
Abstract
Rosacea is a common, chronic skin disease that affects the facial pilo-sebaceous glands. It is characterised by erythema, flushing and sometimes papules. It typically affects the convex surfaces of the face, most commonly the forehead, cheeks, chin and nose. Rosacea predominantly affects the Caucasian population, with prevalence being higher in northern Europe than southern Europe. It is three times more common in females and peaks between 30 and 60 years of age. Rosacea can usually be well managed with topical or oral treatments in primary care, although some forms of rosacea or treatment-resistant cases may need specialist input.
The GP curriculum and rosacea
Understand how to recognise common skin conditions in primary care and instigate appropriate management Be aware of primary care resources and when to refer to secondary care, so that the patient receives appropriate treatment
Aetiology
In rosacea, the facial capillaries develop a tendency to dilate easily. Vasodilatation and chronic inflammation is thought to stem from a change in the innate immune response (Schaller at al., 2017). A link between rosacea and bacteria on the skin or in the gut has been suggested by some researchers, but evidence is still inconclusive. Although antibiotics can be effective in treating rosacea, this is probably due to their anti-inflammatory rather than anti-microbial properties. The presence of the common skin mites Demodex folliculorum or Demodex brevis has been long associated with rosacea, however, they are thought to have an aggravating rather than causative effect.
Clinical presentation
Clinical presentation depends on the subtype of the disease, but in most cases, there is a history of episodic flushing of the face which is exacerbated by environmental and lifestyle factors. The subtypes of rosacea are listed in Table 1 with their common features (Wilkin et al., 2002). Papulopustular rosacea (see Fig. 1) is the commonest type, and can usually be managed well in primary care. Symptoms of episodic flushing commonly precede the onset of rosacea, sometimes even by a few years.
Papulopustular rosacea. The four subtypes of rosacea.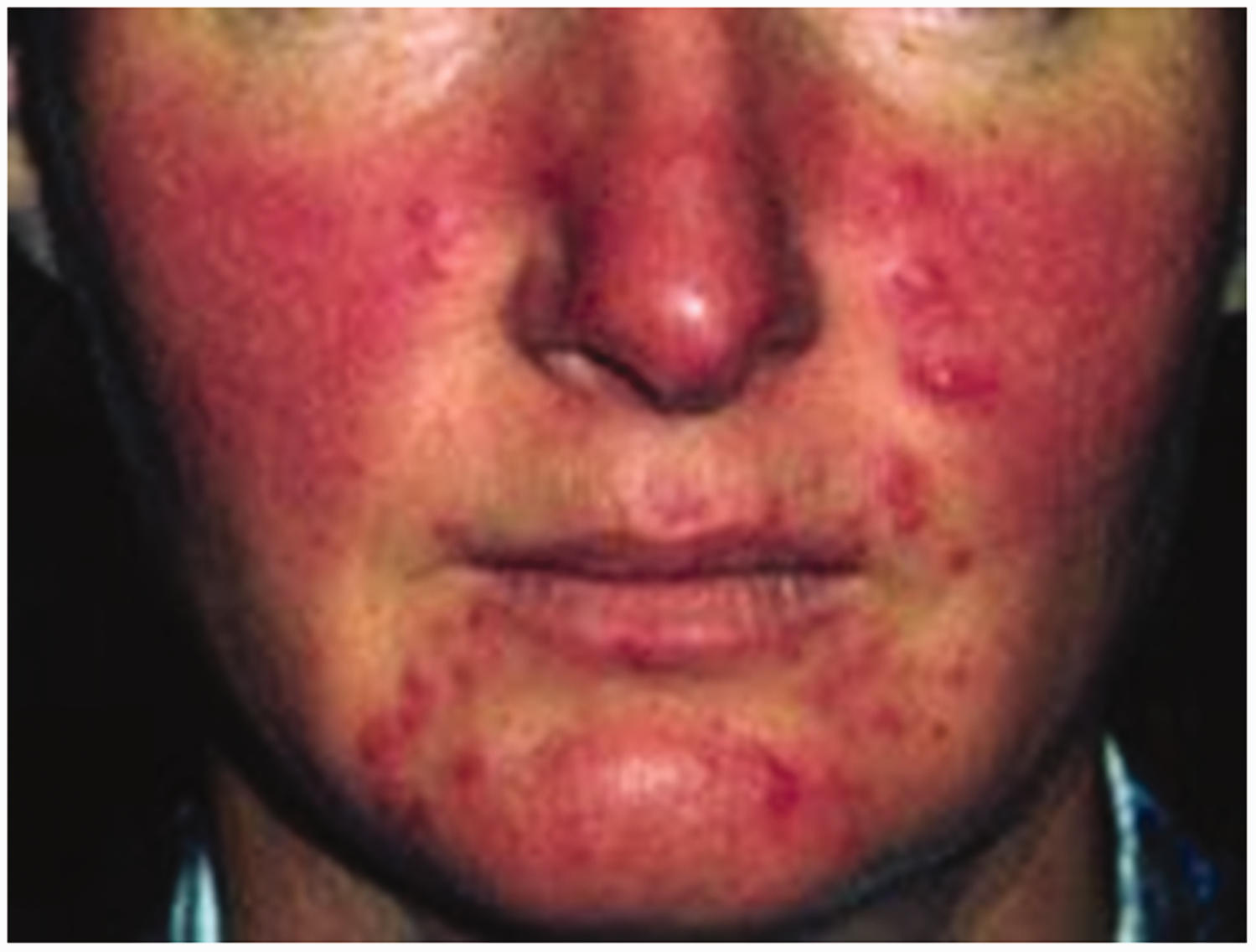

Although it is an acneiform disease, unlike acne, the skin is dry in rosacea. The most common areas involved are the forehead, nose, cheeks and chin, with sparing of peri-oral and peri-orbital skin. Less commonly, other body parts such as the eyes, ears and neck can be affected (Stollery, 2017). Sometimes a sensation like burning and stinging is associated with flushing and oedema. Rarely acne-like comedones can also be seen, which can lead to diagnostic uncertainty.
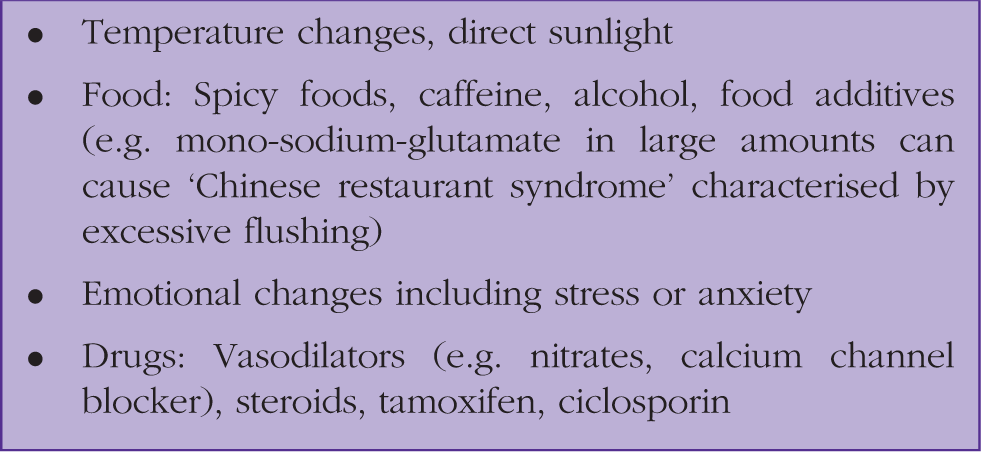
Common causes of flushing.
Like many skin conditions, rosacea often affects self-esteem. A poorly controlled rosacea can lead to low mood and anxiety. It is important in primary care to look at the skin condition in the context of its impact on the patient’s life.
Diagnosis
Rosacea is a clinical diagnosis. There are no fixed criteria or clear definition for rosacea diagnosis. Some suggest that for a diagnosis of rosacea, erythema should be present for at least 3 months.
Differential diagnosis (see also Box 1 for causes of flushing).

Management
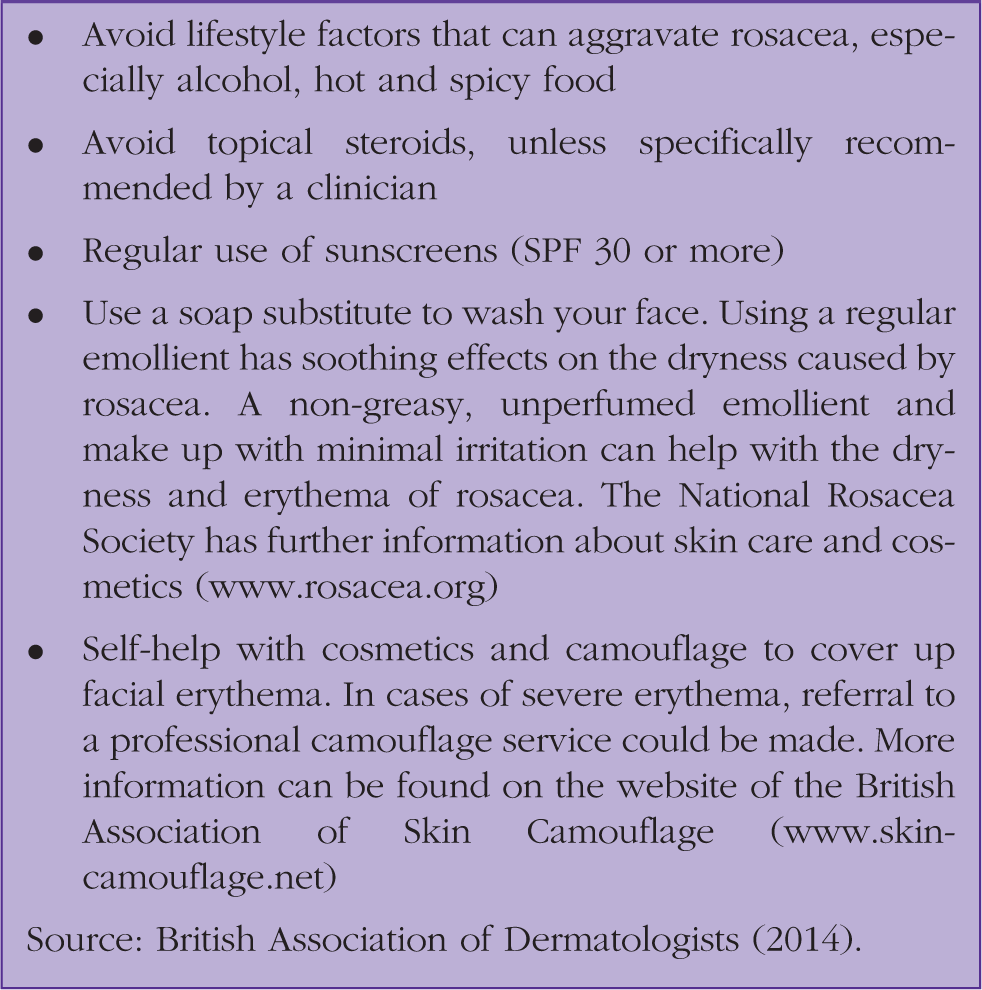
Self-care advice.
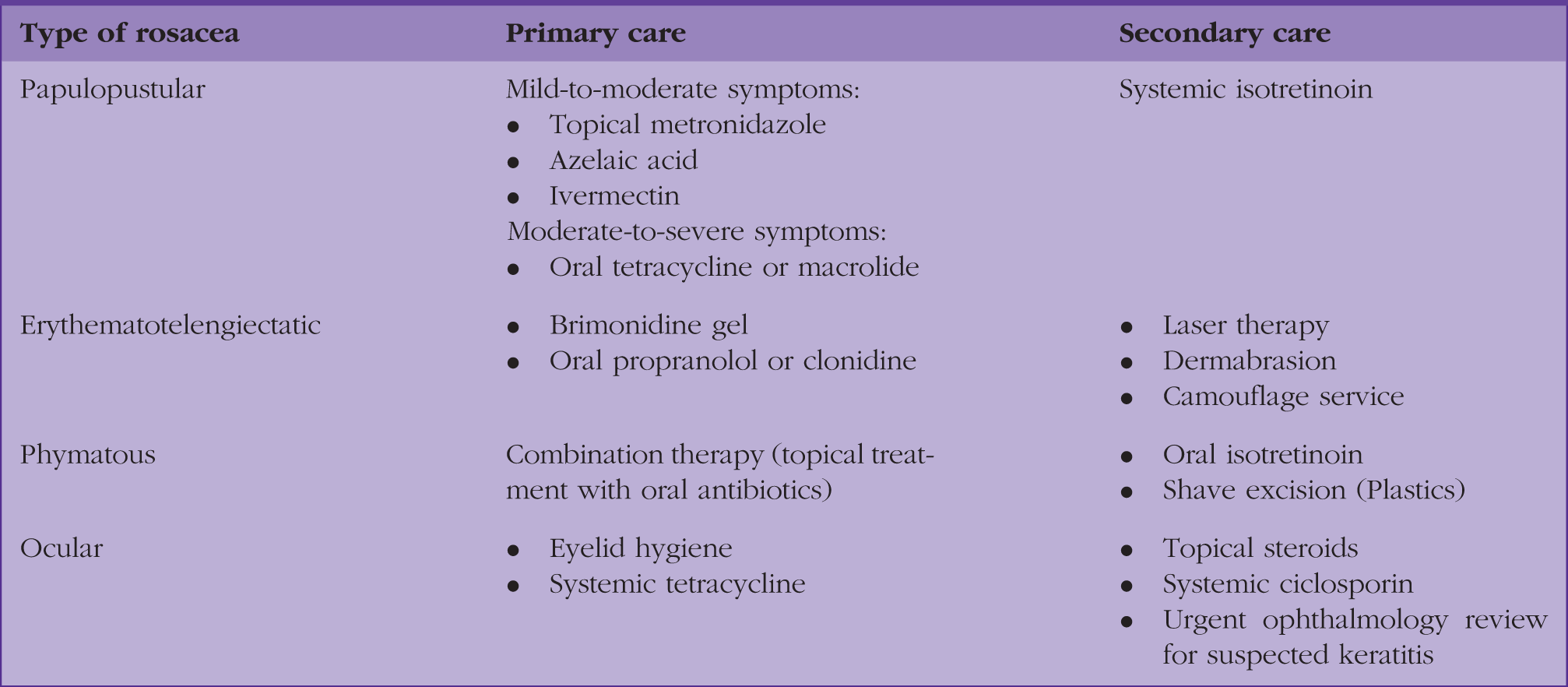
Treatment options.
Papulopustular rosacea
Papulopustular type is one of the most common types of rosacea and can usually be managed in primary care. Treatment choices, depending on the severity of the presentation, could be either topical, systemic or a combination of both.
Topical treatment
Topical treatment for papulopustular rosacea.

Oral medicines
Patients with moderate-to-severe rosacea, papulo-pustular rosacea and rosacea resistant to topical treatment should be treated with oral antibiotics, either on their own or preferably in combination with a topical treatment.
Tetracycline antibiotics such as lymecycline (408 mg once daily), oxytetracycline (500 mg twice daily) or doxycycline (40 mg once daily) are quite effective (PCDS, 2018). Tetracycline antibiotics are absolutely contraindicated in pregnancy and can also cause a photosensitive rash. Macrolide antibiotics, such as erythromycin 500 mg twice daily, are an alternative option. The dose of the antibiotics can later be reduced after the disease has been satisfactorily controlled. Treatment should be prescribed for at least 3 months. Gastrointestinal symptoms, such as nausea and abdominal pain, are the most common side effects with tetracyclines and macrolides. The patient should also be counselled regarding chronicity of the condition and treatment, otherwise it might lead to poor compliance.
Oral retinoids, for example, Isotretinoin, can be used in rosacea resistant to the above treatments. Oral retinoid treatment should be initiated only by a specialist and sometimes low-dose oral isotretinoin can be used for long-term control of rosacea.
Erythematotelengiectatic rosacea
Erythematotelengiectatic rosacea is a type that is more difficult to treat satisfactorily in primary care. Treatment options can be divided into primary and secondary care options. One primary care option is brimonidine gel (Mirvaso). This works as an alpha-2 receptor agonist to reduce flushing. Unfortunately, it can cause rebound erythema, and the patient should be clearly counselled to try it at a low dose for a week before increasing towards a maximum dose of 1 g a day (which is equivalent to roughly five pea-sized amounts applied to the forehead, chin, nose and each cheek). If redness or burning occurs, they should stop using the gel and contact you, their GP.
Other agents that can be used for flushing are non-selective beta-blockers, such as propranalol (40 mg twice daily), or clonidine (50 micrograms twice daily). Compared with papulopustular rosacea, patients with erythematotelengiectatic rosacea are more likely to be referred to secondary care.
Laser treatment can be a very effective option for facial telangiectasia, but availability on the NHS is variable. It is important to inform patients that in some cases telangiectasia can recur even after laser treatment. Another option is referral to camouflage services, which can be effective in hiding the severity of the erythematous changes, especially in treatment-resistant cases.
Phymatous rosacea
Thickening of skin can be related to the chronicity of the disease. Early and aggressive treatment of rosacea might help to slow down the process to rhinophyma. However, once phymatous changes appear (see Fig. 2), surgery usually is the most effective option. These patients should be routinely referred to plastic surgery for shave excision. Other options include dermabrasion and CO2 laser peel.
Rhinophyoma (phymatous changes seen over nose and cheek).
Ocular rosacea
Mild ocular involvement can be treated in primary care with advice regarding good eyelid hygiene with regular cleaning using cooled boiled water or sodium bicarbonate solution. If needed, over-the-counter or prescribed eye lubricants can be used to help with dry eye symptoms, which are commonly present in ocular rosacea. Treatment with oral antibiotics (tetracyclines) has been shown to be very effective for ocular rosacea.
If ocular symptoms persist despite treatment, the patient should be referred routinely to an ophthalmologist. One of the known complications of ocular rosacea is keratitis (see Fig. 3), which causes red, painful eyes or blurred vision. Development of keratitis symptoms warrants an urgent referral to ophthalmology.
Ocular rosacea.
KEY POINTS
Rosacea is a common, chronic, facial rash that predominantly affects the Caucasian population Although it is three times more common in females, it is often more severe in males Presentation and treatment depends on the subtypes of the disease As it commonly affects face, it can affect peoples’ confidence and mental health Most cases of the rosacea can be managed in primary care Severe or treatment-resistant cases can be appropriately referred to secondary care for dermatology, plastics or ophthalmology review