
Abstract
Psychosis is an example of severe mental illness; 80% of first psychotic episodes occur in patients between 16 and 30 years in age. The use of an early intervention in psychosis (EIP) team aims to improve outcomes and provide evidence-based treatment for young patients in the community. GPs are often the first clinicians consulted by patients with early features of psychosis, the symptoms of which are often non-specific. Change in patient behaviour and social isolation may be indicators of psychosis. These patients will need prompt referral to the EIP services. This article will outline the early clinical features of psychosis and the GP’s role in management.
The GP curriculum and early intervention for psychosis
Consider the mental health of a patient in every primary care consultation: 90% of people with mental health problems across the lifespan are managed in primary care Mental health problems contribute to disability, unemployment and social exclusion
What is psychosis?
Psychosis is a mental health disorder that can present with delusions, thought disorder and hallucinations. In England, the incidence of psychosis is 31.7 per 100 000 person-years (Kirkbride et al., 2012). Common causes of psychosis include schizophrenia, schizoaffective disorder, bipolar affective disorder, psychotic depression and drug-induced psychosis. Patients with psychosis have an increased risk of mortality from physical health co-morbidities, with a 15- to 20-year reduced survival compared with those without psychosis (Brown et al., 2010). Psychosis carries a 10% lifetime suicide risk within 5 years of its onset. The risk is highest during the first relapse (Wiersma et al., 1998) and the lifetime prevalence of psychosis is above 3% (Perala et al., 2007), with the condition being three times more common in patients living in inner city areas (Kirkbride et al., 2007). Use of illicit drugs, for example cannabis, increases the risk of developing psychosis (Moore et al., 2007). Eighty percent of new patients with psychosis are between 16 and 30 years in age (Shiers and Lester 2004). The use of an early intervention in psychosis (EIP) team aims to improve outcomes with earlier intervention in the community (Csillag et al., 2017).
Early psychosis and challenges for GP diagnosis
Early symptoms and signs of psychosis, unlike florid psychosis, are non-specific. Patients during this ‘prodromal period’ can present to GPs with symptoms of poor sleep, mood changes or panic. They may be socially withdrawn and isolated. Patients may have poor attendance at school or college. They may have relationship problems. Family members may be concerned with changes in the behaviour of patients including social withdrawal, irritability and paranoia. The ‘prodromal period’ can last from several months to a year prior to the onset of psychosis.
Controversy exists on whether the time between onset of the prodromal period or the time from onset of true psychotic symptoms and treatment should be classified as the duration of untreated psychosis (DUP) (Keshavan et al., 2003). A shortened DUP has been shown to positively impact on the prognosis of psychotic disorders at a year, with improved overall functioning of patients. A shortened DUP is associated with lower levels of depression and anxiety together with reduced positive and negative symptoms (Marshall et al., 2005).
The differential diagnosis of early psychosis includes depression, chronic anxiety, normal stress reaction, autism, and substance misuse. In adolescents, it can be difficult to decide whether social isolation and changes in sleep pattern, for example, are due to early psychosis or part of normal development. It is helpful for GPs to acknowledge family concerns and use clinical judgement when deciding whether changes in behaviour are pathological or not.
Neurological conditions including epilepsy (in particular temporal lobe epilepsy), multiple sclerosis, frontal lobe tumours and head injuries can mimic early psychotic symptoms, as can organic conditions such as thyroid dysfunction, Cushing’s syndrome, systemic lupus erythematosus (SLE) vitamin B12 deficiency and human immunodeficiency virus infection. A variety of other infections may also manifest with psychotic symptoms.
In children and young patients, the prevalence of psychosis is between 0.4% and 0.45%, with the average GP seeing a new case of childhood psychosis every 3 to 5 years (Brugha et al., 2005; National Institute for Health and Care Excellence (NICE), 2014).
GP assessment of the patient
Patients with early psychosis may lack insight into their problem and may not fully understand the concerns raised by their behavioural changes. These patients often feel no need for a GP consultation, and it is common for family members or carers to approach their GP for help. Concerns from relatives or carers are often important in shedding light on the underlying clinical problem. However, it can be a challenging problem to manage when the patient refuses to attend consultations.
A refusal to attend consultations may be the consequence of lack of mental capacity. Assessing the competency of such patients using guidance from the Mental Capacity Act (2005) is not an area with which all GPs are familiar. Patients with a mental disorder may still have capacity to make certain decisions, and it cannot be assumed that patients with possible psychosis lack capacity. GPs will often need assistance in assessment of capacity and should contact the local psychiatric team for advice.
Eliciting the clinical features of early psychosis is not straightforward. It is particularly difficult for GPs, due to the relative rarity of this presentation and the non- specific nature of symptoms and signs. It may be helpful when assessing patients to review patients several times, to offer longer appointments, and to make an extra effort to accommodate appointments, if necessary outside routine surgery appointment times. This flexibility can help trust and build the patient’s confidence while affording the clinician time to better assess the patient.
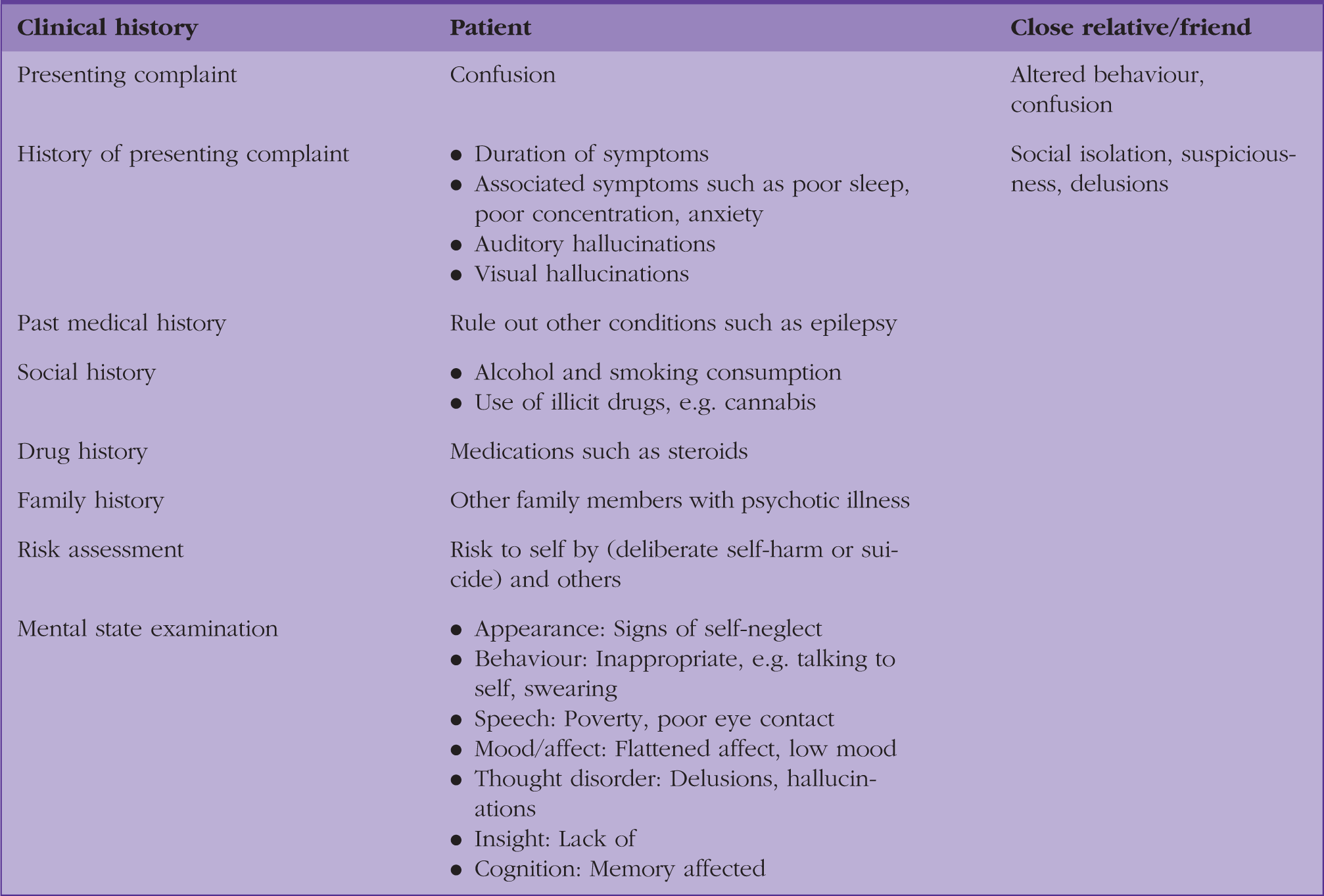
Looking at the clinical history and mental state examination relevant for a patient with early psychosis.
Patients with psychotic features may need to be investigated to exclude physical illnesses causing psychotic symptoms. Such investigation may need to wait until the patient is clinically stable and ready to accept further investigations. Physical illnesses to consider include infection, metabolic disorders, nutritional deficiencies and drug withdrawal. Deciding what is best for the patient depends on the severity of symptoms and the safety of the patient. Investigations can often only be organised by the psychiatry team after the patient’s mental state has been assessed and stabilised.
After assessment of a patient with possible psychosis, it is often appropriate and helpful to discuss findings with colleagues, the community psychiatric team and the consultant psychiatrist. Any plan made for the patient needs to be carefully documented, detailing any advice given from colleagues. Following assessment and discussion a formal referral can be made. In the case of a child or young adult under 18 years in age, informal discussion with the Child and Adolescent Mental Health Service (CAMHS) can be valuable to help access support for the family during what is likely to be a difficult and distressing time.
Referral process for patients with early psychosis
Patients who present with a first episode of possible psychosis should be referred promptly to specialist services, such as the EIP team. If EIP services are not available, referral can be made to the specialist mental health team. NICE (2014) recommends that all patients with a first episode of psychosis should have access to EIP services.
NICE (2016) recommends referral of patients with suspected psychosis presenting for four or more weeks to the EIP services or the CAMHS service (for patients 17 years or under). Diagnostic uncertainty, refusal of treatment by patients with limited insight, and patients with transient or attenuated signs or symptoms of psychosis may all prompt referral. Use of the Mental Health Act in adult patients, and even rarely in children/young adults, may be necessary if patients lack insight into their condition and pose a threat to themselves or others.
GPs can provide valuable support for carers and family, especially during the early phases of care, for example by listening to concerns, offering explanations, signposting and helping with coping strategies.
What is EIP?
EIP is an intervention involving multi-disciplinary professionals to detect and manage psychotic disorders early. The advantages of EIP are multi-fold and include reducing the risk of future relapse, improving patients’ ability to function effectively and managing at-risk patients prior to the development of florid psychotic symptoms. EIP services include specialised outreach teams who have a reduced caseload compared with conventional community mental health services. Multi-disciplinary teams are made up of psychiatrists, community psychiatric nurses, clinical psychologists, social workers and occupational therapists participating in a holistic manner to manage the patient’s symptoms efficiently (Csillag et al., 2016).
Primarily, EIP aims to not only manage young psychotic patients, but also to identify patients who are at risk of developing psychosis. Patients are managed based on the principles of the bio-psycho-social approach using a variety of interventions including anti-psychotic medication, psychological therapies (to help with coping strategies), help with reducing the risk of illicit drug use, and help with financial concerns. Outreach teams help patients and their families to remain in contact with community services. Referrals to the EIP services are encouraged from GPs, other healthcare professionals based in secondary care, schools and even the police (Marshall et al., 2004).
EIP services have been shown to shorten the DUP leading to improved employment (over subsequent 10 years) (Ten Velden Hegelstad et al., 2013), improved social functioning (Dieterich et al., 2010) and improved patient satisfaction (Nordentoft et al., 2014).
Role of GPs in managing the physical health of patients with psychosis
The NICE clinical guideline ‘Psychosis and schizophrenia in adults: treatment and management’ (NICE, 2014), summarises the recommendations for GPs in managing patients with psychosis. GPs have an important role in improving the physical health needs of such patients.
Patients with a severe mental illness die 15 to 20 years earlier than those without a mental illness (Brown et al., 2010). They have a high risk of diabetic and cardiovascular co-morbidity caused by multiple factors. These include genetic factors, deprivation and lifestyle choices. Low exercise levels, heavy smoking, poor diet and anti-psychotic medication all increase the risk of abnormal glucose and lipid metabolism (De Hert et al., 2009). Diabetes, cardiovascular disease, cancer and respiratory diseases are two to three times more prevalent in patients with severe mental illness (Brown et al., 2010). GPs are well placed and able to manage these conditions and address the wider needs of this complex and vulnerable group of patients.
The annual health review is an opportunity to assess physical status. Body mass index, cardiovascular status, nutritional status, physical activity and detection of movement disorders can be combined with blood tests, including fasting blood glucose, glycated haemoglobin (HbA1c), lipid profile and prolactin levels. It is also of value for the QRISK3 score (Hippisley-Cox and Brindle, 2017) and the QDIABETES score (Hippisley-Cox and Coupland, 2017) to be recorded for every patient. Use of cigarettes and blood pressure needs to be recorded annually for patients with psychosis in primary care. It is recommended that secondary care team members (e.g. the care coordinator) are given a copy of these results (NICE, 2014).
There is a risk of weight gain and metabolic changes with anti-psychotic medication (abnormal lipid and glucose metabolism). GPs can support patients to reduce weight and take up more physical activity. Measures to encourage and support patients with smoking cessation are also important.
Conclusions
Psychosis affects young people and can lead to poor health outcomes if not treated in a timely fashion. Detecting early psychosis is a challenging task. Primary care has a vital role in detecting patients with symptoms and signs of early psychosis and referring to specialist services. GPs have an important role in the ongoing care of patients including management of co-morbidities, risk and lifestyle modification.
KEY POINTS
80% of patients with psychosis present between 16 and 30 years of age Psychosis is associated with a high risk of suicide (10% lifetime risk), job loss and premature death (mainly from cardiovascular disease) Early symptoms of psychosis are non-specific and include poor sleep, panic, mood disorders, social withdrawal and thoughts of suspicion or mistrust Early detection of psychosis relies on recognition of early behavioural changes and acting on family concerns Assessment requires screening questions to elicit paranoia, hallucinations, social isolation and suicidal risk Patients with symptoms of early psychosis need referral to specialist services for early intervention
Footnotes
Acknowledgement
The authors would like to thank Dr Alan Cohen for his immense help and encouragement with the writing of this article under the InnovAiT ‘buddy’ scheme.