
Abstract
People with severe mental illness are three times more likely to die prematurely than the general population. Three-quarters of deaths arise from physical illnesses, the biggest cause being cardiovascular disease (CVD), far commoner than suicide. Psychotic illness, adverse treatment effects, lifestyle and socio-economic disadvantage combine to markedly increase risks for CVD and diabetes, often ignored by inadequate or discriminatory healthcare. We argue for more proactive approaches to address cardiometabolic risks. CVD risk has been reduced in the general population over the last 30 years, but not for those with severe mental illness. Reducing this health inequality should be core business for primary care and is overdue. This article will focus on physical conditions arising as a consequence of experiencing severe mental illness, rather than those that may be a primary organic cause of psychosis.
The GP curriculum and protecting the physical health of people with severe mental illness
Be aware that people with severe mental health problems have an increased risk of morbidity and mortality due to cardiovascular disease and diabetes and understand that as a GP you have a significant role in prevention, detection and management of this physical co-morbidity Enable people who are experiencing mental health problems to engage as much as possible in understanding their difficulties and negotiates appropriate, acceptable management Understand why some people find it difficult to access primary care and mental health services with their symptoms, and what you can do to increase equity of access to care Be aware of the impact that social circumstances such as poverty, debt, inequalities and upbringing can have on mental illness, and that recovery is contingent on the effective management of those social circumstances Practice holistically and promote health. This is about the physical, psychological, socio-economic and cultural dimensions of health. It includes considering feelings as well as thoughts, encouraging health improvement, preventative medicine, self-management and care planning with patients and carers
Introduction
In the UK, the lifetime prevalence of schizophrenia and bipolar disorder is 0.72% and 1–2%, respectively. These are psychotic disorders that are characterised by changes in perception and thinking, mood, and behaviour. Varying levels of insight are common. Stigma and social isolation frequently compound these difficulties with strained relationships, disrupted education and employment, and financial and accommodation uncertainties.
A GP with an average list size of 1577 patients (Baird et al., 2016) can expect about one patient per year to present with a new psychotic illness. Of these, about 20% will fully recover following a single episode. However, most continue to experience psychological and social difficulties; of these about half achieve good levels of social functioning, with the others experiencing a more difficult course, sometimes leading to severe disability; many develop poor physical health. This means that every general practice in the UK cares for substantial numbers of patents affected by severe mental illness (SMI) who have substantial ongoing needs. GPs and primary care teams can build up a relationship over time and help these patients and their families to cope positively with their healthcare needs.
Compared with the general population, life expectancy is reduced by around 15 years in females and 20 years in males with SMI. Suicide rates are particularly high in the first 5 years of psychosis. However, overall many more premature deaths arise from physical illnesses including cardiovascular disease (CVD), diabetes, smoking-related pulmonary disorders, drug and alcohol-related disorders, some cancers, and infectious diseases such as human immunodeficiency virus infection and hepatitis. Type 2 diabetes is two to three times more frequent, affecting 10–15% of people with SMI. CVD is three times more frequent than in the general population and the single biggest cause of a still widening mortality gap (Sami et al., 2017).
Case study 1. Mary’s story.
Mary is the eldest of David’s three children and developed schizophrenia 25 years ago when aged 16. Now in her 40s, she generally enjoys life, supported in an excellent residential care home close to where David and his wife Ann live. However, Mary experiences severe psychological impairments, due to her schizophrenia and learning disability; adverse physical effects, due to her antipsychotic medication (clozapine); and more recently some physical co-morbidities with additional treatment/care requirements. In contrast with her brothers, Mary requires support with all aspects of her life. Her poor experiences of initial care motivated a career change for David. David retired as a GP Principal in 2002 to engage in mental health service reform.
(Please note: This story is illustrative of one individual’s lived experience of having a SMI and is not meant to be representative of all patients with SMI.)
Why do people with SMI die early from CVD and diabetes?
Psychosis typically emerges in late adolescence/early adulthood. As Mary’s experience illustrates, poor mental health often combines with antipsychotic-induced appetite and weight gain, unhealthy lifestyle and social disadvantage. Cardiometabolic risk can rapidly escalate to put this vulnerable group on a path towards CVD and diabetes at a much younger age than the general population. Metabolic syndrome, a collection of conditions thought to be due to a combination of genetics, lifestyle and pharmacological interactions, occurs at much higher levels in those with SMI than the general population (De Hert et al., 2012).
GPs have focused on the middle aged or elderly general population, through the Quality and Outcomes Framework (QOF) and the NHS Health Check commencing from age 40 years. However, delaying primary prevention until age 40 may be too late for the young vulnerable population with SMI, emphasised by their diverging trajectory towards metabolic syndrome:
At onset of psychosis, the rate of metabolic syndrome compares with that of the general population By age 40 years, people with schizophrenia are three times more likely to experience metabolic syndrome than peers without psychiatric illness (De Hert et al., 2012) Presence of metabolic syndrome confers treble the risk of heart attack or stroke and 5-fold the risk of type 2 diabetes All this in an SMI population who are also three to four times more likely to smoke
Smoking
Smoking cessation is a public health priority to help tackle the largest preventable cause of death in the UK. Strikingly, 42% of all tobacco smoked in England is by those with mental disorders. Furthermore, those who have a SMI start younger, smoke more, inhale deeper, and spend a greater proportion of their income on cigarettes. Over half of people in their first episode of psychosis already smoke, and around 60–70% of those with established SMI smoke. Rates have remained steady over many years, contrasting with the steady decline in UK general population rates to now under 17%. As well as the myths referred to later in this article, other factors to help explain the high smoking rates include socio-demographic disadvantage, a culture of smoking within mental health services, smoking cessation services that are unsuited to the needs of patients with SMI and a possible causal link between smoking and psychosis (Gurillo et al., 2015).
Nutrition and physical activity
Compared with the general population those with SMI are twice as likely to be sedentary, and more likely to eat diets low in fruit and vegetables and high in fat and sugar. Antipsychotic-induced craving for food commonly drives high levels of calorie intake.
Antipsychotic medicines
Almost all antipsychotic medicine can cause weight gain and lipid and glucose disturbance, liability varying between drugs with olanzapine and clozapine the most likely to do so (De Hert et al., 2012). The scale of early weight gain is striking, averaging 12 kg within the first 24 months of treatment (Fig. 1). However, concern is not limited to cardiometabolic impact. We should consider the patient’s perspective and ask: ‘How must this weight gain feel for a young person experiencing psychosis and its treatment for the first time?’ It is not surprising that some patients discontinue treatment or disengage from services, only to risk a detrimental and dismal cycle of relapsing psychosis and problematic service re-engagement.
Published with kind permission from Professor Mario Alvarez-Jimenez. Based on the findings of Alvarez-Jimenez et al., 2008.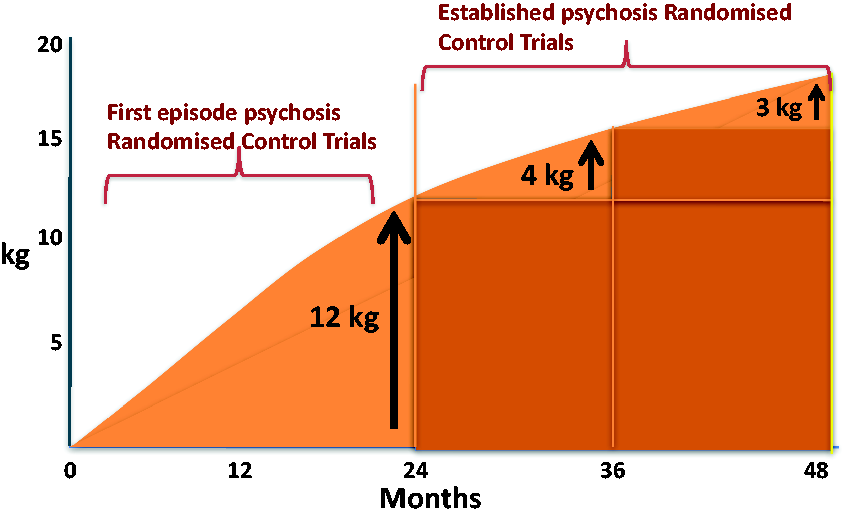
Healthcare
Reporting a focus group study, Professor Lester describes how people with SMI regard primary care as the cornerstone of their physical and mental health care, valuing the continuity and holistic approach (Lester et al., 2005) reflected by their annual consultation rates of about 13 per year. A more recent study of 1150 patients with SMI drawn from 64 practices across England found average consultation rates had plummeted to only three per year, barely higher than for the wider practice population, and practice nurses were half as likely to see people with SMI as the wider practice population (Reilly et al., 2012).
Despite annual physical health checks for people with SMI being incentivised through the QOF since 2004, the ‘2012 National Audit of Schizophrenia for England and Wales’ reported less than a third of over 5000 patients audited received a completed cardiometabolic risk assessment within the previous 12 months. Even when assessed, many of those with identified risks received no intervention (Crawford et al., 2013). This may reflect barriers to accessing routine health checks and poorly coordinated primary and mental healthcare services. A survey of 314 practices in Scotland revealed under-recognition and under-treatment of CVD in people with schizophrenia (Smith et al., 2013). Despite such evidence of health inequality, the incentivised requirement to monitor cholesterol, blood glucose and body mass index (BMI) was retired from the QOF in England in 2014. This removal of incentives has had a negative impact on patients demonstrated in research commissioned by NHS England (Wilding et al., 2018). This found significant reductions in annual monitoring, almost 20%, followed immediately suggesting that this population’s health may assume lower priority without incentives and prompting for primary care.
Case study 1. Mary’s story (continued).
Following severe psychosis, several ineffective conventional antipsychotics, a journey across Child and Adolescent Mental Health Services (CAMHS)/adult service divides, and psychiatric in-patient settings Mary’s psychotic terror eventually abated on clozapine. Use of clozapine was delayed due to concerns about potentially life-threatening white cell disturbance and the need for continued monitoring. Clozapine’s greater efficacy, although welcome, could not undo the effects of rehabilitation by the NHS on a 20-year-old in the local asylum. Heavily sedated, disconnected from all normal life and with staff rewarding her with extra helpings of pudding to quell antipsychotic-induced food cravings because they felt sorry for her, Mary’s BMI rose from 22 kg/m2 (pre-treatment) to 34 kg/m2 in just 3 years. Once fit and active, she became totally inactive. Fortunately, Mary did not engage with the ward’s established smoking culture.
Improve the physical health of those with SMI: Don’t just screen, intervene
High rates of CVD and diabetes in people with SMI are predictable, but also avoidable. The best way to tackle these physical co-morbidities is through prevention and early intervention. This approach is the basis of the Lester resource, tailored to respond proactively to cardiometabolic risk from the onset of psychosis and its treatment. Although the resource focuses on antipsychotic medication, many of the principles apply to other psychotropic medication given to patients with long-term mental disorders. For example, patients with bipolar disorder also experience high rates of CVD and diabetes associated with mood stabilisers.
The Lester resource was adapted and developed for UK use from an Australian version by the late Helen Lester with the RCGP and the Royal College of Psychiatrists. It was updated and endorsed by the National Institute for Health and Care Excellence (NICE) in 2014. It is consistent with wider NHS cardiovascular targets, but identifies the particular needs of this, often younger, high-risk population. The Lester resource encourages collaborative care; its framework for identifying and treating abnormal CVD risk utilises a simple traffic-light system to support clinicians in providing a consistent approach across services. For example, when a mental health nurse finds a patient with elevated blood pressure, in the red for CVD risk, that patient can expect further assessment, usually directed to the GP, to diagnose and treat hypertension, restoring CVD risk to green status.
GP or a psychiatrist?
The assignment of lead clinical responsibility for monitoring physical health is another key aspect of NICE guidance and the Lester resource:
The secondary care team should maintain responsibility for monitoring a person’s physical health and the effects of antipsychotic medication for at least the first 12 months or until the person’s condition has stabilised (whichever is longer) (NICE CG178, 2014) GPs and practice nurses should monitor the physical health of people with psychosis or schizophrenia when responsibility for monitoring is transferred from secondary care at least annually. The health check should be comprehensive, focusing on physical health problems common in people with psychosis and schizophrenia (NICE CG178, 2014)
The overarching principle is that psychiatrists and GPs should collaborate to ensure treatment plans are shared and that physical health is monitored and supported by clear lines of responsibility for further investigation, intervention and follow-up. Organisationally the practice SMI register helps the GP manage their responsibilities towards these collaborative arrangements. The SMI register includes those patients diagnosed with schizophrenia, bipolar disorder or ‘other psychosis’. Maintaining the register should not be a tick-box exercise. Registration should be continually updated to include newly diagnosed patients. Crucially the patient and carer should be actively involved in monitoring and management.
Systematic monitoring : ‘Don’t just screen, intervene’
Lester resource monitoring schedule.

Useful resources.
Encourage smoking cessation
GPs and primary care nurses have an opportunity to encourage and support smoking cessation at the annual review. However, some myths can perpetuate health inequality:
‘Smoking is good for people with mental disorders’ – No! Stopping smoking is the most effective way to live longer. And stopping smoking is as effective as antidepressants for treating mild-to-moderate depression (Taylor et al. 2014) ‘People with mental illness can’t stop smoking’ – No! Not only do they want to stop smoking – with appropriate support they can ‘Interventions that work for the general population do not work for people with mental illness’ – No! Evidence-based smoking cessation interventions for the general population can be just as effective for people with SMI
Evidence shows that people with SMI are reluctant to access conventional ‘opt-in’ smoking cessation services. However, a recent study has shown that bespoke smoking cessation offering more intensive and sustained support is feasible and the results of a recently completed randomised control trial are awaited (Gilbody et al., 2015). For detailed practical considerations, see useful resources: ‘Primary Care Guidance on Smoking and Mental Disorders’.
Promote healthier lifestyles
There is limited evidence that intensive lifestyle programmes can increase physical activity and reduce weight by around 3 kg. These programmes are more effective when delivered early in the course of psychosis. Engaging practical support from friends and family can be helpful. Tackling social determinants is important in overcoming limited budgets, nutritional knowledge, shopping/cooking skills, and poor access to recreational activities.
Treat hypertension
Compared with the wider practice population, patients with SMI are about twice as likely to develop hypertension and three times more likely to die from hypertension-related disease (Franklin and Wong, 2013). Treatment targets are the same as for the general population. Potential adverse drug interactions can arise and advice from the pharmacist can be helpful.
Treat dyslipidemia
Statins can lower total and low density lipoprotein (LDL) cholesterol effectively and safely in people with SMI, but a consequent reduction in CVD has yet to be demonstrated in trials. Again, potential adverse drug interactions can arise and pharmacist advice should be considered.
Treat diabetes and pre-diabetes
Co-morbid diabetes is especially challenging to manage and requires close collaboration between mental and physical health services. It is important to proactively identify and treat those at high risk of diabetes. Intensive lifestyle programmes can reduce the likelihood of developing diabetes, but if these prove ineffective, pharmacological approaches such as metformin can help. Other options are considered in the Lester resource.
Prescribe safely
Antipsychotic medication should be monitored closely and regularly for efficacy and side-effects. Antipsychotic medication should only be initiated by a GP for someone with a first episode of psychosis in close collaboration with a consultant psychiatrist (NICE, 2014). Although the decision to prescribe is usually initiated by psychiatry, if problems arise GPs should be ready to advocate for a patient and alert the prescribing clinician. Three examples of clinical safety emphasise the importance of collaborative working between GPs and psychiatrists:
Rapid early weight gain (e.g. 5 kg in 3 months) alerts to a propensity to severe weight gain and should prompt urgent psychiatric review. There is some evidence that switching to drugs less likely to cause weight gain can help. Benefits should be balanced against the risk of relapse of psychosis Rarely, marked glucose or lipid disturbance can occur within weeks of commencing antipsychotics. These metabolic abnormalities may settle on withdrawing the antipsychotic responsible. A patient, recently diagnosed with psychosis can occasionally present with life-threatening diabetes (e.g. diabetic ketoacidosis) even in the absence of weight gain (De Hert et al., 2012). Both GP and psychiatrist must be alert to this possibility. If any patient becomes rapidly unwell it is vital that random or fasting blood glucose is tested. Stopping smoking can affect hepatic metabolism of certain psychiatric drugs causing drug levels of antipsychotics such as clozapine and olanzapine to rise by up to 25% within a week and 50% within a month and risking clozapine toxicity. Similar effects can occur with certain antidepressants and benzodiazepines. These effects can work in reverse for those patients who resume smoking. Therefore, prescribing should be carefully managed when considering smoking cessation. Always inform and involve patients, coordinating primary and secondary care with smoking cessation services.
Prescribing: Some clinical safety concerns of which to be aware.
First- or second-generation antipsychotics and risk profile
The classification of drugs into older first-generation and newer second-generation drugs is unhelpful and largely a marketing device. Efficacy and side-effects vary according to individual drug response. Neurological side-effects may occur with any antipsychotic, but are commoner with some of the older drugs, particularly haloperidol (e.g. parkinsonian stiffness and tremor, akathisia, rare but difficult to reverse tardive dyskinesia causing involuntary movements usually of jaw and tongue). However, weight gain and metabolic disturbance are more marked with olanzapine and clozapine in particular. Individual treatment plans aim to maximise benefits and minimise adverse effects.
It is vital to support patients in understanding the risks and benefits of treatment, exploring their preferences engaging them in decisions about treatment. Rethink produces a helpful factsheet on antipsychotic side-effects to aid these discussions at www.rethink.org/diagnosis-treatment/medications/antipsychotics/side-effects.
Improving access to primary care for those with SMI
Practical tips for facilitating access to primary care.
However, perhaps Professor Lester’s most important message was to caution against the stigma that can ‘seep and creep’ into clinical practice behind the health inequalities experienced by patients with psychosis like Billy, concluding: ‘ above all, I think, if we examine our hearts, it boils down, quite simply, to being bothered about Billy’.
Support families and informal care-givers
Many people with SMI either live with, or are closely supported by, informal carers, often members of their family. Informal carers can provide invaluable practical support: for instance, by encouraging healthier diets and physical activity, by supervising treatment and monitoring requirements, and by noticing when things are not right and offering advocacy when needed. Many carers complain they receive insufficient information about the person they support. They can feel excluded from the process of care, yet may provide large amounts of support with little guidance. Clinicians need to listen to the concerns of the carer and value their contribution as part of the system of support for a patient.
GPs often overlook the impact of long-term care-giving. Carers suffer significant social, economic and health consequences. The initial distress of discovering a family member has a psychosis may give way to exhaustion and ‘burn-out’ as the condition continues. As a group, carers of people with SMI are more isolated than carers of those with other conditions. They experience poorer quality of life and higher levels of physical and mental co-morbidity than ‘non-carer’ peers (Onwumere et al., 2016). For these reasons, they can be viewed as a vulnerable group in their own right; and are likely to benefit from proactive and systematic support in primary care. Moreover, the majority of carers of people with SMI identify their GP as the health professional most able to improve their lives.
Thus, GPs are uniquely placed within the NHS and identified as trusted confidantes offering long-term healthcare to individuals and families, able to understand the context in which problems arise and provide holistic support. A helpful resource for carers is: https://www.rethink.org
Conclusions
The scale and nature of inequalities in morbidity and mortality with SMI demand holistic and integrated services. Primary care can work with and build on the advances of the ‘Early Intervention in Psychosis’ services to transform the early experiences of care, and then to consolidate those gains with on-going and collaborative care for patients whose needs persist. The strengths primary care brings individuals with a person-centred and holistic approach also bring an ability to support the contribution of family and other informal care-givers. Nevertheless, perhaps the greatest obstacle to leading fulfilled and healthy lives for people with SMI is their experience of stigma, not just from the general public, but also from health professionals in how we practice, think and talk. Much of what is needed hinges not on new science or technologies, but rather on our own willingness to empathise, to get to know our patients and their families, and to find practical ways together of encouraging healthier lifestyles. We must deliver the monitoring and interventions appropriate for all patients at high risk of co-morbidity and reduced life expectancy. A future blighted by poor physical health should not be the inevitable consequence of experiencing a psychosis or its treatment.
Case study 1. Mary’s story (continued).
Twenty-five years on from the onset of psychosis, Mary now deals with a mixture of mental and physical disorders and treatments, against a backdrop of increasing reliance on others. Many of the seeds of Mary’s future poor physical and mental health were sewn early in the course of her psychosis. This was also the toughest time for Ann and David as they struggled to adjust to their daughter’s illness and the pessimism of what was offered to someone so young and with a lifetime ahead. Through all the different practitioners and services since, they have been the constant, holding the narrative of who Mary is and how her increasingly complex medical history affects her. They have learnt how to hold hope for Mary in bad times, and to notice and celebrate her improvements in better times. And despite her many difficulties, they are proud of how Mary has come through. She lives for today, loves her new home, takes pride in her appearance and is a valued member of her family.
KEY POINTS
‘Don’t just screen, intervene’ – adopt the mantra of the Lester resource to act on identified risks Engage and support patients and their families to make well-informed treatment choices, to understand the purpose of physical health monitoring, and to agree and implement a practical well-being plan to mitigate relevant physical health risks from the onset of psychosis Promote healthier lifestyles and help address key social determinants on practical issues such as poor housing conditions, lack of access to recreation and physical activity, lack of cooking skills and a limited budget for food Make reasonable adjustments to facilitate access to primary care, for example, flagging notes, offering proactive care, providing longer pre-bookable appointments For those patients who fail to engage despite all efforts, consider a combined outreach approach working with the mental health team Identify carers of people with SMI as a vulnerable patient group in their own right within primary care who can benefit from proactive engagement and support to meet their own high levels of emotional and physical health need
Footnotes
Acknowledgements
Ms Mary Shiers and Mrs Ann Shiers who gave permission for writing this article.
Dr Curtis, Professor Samaras and Dr Newall, Sydney, Australia for enabling the Lester UK adaptation from their original HETI Positive Cardiometabolic Health algorithm.
In special memory of the late Helen Lester: For her contribution to the resources listed and her dedication to improving the lives of people affected by mental illness.
Conflicts of interest
DS is expert advisor to the NICE centre for guidelines and a member of the current NICE guideline development group for Rehabilitation in adults with complex psychosis and related severe mental health conditions; Board member of the National Collaborating Centre for Mental Health (NCCMH); Clinical Advisor (paid consultancy basis) to National Clinical Audit of Psychosis (NCAP); views are personal and not those of NICE, NCCMH or NCAP.
CCG is Curriculum Advisor, RCGP Mental Health.
This article represents the authors’ views and not those of RCGP, NIHR, NICE, NCCMH or the WHO guideline group.