
Abstract
The aim of the Clinical Skills Assessment (CSA) is to test a doctor’s ability to gather information, apply learned understanding of disease processes, and offer appropriate person-centred care. Effective integration of these skills is a key element in the exam, and not commonly tested in other disciplines. The CSA is a type of Objective Structured Clinical Examination (OSCE). Most medical OSCEs have stations each relating to one skill set, such as ‘communication’ or ‘physical examination’. Although that may be more relevant in secondary care, where patients arrive already partly sifted, the primary care doctor is faced daily with undifferentiated, often multiple, problems experienced by patients who vary as much as their symptoms. The GP’s task is complex, and best considered as an integration of skill sets. The CSA is an exit exam, testing for evidence of competence of independent practice as a family doctor; hence, we use the entire consultation as our unit of testing. In this article I set out to demystify consulting in the CSA. Throughout, I offer practical tips; these are marked *. I end with a list of suggestions to better prepare candidates for what we all hope will be a good experience.
The GP curriculum and consulting in the clinical skills assessment
Show a commitment to patient-centred medicine Balance the patient’s values and preferences with the best available evidence Demonstrate clear, sensitive and effective communication Manage complexity and uncertainty within the limited time available
Consulting styles
We examiners are often asked what style of consulting is required for the CSA, to which I reply, ‘Any style that achieves the desired result!’ Clinical knowledge is important and enables you to guide the patient in the right direction. However, clinical knowledge alone may be insufficient in all but emergency cases. The ability to understand and respond to the patient’s perspective is also crucial. A case of ‘chest pain’ does not appear in your chair; rather a patient with chest pain consults you. Different patients perceive different issues as problematic, needing varying approaches. Mr A, a young man who has recently started working out in the gym, may happily accept your diagnosis of musculoskeletal chest pain. You may need to adapt your approach, however, when you consult with Mr B, who describes similar symptoms and whose friend died recently from undiagnosed cardiac disease.
Finding out the patient’s ideas, concerns and expectations (ICE) will give you a good start, but to get a good finish, you will need to use that information.
* Aim to weave the ICE into your explanation and/or your suggested management plan(s).
Common misapprehensions about the CSA include:
You need to ‘pass’ every case Blood pressure, pulse, temperature and social history should always be included The role players influence your mark There is always a hidden agenda
Let us take these in turn.
You need to ‘pass’ every case
Clinical Skills Assessment grade descriptors.
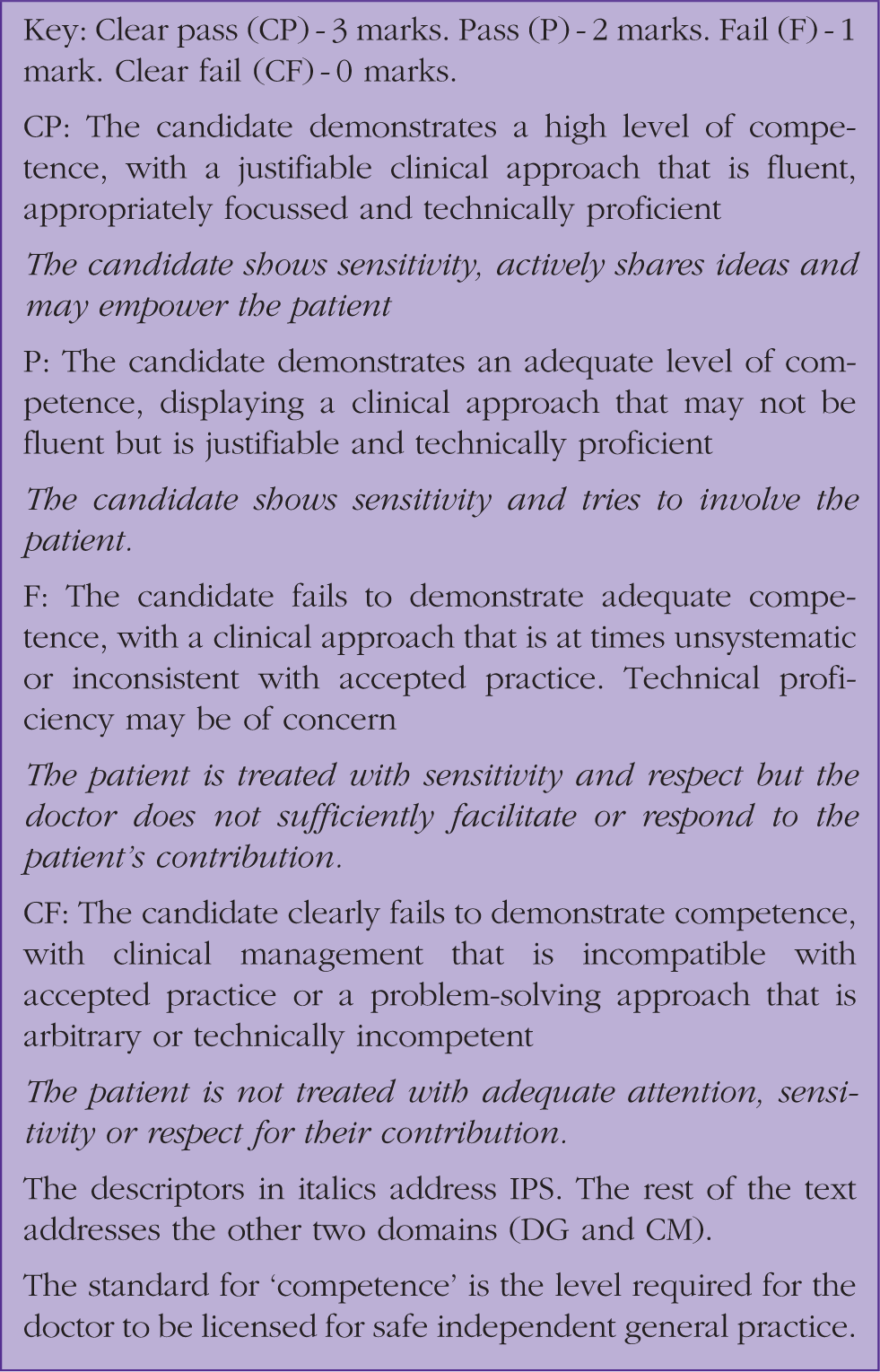
* When you are practising consultations in small groups (as I hope you are), try scoring them in those domains. Read on for details:
Data gathering
DG includes taking a focused history, usually most efficiently started with open questions before narrowing down to specific enquiry relevant to that particular patient. DG also includes your choice of examination, if any, and your interpretation of findings, including test results, if available. High-scoring candidates are typically able to gather the information needed to complete their assessment of the problem within 5–6 minutes.
The biggest shortcoming we see in this domain is a ‘scattergun’ approach, asking a wide range of questions and taking up to 8 minutes. You may lose marks for lack of focus, but more important you will lose them by leaving insufficient time to discuss and negotiate a management plan.
* When nearly ready to sit the CSA, consult with a clock on your desk, or one that is easily visible. How many minutes into the consultation are you stating a working diagnosis, or differential, and moving on to the discussion of management?
Clinical management
CM may include your explanation of the working diagnosis as well as your demonstration of ‘accepted practice’. Higher scores reward a range of feasible options that are justifiable, focused, relevant to, and accepted by, the patient. Have you given the patient significant influence in the plan? Do they agree with it? Do not forget safety-netting and follow-up.
Of the three domains, candidates, whether passing or failing, tend to score lowest on this one. A common pitfall is running short of time, DG having eaten up too many of the 10 minutes. That tends to result in a more doctor-centred approach, with instructions dictated to a passive patient and no time for clarifying/agreeing plans or arranging follow-up.
Another pitfall is simple lack of knowledge of the condition or the guidelines. Cases are written by real GPs and based on real patients, and so deal with common or important conditions.
* The Internet will not be available during your exam, but you will have the British National Formulary (BNF); become familiar with what it contains.
* Keep lists of conditions that you have come across. Working in pairs or groups, swap lists and test each other’s patient-friendly explanations and management strategies.
* Seek out trainees who are different to you. Be aware of your ‘blind spots’ or gaps in experience and discuss strategies for broadening your case load.
NB: Grade descriptors for scores in both DG and CM use the word ‘fluent’. This does not refer to linguistic fluency, but rather to the smooth and efficient flow of the consultation, taking doctor and patient together to a conclusion. This ‘fluency’ can come with practice and attracts a ‘clear pass’ grade (three marks). The description of a ‘pass’ (two marks) is ‘an adequate level of competence, displaying a clinical approach that may not be fluent but is justifiable and technically proficient.’
Interpersonal skills
These include your approach to the patient and your consulting skills. Are you genuinely interested in their predicament? Do you tailor your explanation and/or management to that particular patient? For a ‘pass’ grade, we look for evidence that you have been sensitive to the patient’s position, and at least tried to involve them. Highest scores reward an effective approach, possibly resulting in the empowerment of the patient.
*Be aware of your consulting style and be honest with each other while practising. When under time pressure do you tend to dictate rather than negotiate? Or perhaps you are just too ‘nice’ and agree to all demands? Do you know the Transactional Analysis model of Parent, Adult, Child? Aim for an Adult–Adult conversation with your patient.
Blood pressure, pulse, temperature and social history should always be included
False. To maximise your CSA marks, and to run to time, your DG needs to be focused. If a patient’s condition does not indicate the need for a blood pressure, pulse, temperature, etc, and particularly if that information is already in your notes, then please do not say in the exam that you would like to do it. A detailed social history will be relevant sometimes, but not always. You only have 10 minutes for each case. Choose carefully, as you would do in the GP surgery, what you need to enquire about or examine to enable you to make a working assessment and an appropriate management plan. Focus on that. Ask for relevant information and be prepared to go ahead with any named examination, in the exam setting, in the available time. Your choice, as well as your examination technique, may influence your score in that domain.
The role players influence your mark
False. Role players play no part in the assessment, and do not speak with examiners until the mark has been submitted.
The opening statement is scripted, so every consultation on that case will start identically, whatever circuit, whatever date. After that, it is up to you, and the consultation will progress in the direction that you lead. Most candidates respond to that opening statement with ‘Tell me more’. In the exam, we look for evidence of what you know; so your: ‘Tell me more’ may well lead to the role player replying, ‘OK, what more would you like to know?’ Do not be startled by this into shifting straight to closed questions.
* Practise alternative phrases to keep the data gathering open. What do you want to know?
There is always a hidden agenda
False. Cases are based on real patients. All patients have a viewpoint; some will have preconceived ideas or concerns, whereas others will not. It is the same in the exam. Role players will not intentionally mislead you, but they are instructed to offer certain information only if specifically asked. As with real patients, they are more likely to divulge sensitive information, if it exists, when they are made to feel comfortable. Try to gain their trust. Look interested, be sensitive to their situation and their responses, and then believe them if they tell you (again) that they really are not worried about anything sinister!
Consultation models
Models are frameworks, tools to help us understand the reality of that complex interaction we call the consultation. Your trainer may suggest using various consultation models at different times in your training journey to give insight into what is happening, and to give you a way of measuring your progress as you focus on different aspects of the consultation. Models can also offer techniques for dealing with situations that you find difficult. The RCGP does not support or promote any one particular model, so I suggest that it is worth getting to know several, thus forming a toolkit from which you can select the model most likely to help you with the particular patient in front of you.
* Practise using specific skills or question sets suggested by the various models until they become almost automatic. Then, even under exam stress, they will be there for you, providing that ’fluency’ I mentioned earlier. That will free you up to listen to the patient and concentrate on management plans.
For example:
You may learn from the Pendleton model to enquire into patients’ ideas, concerns and expectations You may use the Calgary–Cambridge system to understand the structure of the consultation as you refine your timings You may use Neighbour’s approach to learn the advantages of summarizing, safety-netting and housekeeping You may refer to Transactional Analysis to understand the power balances in dysfunctional consultations
There are many different models, but the important message is to explore, with guidance from your trainer, the ones that may be useful for your own practice, and try them out. Ultimately the CSA is looking for evidence of a person-centred approach that enhances understanding of a patient's illness and promotes a shared approach to managing problems. There are many ways, with each patient, of reaching that end goal. Any one of them will be rewarded, not only with high CSA marks but with increased concordance and satisfaction levels for you and your patients.
Common reasons for failure, and what to do about them
The most important point here is that success is far more common than failure! Approximately 80% of candidates pass on their first attempt, with a cumulative pass rate of 97% for repeat attenders. The nation needs more competent GPs, and we in the College would be delighted if all candidates were able to demonstrate their readiness for independent practice. That standard is policed by the General Medical Council and determined with patient safety and public accountability in mind.
It is difficult to generalise reasons for failure, but among the most common feedback statements chosen by the examiners from a pre-prepared list for failing candidates are:
Does not develop a management plan reflecting knowledge of current best practice Does not recognise the issues or priorities in the consultation Does not demonstrate an awareness of management of risk or make the patient aware of relative risks of different options Does not develop a shared management plan, demonstrating an ability to work in partnership with the patient
Anecdotally, many examiners also cite, as a reason for poor scores, all-too-frequent examples of candidates who spend so long on DG that they cannot demonstrate shared management. All this boils down to three main principles: know your clinical medicine; tailor your approach to the particular patient in front of you; and work on your time management.
How to maximise your chance of success
My advice is to learn how to consult well, not just how you think you ought to consult for the exam. There is a parallel here with advice on driving tests. Learn to drive well for all road conditions and you are likely to do well in the actual test. If you simply learn for a test, whether the driving test or your CSA, you lower your chances of doing well, as you may come across situations for which you are unprepared.
Study all the resources on the CSA website. It contains a wealth of information. For instance, you will learn there that the ‘palette’, the collection of 13 cases which forms the exam, changes daily. Each ‘palette’ has a pattern; one older patient, one child case, other ages scattered. Cases are roughly equally divided male/female and in social class distribution. You will read of the regular inclusion of cases with a diversity element and that you can expect to perform an examination on at least three cases. Cases broadly sample the curriculum… and more.
Here are some more practical tips:
* Work in pairs or small groups as well as in your practice and in the Training Programme. Use your patients and each other as resources. Try to mix your small learning groups. Find someone different from yourself with whom to study. They are likely to have different life and work experience; thus when you both share your experiences, you will each broaden your awareness of the range of people who may present as your patients.
* Ask for feedback from patients, out-of-hours supervisors and TPDs. Listen to it! Does a pattern emerge?
* Learn to assess your own performance e.g. by using video.
* Agree with your trainer what you need to work on at any given stage in your educational journey: Time management? Focussed, smooth physical examination? Explanations of diagnoses? Management options? Checking patient understanding? Putting all the tasks into a coherent whole?
* Know what resources are in your BNF. Mark your copy with page finders if you want, but do not write in it.
* Wait until your trainer agrees that you are ready to sit the CSA. You should be consulting comfortably at 10 minutes by then. There is very little advantage in sitting the exam at too early a stage in your training.
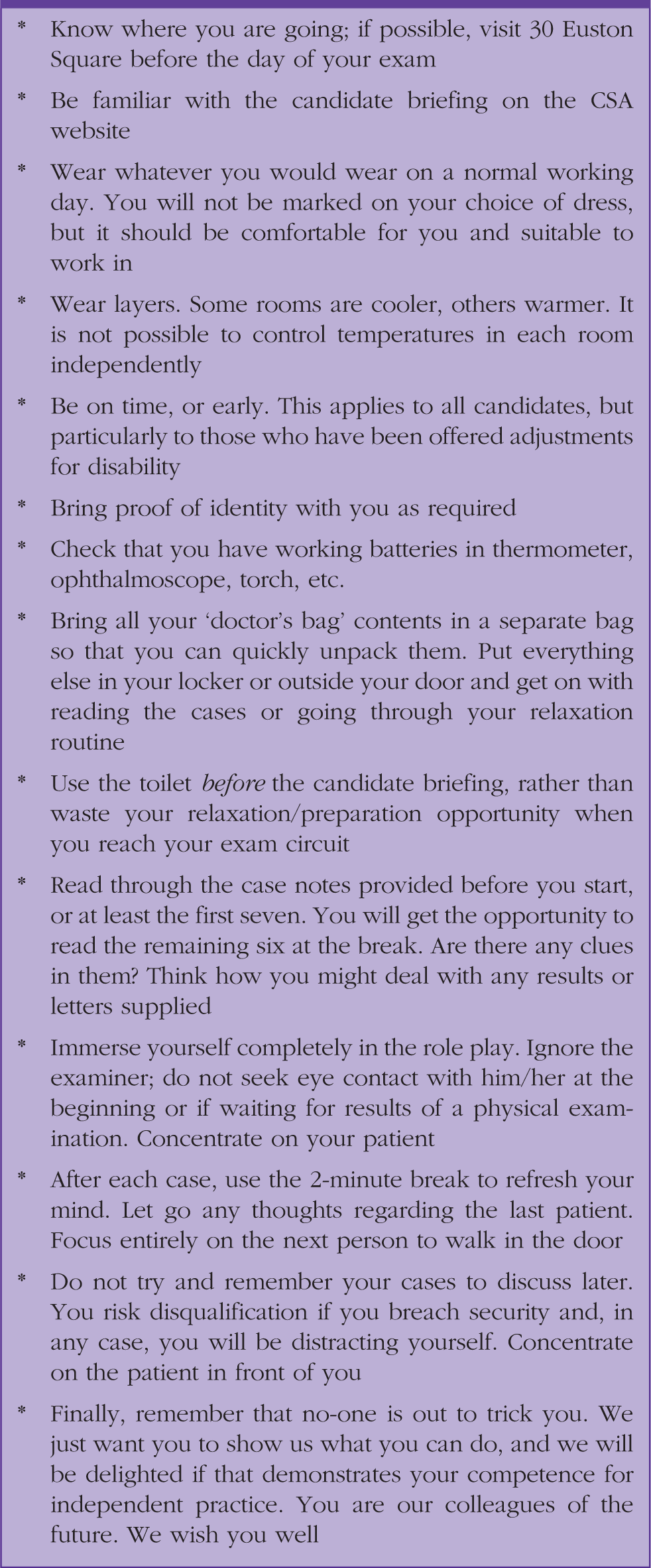
Top tips for the day
Top tips for the day.
KEY POINTS
Familiarise yourself with all the information on the CSA website Learn to consult well in real life; do not try to put on a performance for the exam Keep your DG clinically relevant, but also focused on the patient’s perspective Make sure you leave plenty of time for the ‘management’ part of each consultation Practise in small groups of your peers and give each other honest feedback based on the CSA’s marking domains Trust that the examiners, the role players and the College are not out to trick you