
Abstract
The three core principles of the NHS: that it meets the needs of everyone, that it be free at the point of delivery, that it be based on clinical need not ability to pay, are under threat. Recent policy changes compromise these principles by denying treatment to those in need who cannot pay. This article will give an overview of the policy changes and the impact these have on individuals in vulnerable situations trying to access care, on healthcare staff and our society. Case studies from the Doctors of the World clinic are used to illustrate the effect these changes are having. All names have been changed to protect anonymity.
The GP curriculum and migrant healthcare
The GP curriculum states that as GPs we must ‘actively promote equality of opportunity for patients to access healthcare’, act as ‘advocates for our patients’ and ‘take action to address prejudice and unfair discrimination within systems’. It is also our duty to understand how our patients can access healthcare and be aware of financial restrictions they may face.
Treat others fairly and with respect, acting without discrimination Demonstrate a non-judgmental approach in your dealings with patients, carers, colleagues and others, respecting the rights and personal dignity of others and valuing diversity Recognise and take action to address prejudice, oppression and unfair discrimination in yourself, others and within teams and systems Actively promote equality of opportunity for patients to access healthcare and for individuals to achieve their potential Identify and discuss ethical conflicts in clinical practice and manage the conflicts arising within your roles as a clinician, a patient advocate and a leader in the health service Describe the current structure of your local healthcare system, including the various roles, responsibilities and organisations within it, applying this understanding to improve the quality and safety of the care you provide Identify how local services can be accessed and use this understanding to inform your referral practices Demonstrate an understanding of the financial restrictions within which healthcare operates and identify how the limitations of local healthcare resources might impact upon patient care Optimise your use of limited resources (e.g. through cost-effective prescribing) Identify the opportunities this expanded role provides for reducing inequalities and improving local, national and global healthcare
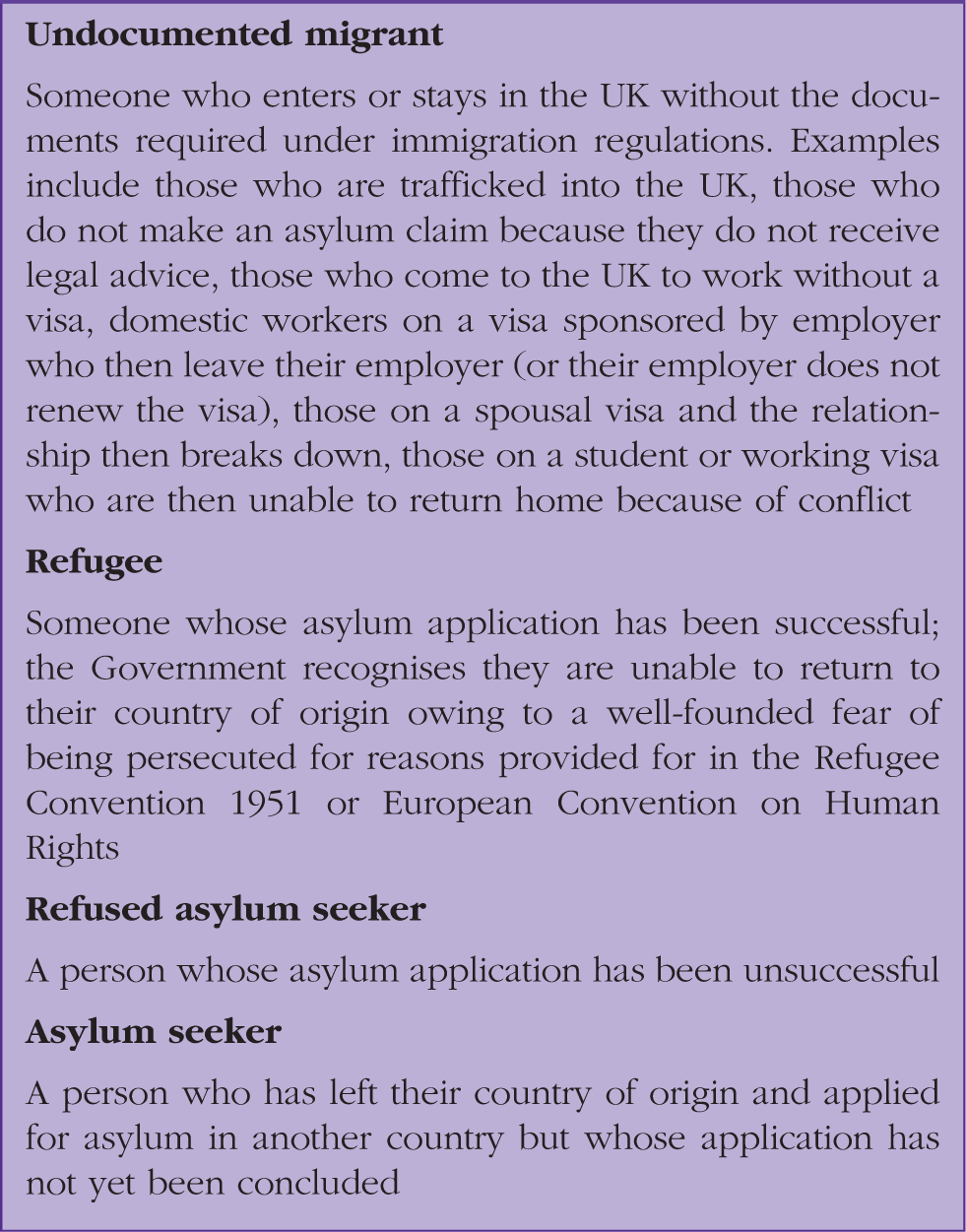
Immigration status definitions.
Entitlement to primary care
NHS England guidance is clear: everyone in England is entitled to free primary care. Lack of proof of address or identification (ID) should not be a reason to refuse patient registration (British Medical Association (BMA), 2016). However, at the Doctors of the World’s (DotW’s) clinic in London, refusal of registration is regularly seen. In 2016, of all the service users seen in the DotW’s clinic, 94% had difficulty in accessing healthcare, and 89% were not registered with a GP (DotW, 2016). Barriers to registration included fearing arrest, refusal by a healthcare team, administrative barriers such as requiring proof of address or ID, and lack of understanding of how the NHS works.
DotW has run a clinic in London for 10 years. Short-term medical care is provided by volunteer GPs and nurses. GP registration advocacy and signposting to housing, immigration advice and community support groups is carried out by volunteer clinic support workers. Service users include migrants in vulnerable situations, sex workers, and those who are homeless. In 2016, 170 volunteers saw 1924 people seeking help to access mainstream NHS services (DotW, 2016). DotW uses this experience in the clinic to challenge health policy and practice that makes it more difficult for vulnerable people to get the healthcare they need. Registering with a GP is a lifeline to many in vulnerable situations. Mariam’s story highlights why.
Case study 1. Mariam.
Mariam, 28 years old, is a refused asylum seeker. She fled Eritrea after escaping from the national military service. The Eritrean government’s use of extrajudicial executions and forced conscription programme - including slave labour, rape of female conscripts and conscription of children - is widely documented (United Nations Human Rights Office of the High Commission, 2015).
After Mariam fled she spent the next few years living as a refugee in Sudan and Libya. She married and had a child. In 2010, her husband disappeared: ‘He went to work and never came back, and we thought he was no-where’. Knowing she was not safe in Libya, she made the dangerous sea crossing to Italy. In Italy, Mariam spent many months sleeping on the streets, experiencing physical abuse and rape. Mariam was then smuggled to France and stayed in ‘the Jungle’ in Calais. By this point in her journey her mental health was deteriorating. She was then smuggled into the UK and picked up by the UK border force. Her claim for asylum was quickly rejected. Her fingerprints had been taken in Italy so, as per the Dublin III Regulation, she was only eligible for asylum there. Mariam had never received immigration advice and relied on hearsay from other asylum seekers: They said they are going to send you back to Italy. I was scared, I don’t want to live the life I was living in Italy, I’d rather live here. So I left the system.
DotW managed to register Mariam with a GP, and she is receiving support from the Red Cross and her church.
Like so many of the patients seen in the DotW’s clinic, Mariam was inappropriately turned away from a GP practice. By denying her primary care, her physical and mental health issues remained unaddressed. Registering Mariam with a GP is one step in helping her access the care she needs. From her experience, she has multiple, complex needs, including risk of sexually transmitted infections, psychological trauma, and risk of infectious diseases such as tuberculosis.
Although she is now receiving care from her GP, any onwards referral, including community mental health services, will now be chargeable, as is outlined in entitlement to secondary care.
Entitlement to secondary care
The 2014 Immigration Act introduced changes to how those ‘not ordinarily resident’ in the UK are charged for NHS healthcare. Charges at 150% of the NHS tariff were introduced, but hospitals were allowed to issue them after the care had been given, allowing clinicians to focus on the patient in front of them. This changed in 2017 with the introduction of upfront charging in hospitals and community health services such as community mental health teams, drug and alcohol teams, district nurses, and non-NHS providers including charities (Department of Health (DoH), 2017). In order to implement this policy on the ground, two processes must take place: first, an assessment of eligibility for NHS care, and second, an assessment of the urgency of care. If a patient who is not eligible cannot pay the full cost of their care upfront and their care is deemed non-urgent, treatment will be refused. The exemption of certain conditions, such as infectious diseases, is of little practical use, as patients would need to be aware of their diagnosis prior to seeking care. In addition, having an unpaid bill of £500 after 2 months carries the threat of being reported to the Home Office, which, for some, could mean arrest (DoH, 2017).
Assessing eligibility is not straightforward. The DoH has not given any clear instructions on how this should be done, and hospitals vary in their methods, often requiring photographic ID, utility bills, previous pay-slips and visas. These documents are rarely readily to hand, and for those in the most vulnerable situations, such as the homeless, those with mental health problems, and undocumented migrants, it presents a significant barrier to accessing healthcare. Ensuring the right assessment is made is difficult, and may have serious consequences if a patient is wrongly refused. No adequate equality impact assessment has been carried out, which is crucial given the likelihood of this resulting in racial profiling and of vulnerable patients being unable to challenge incorrect decisions. Indeed, DotW is regularly notified of exempt patients being charged or urgent treatment being refused if a patient cannot afford it. Without external advocacy for patients in such positions, many individuals are unable to access the care they need.
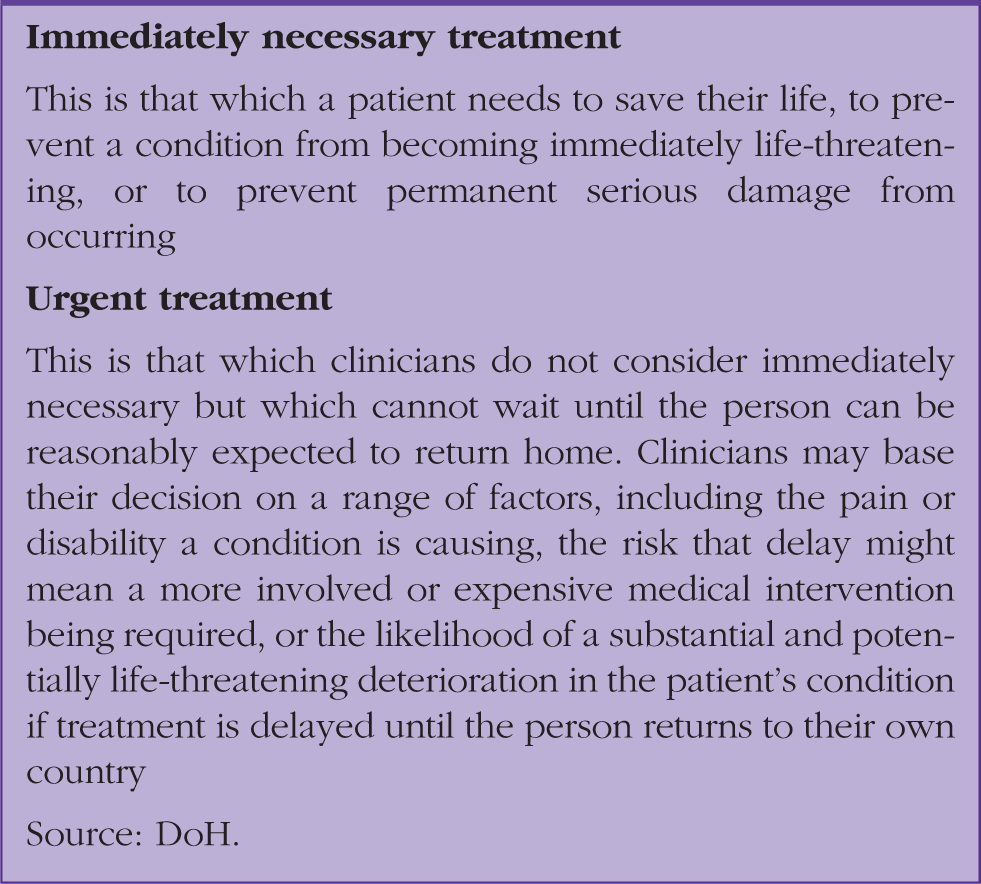
Definitions of immediately necessary and urgent treatment.
These changes bring an unwelcome burden of additional work and complexity to an NHS already under pressure. The full focus of staff on patient care is likely to be impeded as they consider eligibility and whether treatment is urgent or immediately necessary. To make this assessment, clinicians can order some tests, but then an invoice must be presented by hospital administrators based on an estimation of the cost of hospital admission. This puts healthcare professionals in an impossible position: refusing healthcare on financial grounds will be offensive to most NHS clinicians, but their obligations in terms of charging patients have been made clear. Doctors and administrators are not border guards but this immigration policy has a detrimental effect on the doctor–patient relationship.
Restricting healthcare for some impacts the health of all
Restricting healthcare for some impacts the health of all (Hiam et al., 2018). The reasons for this are threefold. First, although migrants carry a very low burden of infectious diseases, lack of routine immunisations and late detection, or under-treatment, could pose a risk to the whole population. Second, limited diagnosis, treatment, and prevention of noncommunicable diseases leads to an increase in late complications that require more costly and lengthy emergency interventions instead of routine preventative care. Overall, this leads to a greater cost to the health service. Third, diverting healthcare teams’ time and resources from patient care to additional administrative processes, decreases patient contact time, and will inevitably lead to longer waiting times and poorer health outcomes.
The argument for implementing these regulations is to ‘recover’ money for the NHS, based on the flawed and largely discredited concept of ‘health tourism’. The government aims to save £500 000 000 annually. No matter how unlikely it is that this objective is achieved, as highlighted by the National Audit Office, the BMA points out that even if the full projection were recovered, this sum would equate to only 0.3% of the NHS budget.
The idea that these measures will result in sufficient revenue to ease pressures on the NHS is not supported by the Government’s own cost assessment (UK Government, 2017a). Scapegoating migrants in vulnerable situations based on anecdotal evidence of ‘health tourism’ overblown by the media is not only unjust, but is also unlikely to make any significant cost savings.
Data sharing
In January 2017, the DoH, Home Office and NHS Digital (which stores NHS patients’ data) published a Memorandum of Understanding (MoU) which allowed the Home Office to access patients’ personal information for the purpose of immigration enforcement (UK Government, 2017b). NHS staff and the public were not consulted on this or, indeed, informed of the practice until a Freedom of Information request triggered the release of the MoU. Home Office officials could request patients’ details (such as addresses) in order to arrest, detain and deport undocumented migrants. According to the DoH, the Home Office made 8127 requests for data in the first 11 months of 2016 alone (The Guardian, 2017).
Following a successful campaign by doctors' groups and charities, including DotW, the government suspended the MOU in May 2018.
There were serious concerns that the practice breached confidentiality, a cornerstone of medical ethics and the doctorpatient relationship. It created another significant deterrent for individuals in vulnerable situations needing to access healthcare. Many healthcare staff felt that implicating the NHS in the ‘hostile environment' regime jeopardised trust in the profession as a whole (Hiam et al., 2018).
Although the government's U-turn is a huge achievement, the data sharing mechanism has not been completely retracted. It still allows Home Office immigration staff to trace people who are being considered for deportation from the UK because they have committed a serious crime.
Impact on those in vulnerable situations
Creating barriers to healthcare disproportionately affects those in the most vulnerable situations; however, to date, no assessment has been carried out of the impact of upfront charges on these groups. Research at the DotW’s clinic found 1 in 3 service users were deterred from seeking timely healthcare due to charging and fear of data sharing (DotW, 2017a). Furthermore, care was displaced from planned routine care to A&E attendances—at a far greater cost to the NHS.
Pregnant women are not exempt from these charges, with devastating consequences. The research published by DotW found 2 out of 3 pregnant women had not had a first appointment by the NICE recommended time of 10/40, and a quarter had not been seen by 18/40. Fear of data sharing and financial debt prevented women accessing the care they need. Unfortunately, this fear is not unfounded, with the cost of an uncomplicated birth billed at £5000–£6500, and with outstanding bills of over £500 at 2 months being reported to the Home Office. It is understandable that women can feel forced to put both their own and their baby’s health at risk. Indeed, two women reported contemplating abortion to avoid the catastrophic costs of pregnancy in the NHS. Josephine’s case outlines some of these fears.
Case study 2. Josephine.
Josephine, 37, is a refused asylum seeker. She fled Uganda because of her sexuality. She was ‘forced into marriage because they found out I was gay which is not allowed in my country’. Her husband had been verbally and physically abusive and when he found out her true sexuality: ‘He came to beat me up’ and told her family. She was forced to run into hiding with a friend leaving her children behind. She reports: I was scared he would have revenge on me because he said I brought disgrace to the whole family. I feared for my safety. I started to beg her, my feet were swollen and I had been walking up and down for 2 days, I hadn’t showered and I hadn’t eaten well. She could see that I was pregnant, and eventually she said that I could come and rest a bit at her house. That’s where I am still staying now. Every time they would chase me away, they told me that as my visa was still valid I wasn’t entitled. They told me I would have to pay something like £300.
Josephine’s application for asylum was denied: I’m waiting for the court date for appeal next month to see if they will grant me asylum. I have to go to the home office every month to report. I don’t want to think about what’s going to happen - I’m just living each day as it comes at the moment.
Impact on GPs
Primary care - including GP and nurse consultations, treatment provided by a GP and other primary care services - remain free of charge, but GPs are left in an impossible position. Primary care workload will undoubtedly increase with community and hospital care denied to those unable to pay. We may be left powerless to help our patients. DotW often sees patients identified as chargeable who are unable to pay and thus left in unbearable situations. Sometimes clinicians are not aware of the DoH exemptions given above, or their care is deemed non-urgent. As a result DotW sees specialist care, including cancer treatment and cardiac surgery, refused. These patients will return to their GP, but without the support of secondary care colleagues, GPs will be unable progress clinical treatment or effectively and efficiently care for patients. The impact of this is highlighted by the case study of Deidre.
Case Study 3. Deidre.
Deidre is from the Caribbean. After she was widowed she came to live in London with her daughter Sally, a UK citizen. In 2016, Deidre was diagnosed with cancer. A specialist advised her that she was too sick to fly home and another clinician later confirmed that the need for chemotherapy was ‘urgent’. Despite this, the hospital demanded a five-figure sum before treatment could commence. As a care worker, Sally is not able to pay for her Mum’s treatment all in one go.
DotW is supporting Sally to challenge the hospital’s decision to refuse the healthcare that Deidre so desperately needs. In the meantime, Deidre remains at home, with her disease poorly controlled, and her GP the only port of call. DotW continues to work on her case.
GP charging in future
Unfortunately, extension of charging into primary care is on the horizon. The Government has made public its intention to implement a phased introduction of charges in primary care, as well as expressing an intention to consult on charging in A&E. Recent additions to the GMS 1 form (a form filled in when registering with a GP) mean that many GP practices have begun to collect data on patients’ chargeability status, laying the foundations for the introduction of charging in primary care (NHS, 2017).
Is your surgery safe? What you can do as a GP
GPs are in a strong position to oppose these changes and advocate for their patients. As an individual, at your practice, and on the national level, it is possible to stand-up for patients in vulnerable situations.
As an individual make sure you know the guidance on entitlements so that you can challenge incorrect decisions. Of course, with complex guidance and a shifting policy landscape it can be difficult for busy clinicians to stay up to date. Consider using the DotW’s UK website and resources or calling DotW if advice is needed. At your practice, make sure your reception staff are aware of patient entitlements, and check your registration policy to ensure people are not turned away incorrectly if they do not have documentation.
In the wake of the revelations around data sharing you can make your surgery a ‘Safe Surgery’ using the DoTW’s toolkit, which provides ways of protecting your patients’ data (DotW, 2017b). The most recent GMS 1 form includes new ‘supplementary questions’ around a patient’s eligibility for charging (NHS, 2017). This aims to identify those who are chargeable as early as possible in the care pathway and to lay groundwork for the future extension of charges into primary care. However, it is important to highlight that although GPs must provide all patients with the form, this section of the form is not compulsory and GPs are under no obligation to ensure it is completed.
Finally, and crucially, be heard. As a GP your voice is powerful and speaking out through Twitter, writing to your MP, and writing to the RCGP and the BMA can have a real impact. As a profession and as advocates for our patients we have both the responsibility and the power to oppose these changes.
KEY POINTS
Primary care remains free to all at present but the government plans to extend charging for some to GPs’ surgeries and A&E NHS treatment in secondary care is no longer free at the point of care for all: failure to pay upfront for healthcare will result in refusal to treat, unless deemed urgent and immediately necessary Consider opposing these changes by supporting the DotW ‘Safe Surgeries’ campaign, and calling on the Government to stop sharing patient information These changes affect those in the most vulnerable situations in our society, including children and pregnant women GPs are in a strong position to oppose these changes and advocate for patients in need