
Abstract
The menopause is a normal life event for women and not an illness or medical condition. Despite this, menopause can predispose vulnerable women to distressing symptoms that impact adversely on their quality of life and to long term medical conditions such as osteoporosis, cardiovascular disease and dementia. Many healthcare professionals are uncertain about the management of the menopause, and this leads to many women not receiving treatment which is often beneficial to them. This article will cover the diagnosis of the menopause including premature ovarian insufficiency. Some of the health risks of the menopause will be discussed and treatment of the menopause, with a particular focus on hormone replacement therapy, will be covered in detail.
The GP curriculum and the menopause
Recognise and manage common medical conditions encountered in generalist medical care. It includes safe prescribing and medicines management approaches Demonstrate an understanding of the importance of risk factors in the diagnosis and management of women’s problems Know how the social and biological features of the perimenopause and menopause period interact and affect heath, social well-being and relationships (e.g. mood swings, anxiety and depression, reduced libido) Be able to advise on prevention strategies relevant to women (e.g. osteoporosis)
Background
Definitions.
In the early-1900s the average age of the menopause was 57 years, and a woman’s life expectancy was around 59 years. However, the average age of the menopause is now 51 years and a woman’s life expectancy is around 82 years. This means that many women are postmenopausal for around 30 years or more, which can have a negative impact on the quality of their lives.
Many women are affected by symptoms of their menopause, often to the detriment of their families, work and life in general. In addition, many women do not realise that there are health risks to having low oestrogen levels in their bodies; these include increased risk of cardiovascular disease and osteoporosis. The predisposition to cardiovascular disease is due to an adverse effect on lipids, lipoproteins, insulin resistance and arterial compliance. Loss of bone density, and ultimately osteoporosis, occurs due to an increase in bone breakdown by osteoclastic activity which exceeds bone formation by osteoblasts.
Guidelines on the menopause were published in November 2015 by The National Institute for Health and Care Excellence (NICE) and menopause care in the UK should be based on these guidelines (NICE, 2015a). These are the first clinical guidelines on menopause to be produced by NICE and provide clear recommendations on both the diagnosis and treatment of women with menopausal symptoms.
Symptoms of the menopause
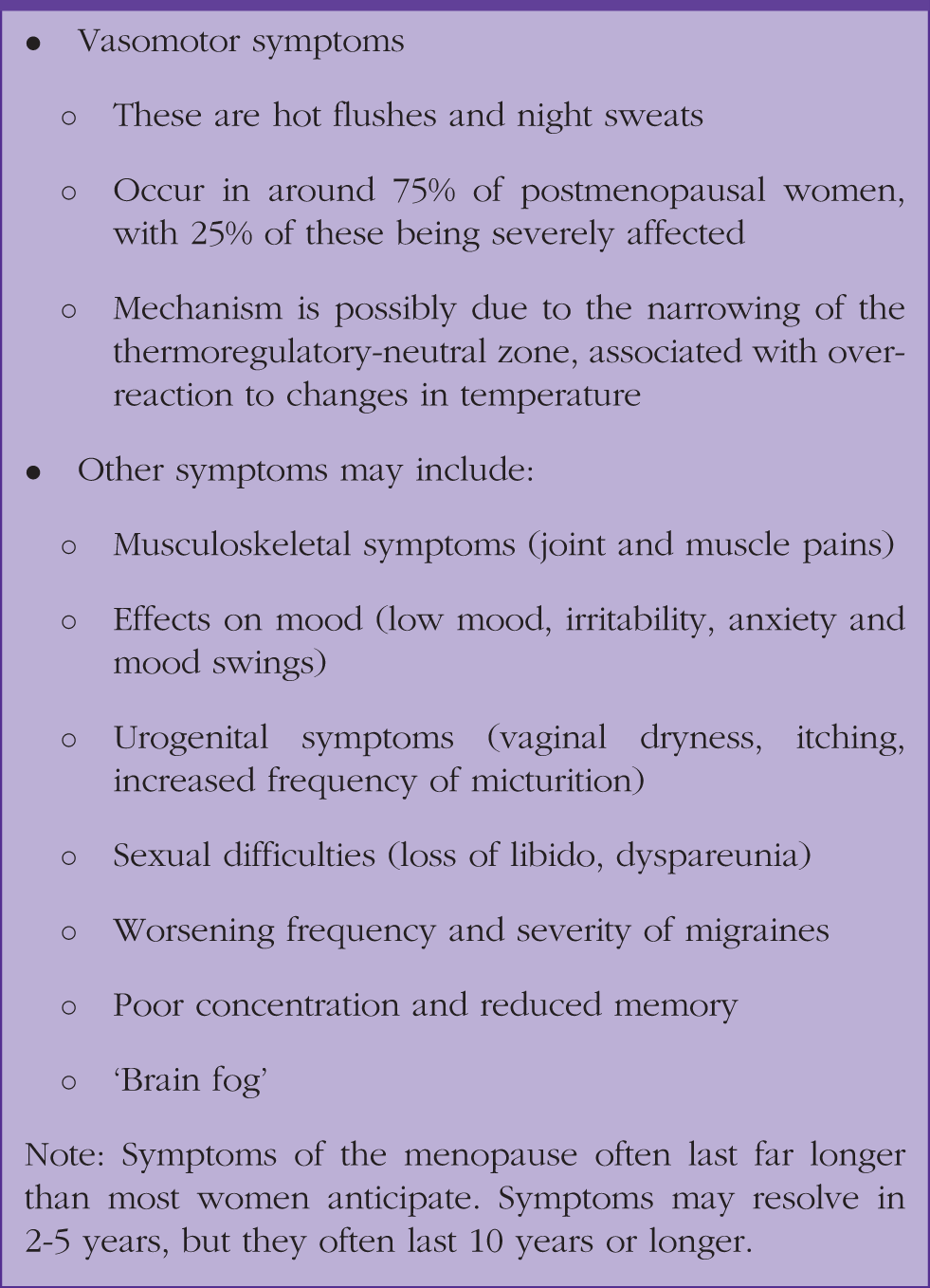
The majority of women experience symptoms of the menopause; however, they vary between women and often fluctuate during the months. Many women do not even recognise some of their symptoms as being related to the perimenopause and menopause. The psychological symptoms of the menopause are the ones that usually affect women the most, and are often misdiagnosed as depression.
Common symptoms of the menopause.
Urogenital atrophy
The term vulvovaginal atrophy (VVA) (or atrophic vaginitis) is often used to describe symptoms that can arise due to vaginal dryness, but it does not include the urinary symptoms that frequently occur in people with VVA. The term genitourinary syndrome of the menopause (GSM) is increasingly used, as this includes the urinary symptoms which often also occur (Portman et al., 2014).
Suggested questions to ask regarding making a diagnosis of GSM.
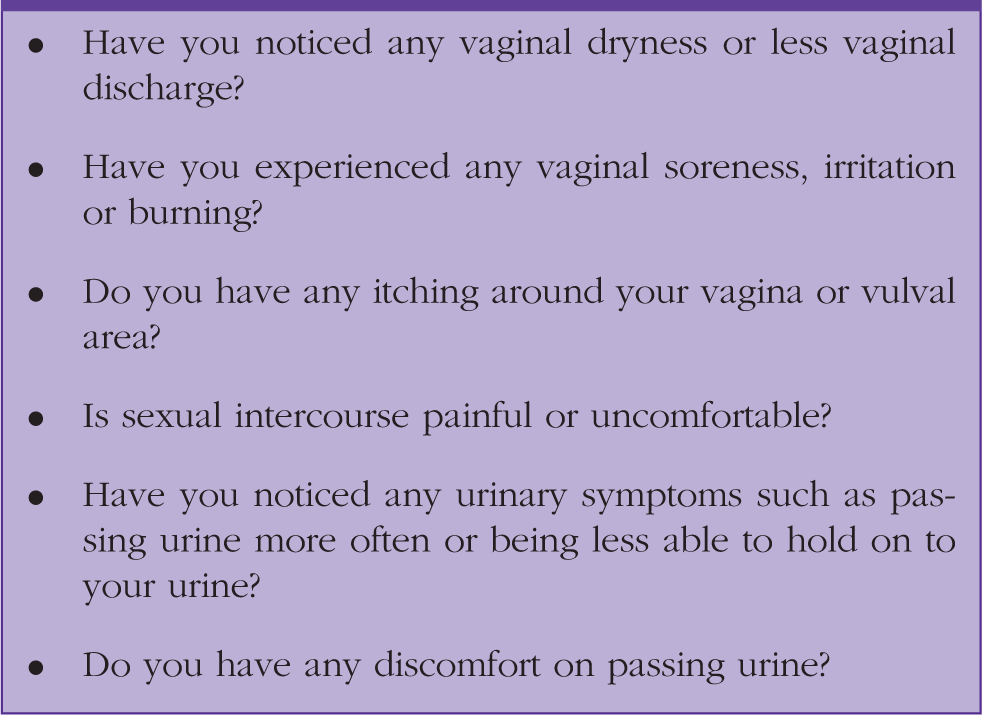
As there are oestrogen receptors present in the vagina, urethra, bladder trigone, and pelvic floor, a lack of oestrogen can affect all these areas. The most common symptom of GSM is usually vaginal dryness, which can lead to dyspareunia. However, GSM is very common in women who are not sexually active, so it is important to also ask these women about these symptoms. Other symptoms can include vaginal irritation and itching, which can interfere with sleep, general enjoyment of life, and mood. Many patients have discomfort exercising, walking or even sitting down. Although many other menopausal symptoms improve with time, symptoms of GSM often worsen with age.
The vaginal mucosa can become drier, thinner, less elastic, and more fragile. There is often a decline in vaginal secretions and a decreased production of glycogen from the vaginal epithelium, which when associated with an increase in vaginal pH can increase the risk of local infections such as bacterial vaginosis and thrush (MacBride et al., 2016).
Making a diagnosis of menopause
NICE recommendations regarding diagnosis of the menopause.
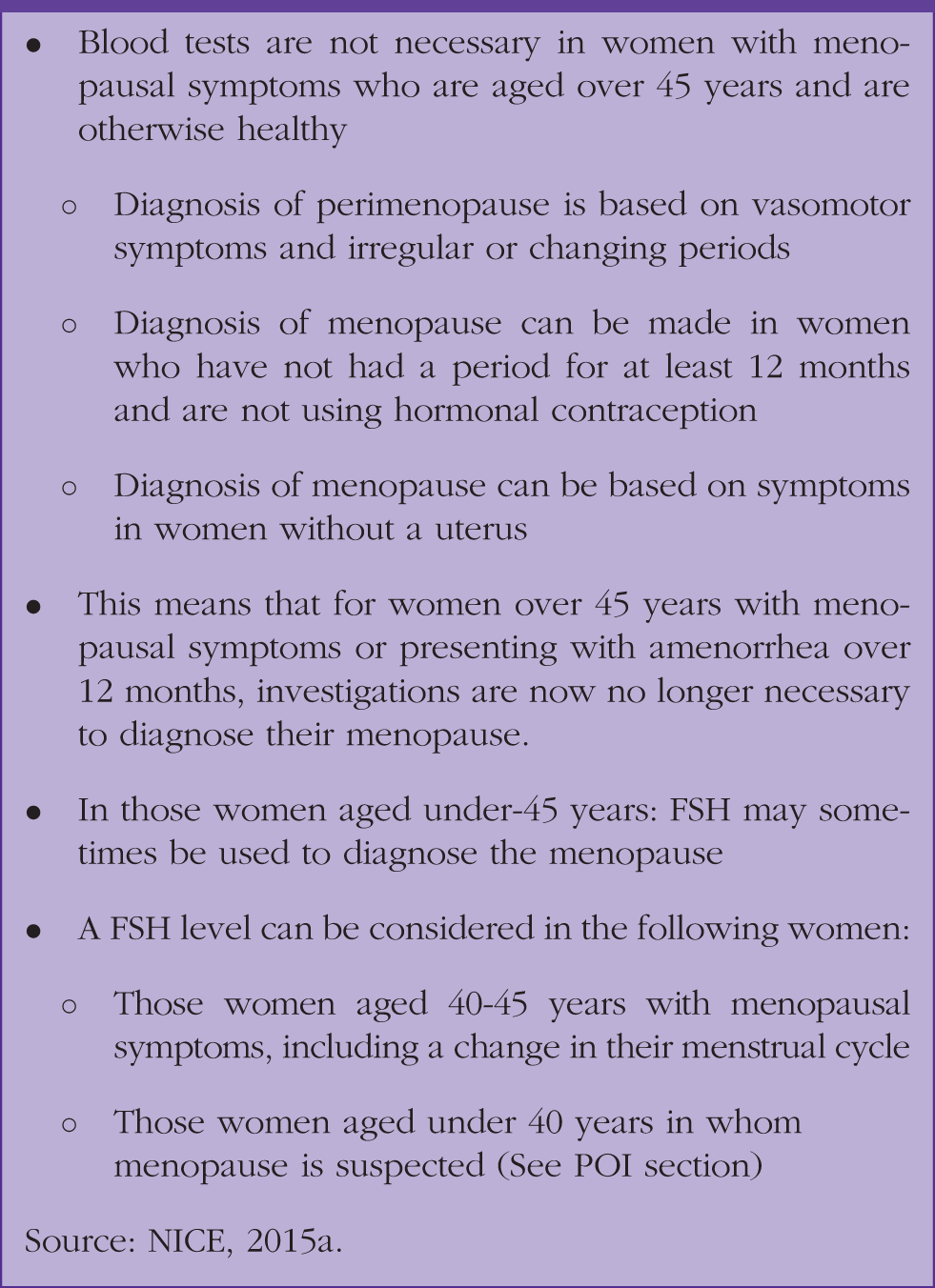
Follicle-stimulating hormone (FSH) measurements in the perimenopause in women over 45 years in age are not precise, as they fluctuate considerably over short periods of time. This means that they can be falsely reassuring.
Approximately 70% of FSH tests are currently performed in women over the age of 45 years, which is no longer appropriate. Reducing the number of FSH blood tests has the potential to bring significant cost savings to the NHS; it has been estimated that reducing unnecessary FSH testing could lead to a national saving of £9 600 000 (NICE, 2015b).
A FSH test may be useful in women below the age of 45 years to confirm the diagnosis of menopause; it can also be instructive regarding the ongoing requirement for contraception. This is particularly helpful in women on progestogen-only contraception, for example, levonorgestrel intrauterine system, who may not be having periods. Women on combined hormonal contraception should be advised to stop treatment for at least 6 weeks before having a FSH level taken (FSRH, 2017).
Other tests are largely unnecessary. This means that in practice women can start treatment sooner, which will be advantageous for many women, especially those with more severe symptoms.
Individualised care
When discussing menopause with women, it is very important that they receive individualised care, so their individual risks are discussed in the consultations. Women should receive appropriate information, ideally written, which will enable them to make informed choices regarding the treatment they receive. Receiving this information will help to enable them to make informed choices regarding the treatment they receive. They should also be signposted to accurate and appropriate websites.
This information should include:
An explanation of the stages of menopause Common symptoms and diagnosis Lifestyle changes and interventions Benefit and risks of the range of treatments for menopausal symptoms Long-term implications of menopause
This individualised approach should be undertaken at all stages of diagnosis, investigation and management of menopause. Any treatment and care given to women should consider individual needs and preferences. When relevant, information about contraception should be given.
Management of the menopause
An informative consultation about the menopause should be seen as an ‘opportunity’. This is because correct medical intervention and advice at this point of life can offer women years of benefits from preventive healthcare.
Useful websites.

Hormone replacement therapy (HRT) is only one part of the management of perimenopausal and menopausal women. For women who cannot take HRT or do not want to take HRT then there is some evidence that medication such as selective serotonin receptor inhibitors and selective noradrenaline receptor inhibitors can be beneficial (NICE, 2015a). However, these should not be offered as first line treatment for vasomotor symptoms (VMS), particularly if mood symptoms are not present.
Management of vasomotor symptoms
HRT is the most effective treatment currently available for the management of VMS of the perimenopause and menopause, improving VMS in at least 90% of women. The actual choice of preparation varies according the individual woman, their medical history and their personal choice.
There is poor evidence regarding other products such as isoflavones, black cohosh or compounded bioidentical hormones, and the safety of many of these products is still uncertain. Compounded bioidentical hormones are not regulated or licensed and not evidence-based for efficacy and safety.
Testosterone is still not licensed for use in women in the UK. However, it does have a role for those women who still have low libido despite receiving HRT (Achilli et al., 2017). Testosterone can also help to improve mood, energy and concentration (Glaser et al., 2011). Any psychosexual issues should be addressed before prescribing testosterone for low libido. It is important that physiological female doses are used in order to avoid the virilising effects of high doses. Restoration of appropriate female physiological testosterone levels is not associated with significant adverse effects and is supported by the NICE menopause guideline (NICE, 2015a).
Management of the symptoms of the menopause
Many clinicians and women understand the benefits of HRT for managing the classic symptoms of the menopause, hot sweats, flushing, tiredness, but may be less good at understanding that HRT can also improve the other symptoms of the menopause. Correcting low oestrogen levels improves the majority of menopausal symptoms and women often find that they feel considerably better within a few months of taking HRT.
Low mood
NICE states that healthcare professionals should consider prescribing HRT to alleviate low mood that arises as a result of the menopause (NICE, 2015a). Cognitive behavioural therapy may also be beneficial for some women. There is no clear evidence that antidepressants improve low mood in perimenopausal women who do not have depression, so they should not be used in these situations.
Urogenital atrophy
Some women present during or after their menopause with symptoms of urogenital atrophy; one of the commonest symptoms is that of recurrent urinary tract infections with negative urine cultures. These symptoms are often effectively managed by giving women topical vaginal oestrogen.
NICE guidance states that vaginal oestrogen should be offered to women (including those on systemic HRT) with symptoms of urogenital atrophy and then continued for as long as needed to relieve symptoms (NICE, 2015a). A year’s supply of topical oestrogen is equivalent to having one tablet of HRT. This means that vaginal oestrogens can be safely given as a repeat prescription. Women using long-term low dose topical oestrogen do not require progesterone, as there is no endometrial stimulation.
Vaginal moisturisers and lubricants should also be given, either alone or in conjunction with vaginal oestrogen (NICE, 2015a). Moisturisers should be used regularly, as a treatment to rehydrate the vaginal tissues and increase moisture (Edwards and Panay, 2016). Lubricants are recommended prior and during sexual intercourse and do not need to be used on a regular basis. The type of lubricant and moisturiser is important; they should be balanced for pH and osmolality in order to achieve optimum efficacy and to avoid adverse effects.
Starting HRT
Women need to be made aware that the HRT benefits and risks vary by dosage, regimen and timing of initiation. They need to be informed that vaginal bleeding may occur in the first 3 months of treatment. The initiating dose should be judged based on the severity of symptoms, the age of the woman and also her individual circumstances. Younger women are more likely to need higher doses of HRT than older women.
Prescribing HRT
The preparations are usually oral or transdermal and then are sequential or continuous combined. Oestrogen can be given unopposed or combined with a progestogen. Women with an intact uterus need to take oestrogen and progestogen, whereas women who have had a hysterectomy only need to take oestrogen. The Primary Care Women’s Health Forum (PCWHF) has produced a useful flowchart regarding prescribing HRT (Fig. 1).
PCWHF’s flowchart for HRT prescribing.
In general, women who have not had a period for at least a year, and also women who have taken a sequential preparation for at least a year, can be given continuous combined HRT. Taking a continuous preparation means that the women should not have any more periods, although initial breakthrough bleeding is not uncommon.
Women who wish to achieve a continuous combined regimen in the perimenopause and/or have problematic periods can have a levonorgestrel intrauterine system inserted, which will give excellent endometrial protection and provide contraception where required.
Benefits of HRT
HRT is often very effective at improving VMS and other menopausal symptoms, including reduced libido. Many women notice their skin, hair, joints and generally well-being also improve dramatically with taking HRT.
Health benefits of HRT
Cardiovascular disease
The risk of cardiovascular disease (CVD) greatly increases after the menopause and CVD is the most common cause of death in women worldwide. Studies have shown that there is a lower incidence of CVD in those women who take HRT within 10 years of their menopause. A meta-analysis showed that for women taking HRT within 10 years of their menopause there is a 0.70 relative risk reduction of all-cause mortality and a 0.52 relative risk reduction of coronary heart disease mortality (Boardman et al., 2015).
The CVD benefit of taking HRT is greatest the earlier a woman starts HRT. A large Finnish study has shown that using any HRT for at least 10 years is associated with 19 fewer coronary heart disease (CHD) deaths and seven fewer stroke deaths per 1000 women (Mikkola et al., 2015a).
The NICE guidance states that women should be informed that HRT with oestrogen alone is associated with no, or a reduced, risk of CHD and that HRT with oestrogen and progestogen is associated with little or no increase in the risk of CHD. In addition, the presence of cardiovascular risk factors is not a contra-indication to HRT (NICE, 2015a). It is essential to optimally manage any underlying cardiovascular risk factors (e.g. hypertension, high cholesterol) in women taking HRT. However, having hypertension is not a contra-indication to having or continuing HRT.
This means that having raised blood pressure is not a contra-indication to taking HRT, nor a reason to stop prescribing HRT. Elevated blood pressure should be addressed and promptly managed in women as it is for women who are not taking HRT.
Osteoporosis
Fracture incidence increases in women at the menopause, coinciding with lower oestrogen levels, a decrease in bone mineral density (BMD) and higher rates of bone turnover. In the UK alone, annual hospital costs associated with osteoporotic hip fractures are estimated to be £1.1 billion (Leal at al., 2016). The prevention of fractures in postmenopausal women is a vital public health priority worldwide.
Oestrogens are a very effective way of increasing BMD and also preventing osteoporotic fractures in women (Zhu et al., 2016). Consistent evidence from both randomised and cohort studies has demonstrated that the risk of any fragility fracture and non-vertebral fracture is significantly lower for women currently taking HRT (either oestrogen alone or for the combination of oestrogen plus progestogen) compared with non-users (Marjoribanks et al., 2012).
Dementia
Some studies have suggested that HRT might impact the risk of dementia, although this requires confirmation (Imtiaz et al., 2017; Mikkola et al., 2017). There is some evidence that there may be a window of opportunity for lowering the risk of dementia with HRT for women with specific preconditions e.g. if they have first-line relatives with dementia, or for women who have premature ovarian insufficiency (Podfigurna-Stopa et al., 2016). NICE recommend that an explanation is given to menopausal women that the likelihood of HRT affecting their risk of dementia is currently unknown (NICE, 2015a).
Risks of HRT
Much of the negative publicity surrounding HRT arises from misinterpretation by the media of the findings from the Women’s Health Initiative (WHI) study that was published 15 years ago (Rossouw et al., 2002). Many women and healthcare professionals do not realise that many women taking HRT live longer, healthier lives than those who do not take HRT (Anderson et al., 2012).
Stroke and venous thromboembolism risk
There is a low risk of stroke and venous thromboembolism (VTE) in women taking oral HRT. The increase in risk of VTE in those taking oral oestrogen is approximately twofold (Oger et al., 2003). This increased risk is far lower than that experienced when taking the combined oral contraceptive pill or with pregnancy. The background risk of VTE increases with increasing age. Women should be made aware that the baseline population risk of stroke in women aged under-60 years is very low.
In contrast, there is no evidence that using standard or low-dose transdermal HRT increases the risk of stroke or of VTE (Canonico et al., 2008). Transdermal preparations of oestrogen should be considered for those women with a higher risk of VTE, including those with a body mass index greater than 30 kg/m2 (NICE, 2015a).
Breast cancer and HRT
When women are asked about reasons not to take HRT, the most common answer is their concern about the perceived increased risk of breast cancer. Women taking oestrogen-only HRT do not have an increased risk of breast cancer, which is illustrated in Fig. 2. It is only when a progestogen is added to the oestrogen-primed breast tissue that there appears to be an increased risk over a long period of time (Stanczyk et al., 2013). Meta-analysis of the random controlled trial data in the NICE menopause guideline suggests that the excess risk is no more than one extra case per 1000 women per year beyond the average age of menopause (NICE, 2015a). Young women under 51 years in age and taking combined HRT do not have an increased risk of breast cancer.
Cumulative hazards, which have been adjusted for age and ethnic group, of invasive breast cancer by random allocation in the WHI trials of conjugated equine oestrogen alone and conjugated equine oestrogen plus medroxyprogesterone acetate trials.
Epidemiological data support the hypothesis that progestogens are not a uniform class, and that progesterone and progestogens have different effects on the risk of breast cancer in menopausal women using HRT. There is some evidence to suggest that certain synthetic progestogens, such as medroxyprogesterone acetate, may increase breast cancer risk when used in combined HRT and when compared with using micronised progesterone or dydrogesterone (Lyytinen et al., 2009; Fournier et al., 2005). Natural progesterone is micronised, or reduced to tiny particles, and mixed with oil so that it is better absorbed.
An important learning point is that taking HRT does not affect the risk of dying from breast cancer. Women need to be made aware that the increased risk of breast cancer is lower than being overweight or having two glasses of wine each night. Modifiable risk factors for breast cancer, such as obesity, lack of exercise and alcohol intake, should all be taken into consideration and discussed with a patient. Many women find that their lifestyles improve after taking HRT, so their future risk of breast cancer will actually reduce, despite taking HRT.
Premature ovarian insufficiency
Premature ovarian insufficiency (POI) occurs as a result declining ovarian function in young women under the age of 40 years, which leads to a premature onset of menopause. It is a common and an often under diagnosed condition that can have profound physical and psychological consequences without correct management (European Society of Human Reproduction and Embryology, 2015). POI affects around 1 in 100 women under 40 years in age in the UK (Panay and Kalu, 2009).
In the vast majority of cases of spontaneous POI no underlying cause will be identified. Iatrogenic causes include:
Surgical removal of the ovaries Radiotherapy Chemotherapy Hysterectomy without oophorectomy
This condition should be suspected in any woman who presents with secondary amenorrhoea of more than 3 months’ duration. VMS may be present, but around 25% of women do not have symptoms of the menopause. Women with untreated POI are at increased risk of developing osteoporosis, CVD and dementia (Podfigurna-Stopa et al., 2016). All these conditions increase the risk of early mortality in these women without treatment.
The diagnosis should be made in women age < 40 years based on (NICE, 2015a):
Menopausal symptoms, including no or infrequent periods (taking into account whether the woman has a uterus) and Elevated FSH levels on two blood samples taken 6 weeks apart
The diagnosis of POI should not be made on the basis of a single blood test. If there is doubt about the diagnosis of POI, women should be referred to a specialist with expertise in menopause or reproductive medicine.
Women with POI should be offered either HRT or a combined hormonal contraceptive, unless contra-indicated. Hormone replacement is important for treating symptoms and protecting against the long-term effects of oestrogen deficiency (European Society of Human Reproduction and Embryology, 2015). There is some evidence that HRT has a more favourable impact on quality of life and bone density than the combined oral contraceptive pill (Cartwright et al., 2016)
NICE guidance is really clear regarding the need for women who have POI to receive HRT until the average age of the menopause (NICE, 2015a). Any risks of HRT are not applicable to these young women; any risks with HRT are only relevant to those women over 51 years of age.
Review and referral of women taking HRT
Reiterate importance of breast and cervical screening Review after 3 months to assess response and address any side effects Review annually thereafter Refer the following women to a healthcare professional with expertise in the menopause: ^ Those in whom HRT does not improve their symptoms ^ Those who have troublesome side effects ^ Those who have contra-indications to HRT ^ If there is any uncertainty about the most suitable treatment option
Stopping HRT
There is no maximum length of time for which a woman can take HRT, and arbitrary limits should not be applied. This means that HRT can be continued long term. It is important that women who take HRT are assessed annually to assess their benefits and risks regarding taking HRT. Older women (over 60 years) are advised to start on lower-dose preparations and to try to achieve the minimum effective dose.
If women do want to stop taking HRT, then the dose can be gradually reduced or stopped immediately. However, many women have menopausal symptoms after stopping HRT, and it is important that women are reassured that this is not a withdrawal effect from stopping HRT. These are symptoms that would be present if they had never taken HRT. In these cases, many women may decide to continue their HRT for a longer period of time. Tapering the dose may reduce symptom recurrence initially, but does not influence continuation of symptoms in the long term. There is some evidence that morbidity and mortality can initially increase when HRT is stopped, although it is unclear whether tapering the dose reduces that risk (Mikkola et al., 2015b).
Summary
In summary, the NICE menopause guideline should enable clinicians to feel more confident in offering HRT to eligible women. It will also empower women to make more informed choices regarding their treatment, which can now be based on a more balanced review of the evidence. HRT is generally a safe and effective treatment of menopause-related symptoms. All women should be given the opportunity to discuss the pros and cons of HRT and alternatives as they enter the menopause transition. This will empower them to make informed choices about their health at this midlife point and beyond.
Declaration of conflicting interests
We have both lectured and acted in an advisory capacity for a number of pharma companies.
KEY POINTS
The mean age of women who have a natural menopause in the UK is 51 years, although there is wide variation between women 1% of women experience their menopause before the age of 40 years in the UK The menopause is usually a clinical diagnosis based on symptoms in women aged over 45 years Topical vaginal oestrogen can safely be prescribed long term for women For the majority of women under 60 years in age the benefits of HRT outweigh the risks All women with POI need treatment with HRT unless they have contra-indications