ratios.

Source: Kihlberg and Hammer (2017b).
The history of a preceding upper respiratory tract infection (URTI) has very little effect on the probability of this patient having acute sinusitis. The presence of facial pain adds nothing to the diagnostic process because the LR has a value of one. The presence of maxillary toothache increases the probability of the disease by 15–20%. This case illustrates the same statistical tools can be used with symptoms, as well as examination findings.
What are the limitations of EBPE?
EBPE requires that the clinician is competent to perform physical examinations accurately, elicit signs and interpret the findings. Estimation of the pre-test probability by an individual clinician inevitably introduces a degree of subjectivity.
The accuracy of a LR depends entirely upon the relevance and quality of the studies that generated the numbers (sensitivity and specificity) that inform that calculation of LRs. Furthermore, LRs demand that there is a focus on one single finding, which is counter-intuitive to the usual clinical approach of simultaneously absorbing multiple factors and impressions to arrive at a diagnosis.
Some authors promote the use of LRs sequentially i.e. using one LR to generate a post-test probability, and then using this as a pre-test probability for application of a different LR to arrive at a more accurate probability of diagnosis. The caveat is that the clinical findings being combined must be independent i.e. have distinct pathological mechanisms (McGee, 2012: 20–21). Others argue that LRs have never been validated for use in series or in parallel (www.thennt.com).
Getting started with EBPE in your practice
This article has highlighted the important role of physical examination and the judicious choice of specific examinations to support the process of making a diagnosis. In practice, you will be able to apply this knowledge to aid your clinical decision making. There are some excellent resources that can provide you with the information (LRs) that you need to get started; details are included in ‘References and further information’. You may choose to begin by applying the EBPE approach to a small number of commonly seen clinical scenarios. Once you are armed with some of the most useful LR+ and LR–for your chosen scenarios, there should be no stopping you!
Key Points
Have a diagnosis in mind before you start the examination Estimate the pre-test probability Perform a focused examination, the choice of examination being driven by your diagnostic hypothesis. Consider the LRs for the examination Calculate the post-test probability using your pre-test probability and the LRs Make a diagnosis and plan management