
Abstract
The management of the spondyloarthritis family of diseases has changed significantly over the last 10 years. Improved knowledge of disease pathogenesis, evidence about the effectiveness of early diagnosis, and the routine use of biologic agents, have all improved patient outcomes. This article aims to help GPs recognise spondyloarthritic diseases, improve confidence in primary care management and referral, and provide a summary of the 2017 National Institute for Health and Care Excellence guidance.
The GP curriculum and spondyloarthritis
Know that taking an effective history and making a simple, focused examination in general practice is likely to be more important than imaging and serology, which on their own may be falsely reassuring Know that early diagnosis and treatment of inflammatory arthritis, such as rheumatoid arthritis, has a major impact on long-term outcome. Urgent referral to specialist care is indicated if there is clinical suspicion of inflammatory arthritis Be able to assess the importance and meaning of the following presenting features:
▪ Symptoms which help distinguish inflammatory from non-inflammatory conditions ▪ Systemic manifestations of rheumatic disease ▪ Identify ‘red flags’ that relate to infection (e.g. septic arthritis or osteomyelitis); cancer (e.g. bony metastases and osteogenic sarcoma); fracture (e.g. fragility fracture in osteoporosis); neurological compromise (e.g. cauda equina syndrome); and inflammatory arthritis (e.g. rheumatoid arthritis, ankylosing spondylitis) Know the problems that can be caused by the treatment of musculoskeletal disorders and explain their primary and secondary prevention Be aware of increased cardiovascular risk in patients with inflammatory arthritis, connective tissue diseases and gout
What is spondyloarthritis?
Disease labels in inflammatory disease have changed significantly over the last decade, which often leads to confusion. Spondyloarthritis is the term for the family of diseases that affect not only the joints but also the entheses, the sites where tendons and ligaments join to bone. Inflammation at the enthesis is known as enthesitis, and this is the hallmark pathological finding of the spondyloarthritis family.
Spondyloarthritis can predominantly affect the back and pelvis, which is known as axial spondyloarthritis (Ax-SpA), or can mainly affect peripheral joints (peripheral SpA). People with axial disease can have peripheral symptoms with swollen joints and enthesites, and likewise, people with peripheral SpA can also exhibit signs and symptoms of Ax-SpA.
Spondyloarthritis can often cause inflammation outside of the joints or ligaments, which are known as extra-articular manifestations. The most common of these are anterior uveitis, inflammatory bowel disease and psoriasis.
Is Ax-SpA the same thing as ankylosing spondylitis?
Spondyloarthritis most commonly affects the spine and pelvis; inflammation at the junction between spinal ligaments and vertebrae or within the joints of the pelvis, causes pain and stiffness. The terms ankylosing spondylitis and radiographic axial spondyloarthritis are used interchangeably to describe spondyloarthritis that has caused damage or calcification of the ligaments (ankylosis) that can be seen on an X-ray. If there is no X-ray evidence of change, then this is known as non-radiographic axial spondyloarthritis. As X-ray changes can take 5–10 years to develop, these changes are often not useful in diagnosis or early disease.
What is peripheral SpA?
Peripheral SpA describes the family of diseases that predominantly cause inflammation of the joints and entheses outside of the spinal column. Conditions in this family include psoriatic arthritis, reactive arthritis such as following infection, and enteropathic spondyloarthritis (arthritis which occurs in association with inflammatory bowel disease such as Crohn’s disease or ulcerative colitis). Peripheral SpA can present with joint pain and swelling or tenderness, persistent pain affecting tendon insertions (enthesitis), or swelling of a whole digit (dactylitis).
What is psoriatic arthritis?
Psoriatic arthritis (PsA) is an arthritis associated with skin psoriasis, and is a form of peripheral SpA. Confusingly, patients do not have to have skin psoriasis to be given the diagnosis; 20–30% of patients with PsA will not have currently active skin psoriasis, although they will usually have a personal or family history of psoriasis of the skin or nails.
The major clinical difference between PsA and rheumatoid arthritis (RA) is distribution. PsA is more likely to be asymmetrical, and involve distal interphalangeal joints, large joints, or the spine. PsA is also much more likely to cause inflammation at entheses, or dactylitis, where a whole digit is swollen and tender.
Who is at risk of spondyloarthritis?
Patients of any age and either gender are at risk of developing spondyloarthritis. However, certain groups of patients are at higher risk. These include patients with a personal or family history of:
Psoriasis, or psoriatic nail disease Inflammatory bowel disease Iritis
Patients with a family history of spondyloarthritis are also at increased risk, as are those who have recently suffered bowel or genital tract infections.
Ax-SpA usually starts early in life; it is rare to develop new spinal inflammation after the age of 40 years. Peripheral SpA can develop at any age.
What should make me suspect a spondyloarthritis?
Spondyloarthritis can be difficult to identify, as it can present with a diverse range of symptoms; we know that this can lead to delayed or missed diagnosis. There are some hallmark symptoms and signs that can help differentiate inflammatory pain due to spondyloarthritis from mechanical causes (National Institute for Health and Care Excellence (NICE), 2017):
Pain that is insidious in onset, without a clear injury or trigger Pain that eases with exercise, or worsens with rest Early morning stiffness of the joints or spine that lasts longer than 30 minutes Nocturnal pain Persistent pain affecting tendon or ligament insertions, such as plantar fasciitis, lateral epicondylitis, or Achilles tendonitis Atraumatic joint swelling, or swelling of a whole digit
Remember that certain groups of patients are at increased risk of suffering with a spondyloarthritis; the presence of joint or spinal symptoms in those with established co-morbidities in the SpA family such as psoriasis, inflammatory bowel disease or iritis, or those recently suffering with an infection (especially bowel or genitourinary infections) should raise your index of suspicion.
I suspect spondyloarthritis: What investigations should I request?
The key features of a spondyloarthritis are clinical: a history of inflammatory pain as described above, atraumatic swelling of one or more joints or digits, or persistent musculoskeletal pain in a patient with associated extra-articular co-morbidities such as psoriasis.
Investigations in patients suffering with spondyloarthritis are often not helpful. Inflammatory back or joint disease can often occur despite a normal result in a C-reactive protein test, and X-rays early in disease are frequently normal. You should not therefore exclude spondyloarthritis based on a normal or negative investigation result.
When should I consider referral?
Ax-SpA
NICE referral criterial for suspected axial spondyloarthritis.
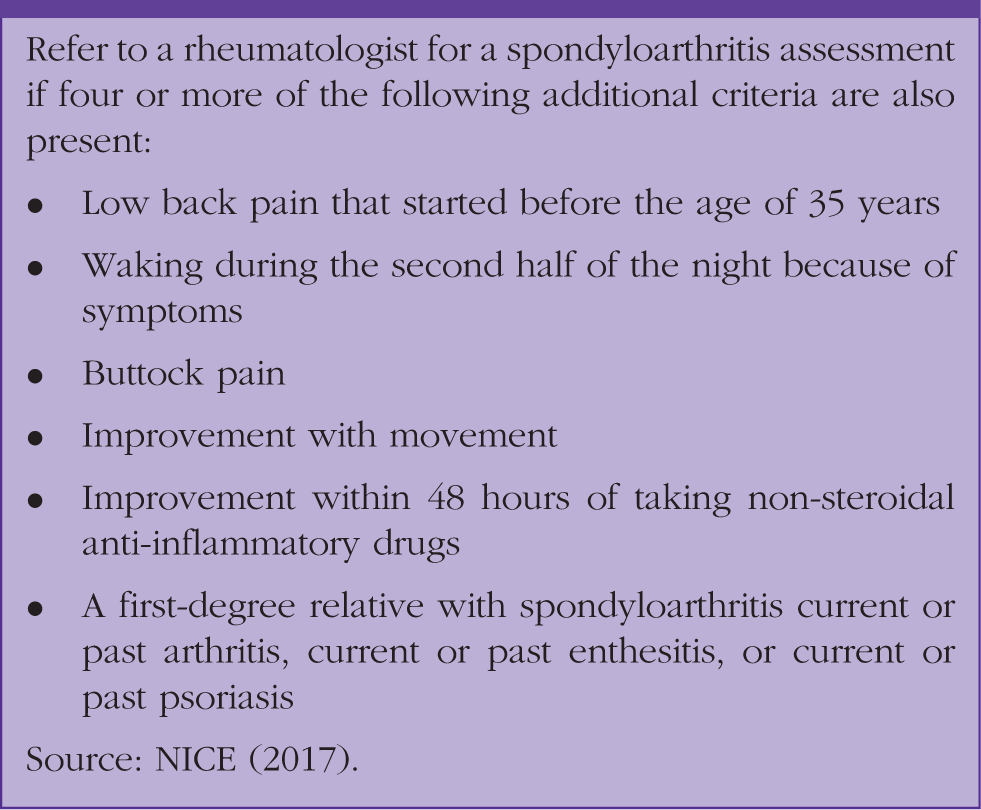
If exactly three of the additional criteria are present, perform an HLA-B27 test, if available. If the test is positive, refer the person to a rheumatologist for a spondyloarthritis assessment (NICE, 2017).
Peripheral SpA
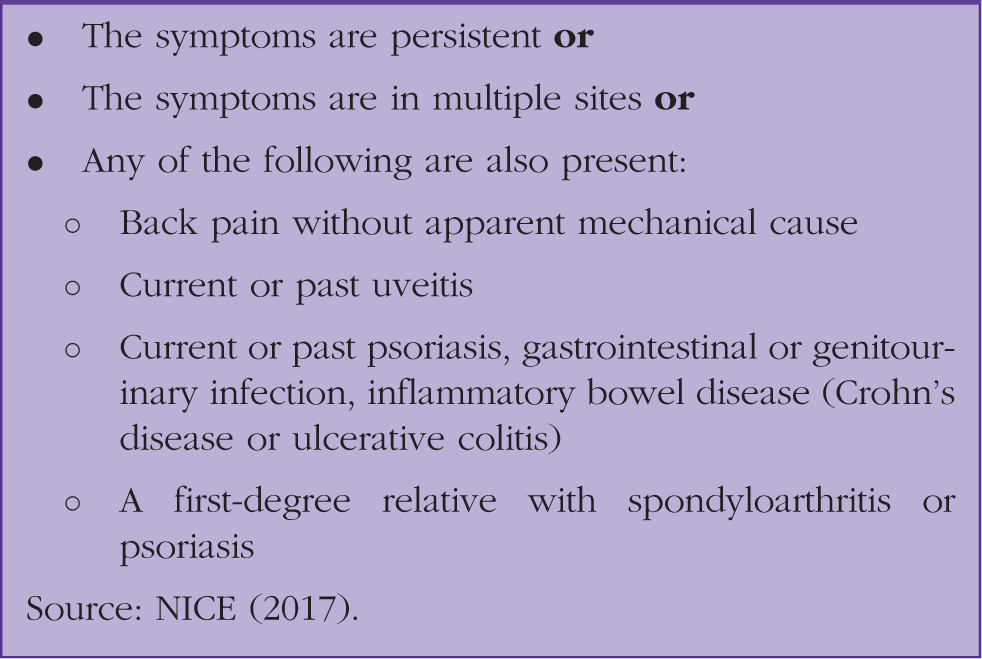
Urgently refer people with suspected new-onset inflammatory arthritis to a rheumatologist for assessment; this should include patients with dactylitis.
NICE referral criterial for suspected peripheral spondyloarthritis.
Primary care management of spondyloarthritis
Shared with secondary care
Management of spondyloarthritis should be shared with colleagues in secondary care. Secondary care colleagues should take the lead in decisions to change or escalate treatment and can offer support from specialist rheumatology allied health professionals such as the specialist nursing team, physiotherapy and occupational therapy.
GPs have a key role in coordinating holistic care in patients with Ax-SpA. Health promotion and recognition of extra-articular co-morbidities, such as depression, are important.
Management of Ax-SpA
Non-steroidal anti-inflammatory drugs (NSAIDs), if tolerated and not contra-indicated are the cornerstone of drug treatment in Ax-SpA. NSAIDs can be effective in reducing the pain and stiffness that affects both the spine and peripheral joints; there is some evidence they may reduce the possibility of spinal ankylosis. It is important to consider co-prescription of a proton pump inhibitor and monitoring of renal function if NSAIDs are used regularly or on a long-term basis. Disease-modifying anti-rheumatic drugs (DMARDs) are not effective in treating spinal pain, or reducing damage in spinal disease. Biologic drugs are proven to be effective in treating symptoms in patients with severe disease.
Management of peripheral SpA
As with Ax-SpA, NSAIDs can be effective in reducing pain from peripheral arthritis and enthesitis. In contrast with axial disease, DMARDs are often very effective in reducing joint pain and swelling. They also reduce the risk of joint damage and deformity. DMARDs should only be prescribed on a shared-care basis with secondary care. As with Ax-SpA, biologic drugs are used to treat severe disease not responsive to DMARDs.
Non-pharmacological management
All patients with axial disease should be referred to a specialised rheumatology physiotherapy service; exercise helps in the maintenance of flexibility and good posture, and also assists with pain management and well-being. Patients with peripheral disease may also benefit from involvement from physiotherapists or occupational therapists.
There is no evidence to support complementary therapy in spondyloarthritis; however, some patients report benefit. Patients with evidence of spinal ankylosis (bony fusion of joints within the spine) should avoid spinal manipulation, due to the potential risk of fracture.
Holistic care should include advice about appropriate weight loss, exercise and smoking cessation. Smoking cessation advice is particularly important; smokers are more likely to have active disease causing joint damage, and biologic drugs in smokers are less likely be effective (Chung et al., 2012; Zhao et al., 2015).
As with all chronic diseases, opportunistic screening for mental health problems is important. Depression and anxiety in spondyloarthritis patients are common; and are associated with increased levels of pain, fatigue and worsened outcomes.
Patient support groups can be invaluable in providing patients with information and advice about their diagnosis. The National Ankylosing Spondylitis Society (NASS, www.nass.co.uk) and the Psoriasis and Psoriatic Arthritis Alliance (PAPAA, ww.paaa.org) can offer information and support to patients.
Flare management
Spondyloarthritis is a relapsing/remitting disease; flares are common, not predictable, and can occur after long periods of well-controlled disease. Although flares can be distressing for patients, symptoms can be managed effectively in primary care. The commonest symptoms of a flare are pain, stiffness and fatigue.
Flares of inflammatory pain
Flares of inflammatory pain can be managed effectively with increased doses of NSAIDs and analgesia. Patients should be encouraged to take an effective dose of NSAIDs and analgesics as soon as a flare begins, and should be given ‘rescue’ courses to keep at home in the event of a flare. Gentle stretches, heat or transcutaneous electrical nerve stimulation machines can help manage pain.
Steroids are of no use in a flare of axial disease. Short courses of corticosteroids may be helpful in treating a flare of peripheral arthritis.
Stiffness
Increased stiffness is a common component of a flare. Patients should be advised that gentle stretching and exercise will not cause soft tissue damage and can help limit symptoms.
Fatigue
Inflammation, pain and poor sleep can all contribute to increased fatigue; patients should be reassured this will settle. Rest, pacing techniques and NSAIDs can all help manage fatigue. Pre-empting flares with a personalised management plan can increase a patient’s confidence in managing flares.
I am keen to improve awareness in my practice: How can I implement change?
How high is the level of awareness about spondyloarthritis within your practice, both colleagues and patients? Could the recent NICE guidelines be discussed at a practice education meeting? Could your practice newsletter include information about the symptoms or signs of spondyloarthritis?
Does your practice have a lead clinician for musculoskeletal disease? A designated lead can help to disseminate information, develop pathways for care, and act as a point of contact with local rheumatologists and physiotherapists.
Identifying patients with spondyloarthritis is difficult. Could your practice develop or use a template for assessment of patients with joint or back pain, which includes a reminder of the referral criteria?
KEY POINTS
The spondyloarthritides are a family of diseases, characterised by inflammation affecting entheses – this is where tendons or ligaments join bones Spondyloarthritis can affect either the spine and pelvis (Ax-SpA), entheseal sites outside of the spine (peripheral SpA), or both Spondyloarthritis is associated with a family of diseases that cause symptoms outside of the joints; the commonest of these are inflammatory bowel disease, uveitis and psoriasis Diagnosis of spondyloarthritis is often delayed; knowledge of key symptoms is important, as investigations are often misleading Flares of spondyloarthritis are common and can be well managed in primary care