
Abstract
Gynaecological problems in primary care are common. Some gynaecological conditions present as emergencies, requiring rapid referral to secondary care for review and treatment. GPs are likely to see such patients more often in out-of-hours sessions. This article will consider common gynaecological emergencies including pelvic inflammatory disease, bleeding and pain in early pregnancy, vulval abscess, Bartholin’s cyst abscess and ovarian cyst accidents. The article aims to guide assessment of patients in primary care including information on aetiology, risk factors, clinical features, initial investigations, management and referral.
The GP curriculum and gynaecology emergencies
Recognise the signs of illnesses and conditions that require urgent intervention Prioritise problems and establish a differential diagnosis Make the patient’s safety a priority Act calmly in emergency situations and follow agreed protocols Determine whether urgent action is necessary for patients who are acutely ill to ensure correct and timely treatment and to ensure that patients with similar symptoms for whom urgent treatment is not needed are protected from the potential harm of unnecessary investigations and/or therapeutic interventions Recognise and intervene immediately when patients present with a gynaecological or obstetric emergency Be familiar with and implement the key national guidelines that influence healthcare provision for women’s problems
Pelvic inflammatory disease
Pelvic inflammatory disease (PID) is caused by ascending infection from the endocervix that results in inflammation of the cervix, uterus, uterine tubes, ovaries and peritoneum. Progression from initial cervicitis to endometritis, salpingitis, oophoritis and pelvic peritonitis can follow. If the PID is severe, it can lead to formation of a pelvic abscess.
There are an estimated 50 000–75 000 cases of PID in England each year, with a third of cases in women aged between 16 and 24 years (Price et al., 2016).
Chlamydia and gonorrhoea are the most common causative organisms, but commensal bacteria that colonise the vagina, such as Gardnerella vaginalis, can also cause PID (British Association of Sexual Health and HIV (BASHH), 2018). Due to the nature of symptoms occurring with PID, many patients will be directed by the NHS 111 service to genitourinary medicine, or will self-refer to genitourinary medicine drop-in clinics. However, patients with complications of PID will often present to out-of-hours GP services and be referred to gynaecologists.
History
Differential diagnosis of lower abdominal pain in women.

A sexual health risk assessment should be undertaken as part of the history, identifying whether the patient has had unprotected sexual intercourse and/or intercourse with multiple partners. Contact screening should be done if appropriate, although this is generally undertaken by the genitourinary medicine clinic to which these patients are usually referred.
Examination
Examination should include abdominal and pelvic examination (Cuscoe speculum and bimanual examination). Abdominal examination will elicit signs of severe PID, with pelvic peritonitis or abscess. These include guarding, rebound tenderness and percussion tenderness. A Cusoce speculum allows the appearance of the cervix to be assessed. The red indurated ‘strawberry cervix’ associated with Chlamydia trachomatis may be seen. The presence of discharge can be assessed and swabs taken in line with local guidelines. Bimanual examination will identify pelvic tenderness and cervical excitation, which is an important sign of pelvic peritonitis and is the equivalent of guarding/rebound tenderness on abdominal examination. If a patient has true cervical excitation, even slight pressure on the cervix will cause significant distress.
Investigations
Primary care investigations should include high vaginal swabs with both charcoal swabs for microscopy, culture and sensitivity, and swabs using nucleic acid amplification testing for chlamydia and gonorrhoea. Many units have abandoned the use of ‘triple swabs’ including endocervical swabs as tests on high vaginal swabs have similar sensitivity. A urine pregnancy test is mandatory.
Onward referral
Indications for immediate referral to secondary care are signs of sepsis, including the patient’s temperature being raised to more than 38℃, tachycardia, tachypnoea or hypotension. If the patient’s abdomen shows signs of peritonism or if a tubo-ovarian abscess is suspected immediate emergency gynaecology referral is indicated.
Treatment of PID in patients not requiring onward referral can be commenced prior to receiving swab results. A negative swab result does not exclude a diagnosis of PID and treatment should be commenced on the basis of symptoms and clinical suspicion.
The recommended treatment of PID is intramuscular ceftriaxone 500 mg single dose with oral doxycycline 100 mg twice daily and oral metronidazole 400 mg twice daily for 14 days, or alternatively ofloxacin twice daily and oral metronidazole 400 mg twice daily for 14 days. Ofloxacin is not recommended to be used in cases where gonorrhoea is suspected, due to increased resistance in the UK. Other regimes are available in the BASHH guidelines (BASHH, 2018).
Follow up after 72 hours is recommended for patients with moderate PID who have not required admission to secondary care. Failure to improve may need further investigation, different antibiotics or referral for surgical assessment. In many cases, these patients will be under the care of a genitourinary medicine clinic, but if they have been managed in primary care, advice and possible onward referral to secondary care is advisable at this point.
Bleeding in early pregnancy
Bleeding in early pregnancy is common; however, a significant proportion of patients with threatened miscarriage will have a viable pregnancy. Often no cause for bleeding is found, but it is important that miscarriage or ectopic pregnancy is ruled out for affected patients.
Spontaneous miscarriage occurring at less than 12 weeks’ gestation affects at least one in every five women who have a positive pregnancy test (biochemical confirmation of pregnancy) (Royal College of Obstetricians and Gynaecologists (RCOG), 2016a).
Symptoms of miscarriage can include painless vaginal bleeding or bleeding associated with crampy lower abdominal pain, which can sometimes be severe.
When reviewing a patient with a threatened miscarriage (any vaginal bleeding in early pregnancy) gestation should be calculated from the patients last menstrual period unless they have already had an early pregnancy ultrasound dating scan between 11 weeks +0 days and 13 weeks +6 days and the estimated date of delivery has therefore been reliably calculated from the fetal measurements.
History
History includes assessment of bleeding. This can be very difficult to assess objectively, as what patients and doctors perceive as heavy bleeding is very subjective. The soaking of a large sanitary pad with blood over an hour is indicative of heavy bleeding. However, if there is any concern about the extent of the bleeding or if it is difficult to assess, the patient should be referred to a gynaecologist urgently. Likewise, if there is any evidence of haemodynamic instability; including raised pulse (>100 beats per minute) and hypotension, urgent referral is mandatory and may require a blue light ambulance.
Examination
Abdominal examination, palpating for areas of tenderness, masses and peritonism should be undertaken. In patients with miscarriage there may be general tenderness, but not usually signs of peritonism. If speculum examination can be undertaken in a primary care setting (correct bed, lighting and chaperone available) this should be performed to assess primarily for active bleeding. Any products of conception within the cervix and the vagina should be removed as this is likely to help stop the bleeding. Many GPs have reservations about doing this as they have not had relevant experience during their training. GPs with sufficient experience, skill and appropriate equipment (Fig. 1) may carry out this procedure, as it can help to stop bleeding and stabilise the patient before transfer to secondary care. Any products of conception removed should be placed in a specimen pot and kept for histological assessment and/or sensitive disposal; they must not be disposed of in clinical waste. During the speculum examination, vaginal swabs should be taken to screen for infection.
Cusco’s bivalve speculum and Rampley’s sponge holding forceps, required for visualisation and removal of products of conception from the vagina and cervix.
Investigations and onward referral
A urinary pregnancy test should always be carried out so pregnancy can be confirmed if facilities are available for this procedure. Patients with a negative urinary pregnancy test and heavy menstrual bleeding or dysfunctional uterine bleeding can be managed conservatively, although it is reasonable to discuss their management with the on-call gynaecologist.
Criteria for referral to secondary care for bleeding and pain in early pregnancy.
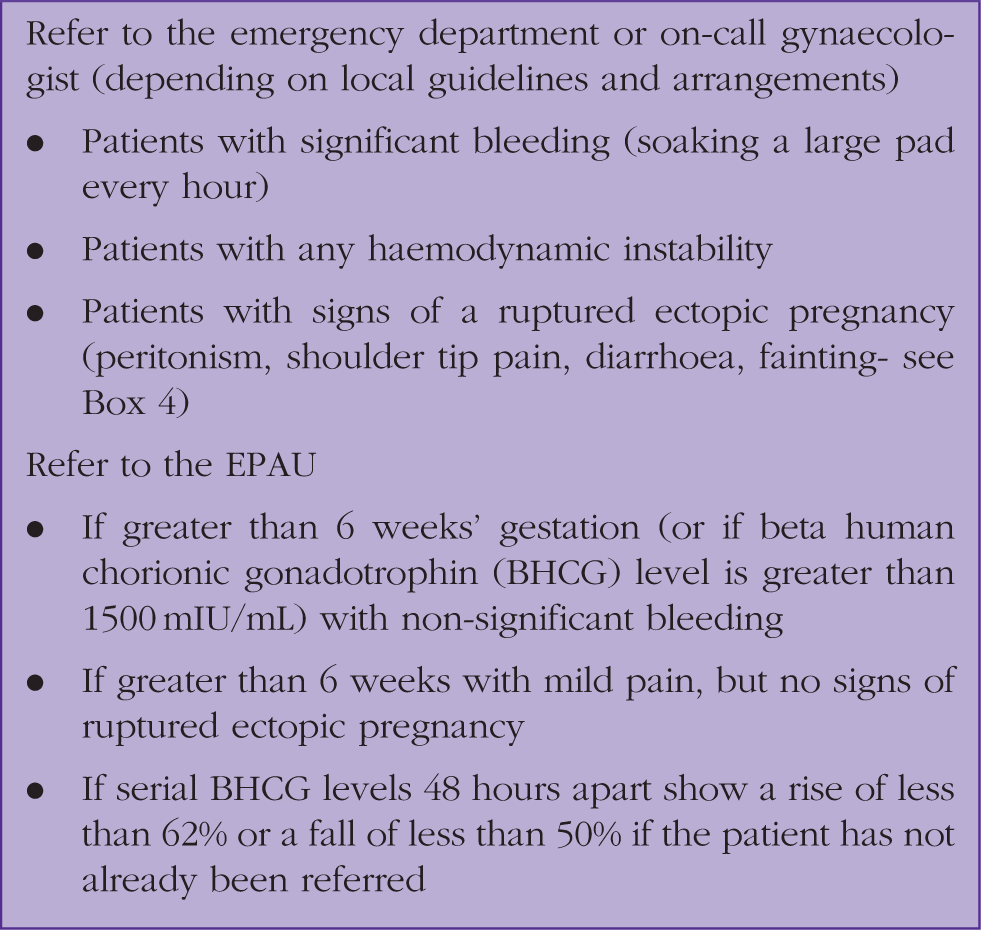
If the patient is under 6 weeks’ gestation and the bleeding is not significant, she should be advised to check a repeat urinary pregnancy test in 7 to 10 days and to return if it is positive (NICE, 2012) to exclude an ectopic pregnancy. A negative pregnancy test will mean that the pregnancy has miscarried. Advice should be given about support systems available and counselling. Written information is helpful. All patients under 6 weeks’ gestation should be advised to return if their symptoms worsen of if they develop pain. If they have pain of any significance they should be referred to an EPAU.
A serum beta human chorionic gonadotrophin (BHCG) level can be assessed in primary care, but many EPAUs will prefer to manage this process, as they are able to provide follow up 7 days a week, with access to ultrasound and expert gynaecological input. Interpreting serial BHCG levels in the context of miscarriage or pregnancy of unknown location is a specialist skill and usually requires the input of an EPAU, or a gynaecologist.
Interpretation of BHCG levels in early pregnancy.

Pain in early pregnancy
Pain in early pregnancy is also a common symptom. An ectopic pregnancy must be ruled out in any patient with abdominal pain and a positive pregnancy test.
An ectopic pregnancy is a pregnancy located anywhere outside the uterine cavity. The overwhelming majority occur in the uterine tubes. They occur in 11 per 1000 pregnancies with a maternal mortality of 0.2 per 1000 cases (NICE, 2012). Risk factors include previous ectopic pregnancy, previous PID and intrauterine device/system. However, one-third of women with ectopic pregnancy have no risk factors.
History
Symptoms and signs of ruptured ectopic pregnancy.

Examination
An examination should include measurement of observations and abdominal palpation. This will elicit tenderness and signs of peritonism, including guarding and rebound tenderness. A speculum examination may be warranted if there is bleeding, as the patient may be having a miscarriage. However, this may not be required, as the pregnant patient with abdominal pain will require an urgent review in secondary care where this can be undertaken.
Onward referral
Women who are stable (mild pain only with no evidence of haemodynamic instability) with a suspected ectopic pregnancy should be referred to the nearest EPAU for an urgent ultrasound scan. Usually this will be done the following working day.
If there is severe abdominal pain, any signs of peritonism or haemodynamic instability or a history of collapse then the patient should be referred immediately to either the Emergency Department or the gynaecologist on call, depending on your local guidance, for resuscitation and assessment. A blue light ambulance may be required to transfer the patient.
In the secondary care setting, the patient will be assessed by a gynaecologist. The diagnosis will usually be confirmed by ultrasound scan and BHCG levels. Ruptured or symptomatic ectopic pregnancy is usually managed surgically with laparoscopic salpingectomy. Stable ectopic pregnancies, with minimal symptoms and low BHCG levels, may be managed medically with methotrexate or conservatively with follow up BHCG levels and, where indicated, further ultrasound scans. Patients are usually followed up until the ectopic pregnancy has either resolved spontaneously or else medical or surgical management has become necessary if not initially required.
Bartholin’s cyst abscess and vulval abscess
The Bartholin glands, also known as the greater vestibular glands, are located in the vagina with openings into the posterior part of the labia majora at four and eight o’clock positions at the vaginal introitus. Their function is to produce mucus which provides lubrication for the vulva and vagina during sexual intercourse.
The Bartholin glands are susceptible to infection and abscess formation (Fig. 2). An abscess is usually a complication of a Bartholin’s cyst, the latter being a small fluid collection at the site of the gland, caused usually by an obstruction to the duct. Bartholin’s cysts are typically asymptomatic and may be felt as a hard pea-sized lump at the vaginal introitus in the anatomical position of the Bartholin’s gland. They often resolve spontaneously.
A left-sided Bartholin’s cyst abscess.
Development of a Bartholin’s cyst is very common, affecting up to one in fifty women. Cyst abscesses are more common in sexually active women between 20 and 30 years in age and women with diabetes mellitus, but can occur in any age; in most cases the cause is unknown.
If a Bartholin’s cyst becomes infected the cyst abscess occurs. Causative organisms are not usually clearly defined; cultures from Bartholin’s cyst abscess tend to be polymicrobial.
History
Symptoms include pain, dyspareunia and discomfort in mobilising. Bartholin’s cyst abscesses can vary in size between that of a small bead and that of a large plum. A Bartholin’s cyst abscess is exquisitely painful and affected patients will present as an emergency to their GP.
Examination
Vulval abscesses usually occur following an infected skin pore or hair follicle. They can occur anywhere on the vulva and can be present at sites including the mons pubis, labia majora and minora.
If a patient presents with a Bartholin’s cyst abscess or a vulval abscess then observations should be measured to rule out pyrexia and tachycardia; which may indicate sepsis. An examination of the abscess is undertaken to review size, swelling, cellulitis and discharge. If any discharge is present swabs should be taken for microbiology, culture and sensitivity.
Treatment and onward referral
Treatment and referral depends on whether the abscess requires incision and drainage. If the cyst is small and the patient has few symptoms or it has already ruptured and is discharging pus, expectant treatment supported by administration of antibiotics is reasonable. Choice of antibiotic is made in accordance with local guidelines and is usually oral flucloxacillin or clindamycin if allergic to penicillin. If a patient is being managed conservatively, they should be reviewed by their GP after a week to check for improvement. If the patient is very uncomfortable and there has been no improvement with oral antibiotics, the patient should be referred to the on-call gynaecologist for surgical assessment.
If at the first consultation the Bartholin’s cyst abscess or vulval abscess is large, significantly indurated and firm then it will be necessary to refer immediately to the gynaecologist on call. Surgical management consists of incision, drainage of the abscess and also marsupialisation for the Bartholin’s cyst abscess. Marsupilisation involves stitching the cyst wall open to allow drainage and prevent recurrence. This is usually undertaken on the emergency theatre list, but is rarely done out of hours, as affected patients tend to be stable. Rarely, systemic infection requiring intravenous antibiotics can occur.
A newer way of managing Bartholin’s cyst abscess, available in many units, involves incision of the cyst abscess under local anaesthetic and insertion of a small catheter device (Word balloon catheter®, Cook Medical, USA) with a balloon that is inflated inside the abscess cavity (Haider et al., 2007). This allows drainage of pus and for the gland to heal while maintaining the opening required for its function.
After treatment, the recurrence rate of Bartholin’s cyst abscess is up to 20% over 4 years. No routine gynaecological follow up is required unless the patient has been affected by recurrent Bartholin’s cyst abscesses (three or more). If this is the case, the patient should be tested for diabetes mellitus and referred for consideration of excision of the affected Bartholin’s gland.
Ovarian cyst accident
Ovarian cysts (fluid filled structures on the ovary) are very common. Up to 10% of women will have surgery for an ovarian mass over their lifetime (RCOG, 2016b). Ovarian cysts usually arise as a result of the physiological functions of the ovary following follicular development and maturation during the first part of the menstrual cycle. An ovarian cyst is 4 cm or greater in size, cysts smaller than this usually represent an ovarian follicle or a corpus luteum and a normal finding in women of reproductive age.
An ovarian cyst accident includes a torsion, rupture or hemorrhage of the ovarian cyst.
In ovarian cyst torsion, the cyst usually has to be larger than 7 cm in size for torsion to occur. They are particularly likely to occur in the postnatal period, as the uterus involutes following a pregnancy, or when the ovaries are swollen with multiple follicles following assisted reproductive techniques (ovarian hyperstimulation syndrome). The cyst and the ovarian pedicle (which includes the blood supply) are twisted. This disrupts the blood supply to the ovary and causes sudden onset severe pain. Usually, there will be signs of peritonism and there may be an acute abdomen with guarding and rebound tenderness. The pain may resolve as the cyst de-torts but can recur. A palpable mass may be present on abdominal and/or bimanual examination Blood tests usually show mildly raised inflammatory markers. An ovarian cyst causing tenderness will be present on ultrasound. Cyst torsion is a surgical emergency and de-torting the cyst via laparoscopy or laparotomy is necessary to restore the blood supply to the affected ovary and to remove or drain the cyst.
When an ovarian cyst ruptures, fluid is released from the cyst into the peritoneal cavity presenting clinically with sudden onset severe abdominal pain. The patient may have signs of an acute abdomen, caused by peritoneal irritation due to the cyst fluid. Blood tests are usually normal. Ultrasound scan typically shows an ovarian cyst and the presence of free fluid in the pelvis. Cyst rupture is usually managed conservatively in secondary care, with analgesia and fluids. Symptoms resolve spontaneously and elective surgery to remove the cyst at a later date may then be required.
Ovarian cyst haemorrhage is when spontaneous bleeding from an ovarian cyst occurs. It can be associated with cyst rupture. Cyst haemorrhage may also occur from a corpus luteum bleeding during the second half of a normal menstrual cycle. Cyst haemorrhage presents very similarly to ovarian cyst torsion and cyst rupture. Blood tests may reveal a lower haemoglobin level on the blood tests and a haemorrhagic ovarian cyst with signs of bleeding may be identified on the ultrasound scan. The bleeding usually stops spontaneously and unless there is haemodynamic instability or a significant bleed, surgical intervention is not usually required. If surgery is undertaken this is usually done laparoscopically.
History
Ovarian cyst accident should be considered in patients presenting with sudden onset lower abdominal pain. History should include the site, onset, character, radiation and associated symptoms of the pain. Vaginal bleeding should be enquired about. Lower urinary tract and gastrointestinal symptoms should be assessed. Differential diagnoses include appendicitis, diverticulitis, gastroenteritis, renal colic, pyelonephritis, adhesions, endometriosis and pelvic inflammatory disease (see Box 1).
Assessment and onward referral
Observations must be assessed to check for haemodynamic stability. A urine dipstick must be taken and a pregnancy test checked to ensure that the patient does not have an ectopic pregnancy. If the pregnancy test is positive, the patient should be treated as having a suspected ruptured ectopic pregnancy until proved otherwise. Abdominal examination will elicit signs of peritonism or the presence of a mass. Ideally a bimanual examination should be undertaken to palpate for adnexal masses or tenderness.
If the patient is in pain requiring parenteral analgesia, is very tender on examination or has a mass or signs of peritonism an urgent referral to the Emergency Department should be made. If the patient is known to have an ovarian cyst, direct referral to the on-call gynaecologist should be considered.
KEY POINTS
Gynaecological emergencies are common and all GPs need to be familiar with their assessment, management and indications for onward referral All women of potential reproductive age with abdominal pain must have a pregnancy test It is essential to consider all women with abdominal pain and a positive pregnancy test as having an ectopic pregnancy until this is excluded If a patient has significant bleeding in early pregnancy urgent referral to the on-call gynaecologist or the Emergency Department is necessary If a non-pregnant female patient presents with severe abdominal pain, consider the possibility of an ovarian cyst accident