
Abstract
Chronic urticaria (CU) is characterised by recurrence of hives or angioedema almost daily for at least 6 weeks. It is benign, but can be intractable, and hence, frustrating for patients and physicians alike. Diagnosis is clinical and based primarily on an allergy-focused history and physical examination. Routine referral for allergy testing is not always required. The goal of treatment is symptomatic relief with non-sedating antihistamines. Targeted screening for nutritional deficiency is of proven benefit. Triggers of CU in childhood are varied and different from CU in adults. This article aims to update GPs on CU in children, focusing on management in primary care, guidance on specialist referral and details of the subsequent targeted diagnostic pathway with non-invasive testing undertaken by paediatricians.
The GP curriculum and urticaria in children
Demonstrate appropriate history taking for patients with skin problems, including past personal history, family history, chemical contacts, and drug usage Understand how to recognise common skin conditions in primary care and instigate appropriate treatment Recognise rare but potentially important conditions and know when to refer to secondary or tertiary care Manage and appropriately treat common and rare but important paediatric conditions encountered in primary care Ensure that parents or carers, children and young people receive information, advice and support to enable them to share responsibility for self-care of chronic conditions and exacerbations Co-ordinate care with other primary care professionals, paediatricians and other appropriate specialists, leading to effective and appropriate care provision, taking an advocacy position for the patient or family when needed
Definitions
The European Academy of Allergy and Clinical Immunology (EAACI) has defined urticaria as a condition that is characterised by wheals, angioedema or both. Wheals consist of three typical features: central swelling of variable size (from 1 mm to ‘giant uricaria’), surrounded by blanching erythema and associated with intense itchiness. These rashes tend to ‘travel’ around the body, with peaks between 8 and 12 hours and then resolution by 24 hours (Zuberbier et al., 2014); a useful pointer for making the diagnosis. Figure 1 and 2 demonstrate wheals over a patient’s arm and lateral foot, respectively.
Wheals over the arm of a child. Wheals over the foot of a child.

Angioedema is defined as well-demarcated erythematous swelling, occurring within deep skin structures and subcutaneous tissue or mucous membrane (Zuberbier et al., 2018). It may be painful, but it is not itchy. Unlike wheals, angioedema tends to last longer, up to 72 hours. Often both urticaria and angioedema co-exist as relapsing and remitting episodes (Zuberbier et al., 2014).
It is important not to confuse urticaria with other medical conditions, such as anaphylaxis, urticarial vasculitis, hereditary angioedema or other auto-inflammatory disorders. Spontaneous urticaria is usually divided into acute and chronic forms. In acute spontaneous urticaria (ASU), the more common form of urticaria, episodes present for less than 6 weeks, whereas chronic spontaneous urticaria (CSU) defines the condition with symptoms that persist almost daily for more than 6 weeks.
Classification
ASU is usually self-limiting and does not require any investigation. Common triggers include viral illness, recurrent exposure to food allergens, aeroallergens or drugs. Unlike adults, viral-induced urticaria (i.e. upper respiratory tract viruses) contributes up to 80% of the cases in children. This can sometimes lead to the false belief that a food allergy exists, causing unnecessary stress to patients and unnecessary specialist referral. Therefore, an allergy-focused history plays a fundamental role in these situations. In exceptional cases where urticaria is allergy related (i.e. drugs, food), skin prick testing (SPT) may be useful to confirm the diagnosis and help with future avoidance of similar triggers. Specific Immunoglobulin E (IgE) blood tests may be requested by secondary or tertiary specialists if the acute clinical history does not align with the SPT results. There is therefore no role for IgE testing in primary care.
CU subtypes.
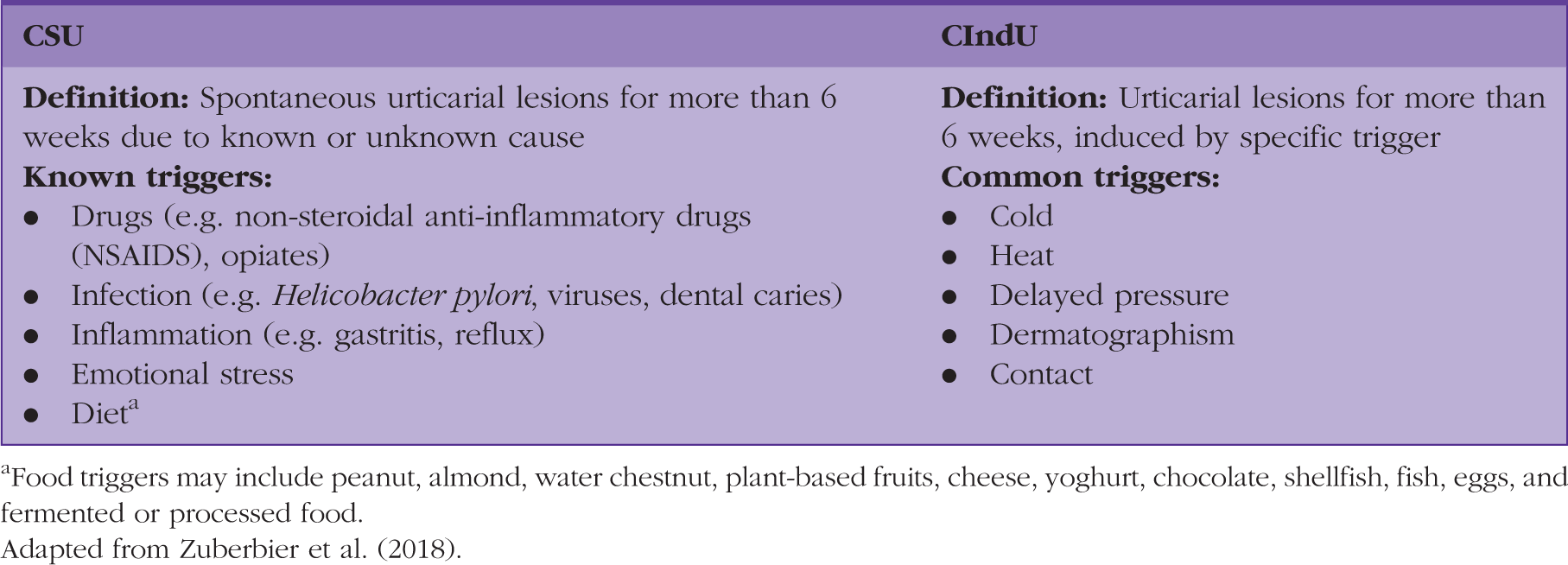
aFood triggers may include peanut, almond, water chestnut, plant-based fruits, cheese, yoghurt, chocolate, shellfish, fish, eggs, and fermented or processed food. Adapted from Zuberbier et al. (2018).
Pathophysiology
Urticaria is a mast-cell-driven disease. Mast cells (‘Mastzellen’ in German, or ‘well-nourished cells’) are circulating large cells that normally stay in close proximity to blood vessels of skin dermis and mucosa. Activation of mast cells is triggered by various stimuli, resulting in three different mechanisms, depicted in Fig. 3.
Authors interpretation of the pathophysiology of urticaria.
Cross-linking of the specific stimulus of an IgE-mediated receptor stimulates mast cell degranulation, followed by immediate release of vasoactive mediators, predominantly histamine (Zuberbier et al., 2018). This behaviour results in sensory activation, vasodilatation, increased blood flow and increased vascular permeability (Powell et al., 2015). Wheals are caused by oedema of the upper and mid dermis, as a result of leakage of serum into the tissue following mast cell activation. In angioedema, a similar phenomenon occurs primarily in the lower dermis and the subcutaneous tissue.
Activated mast cells trigger release of cytokines (i.e. interleukin-1, tumour necrosis factor-alpha) in a later phase, between 6 and 24 hours after stimulation. These cytokines then activate endothelium, which in turn allows infiltration of leucocytes into the dermis, particularly eosinophils (Hennino et al., 2006). This late phase reaction induces maintenance of skin inflammation, expressed clinically as indurated erythema (Kitao et al., 2001). Activated mast cells also induce T-cell infiltration into the dermis, which then contributes to the chronicity of the lesions (Frandji and Mourad, 1998). This mechanism is supported by the excellent clinical efficacy of ciclosporin by suppressing T-cell activity.
In certain groups of patients, mast cell activation initiates the synthesis of leukotrienes and prostaglandins, which play a role in early and selective recruitment of leucocytes, extending the chronicity of the condition (Hennino et al., 2006).
Making the diagnosis
The three recommended diagnostic aims in CU include (Zuberbier et al., 2018):
Ruling out differential diagnoses Assessing disease severity, impact, and control Identifying triggers of exacerbation
Clinical history and examination
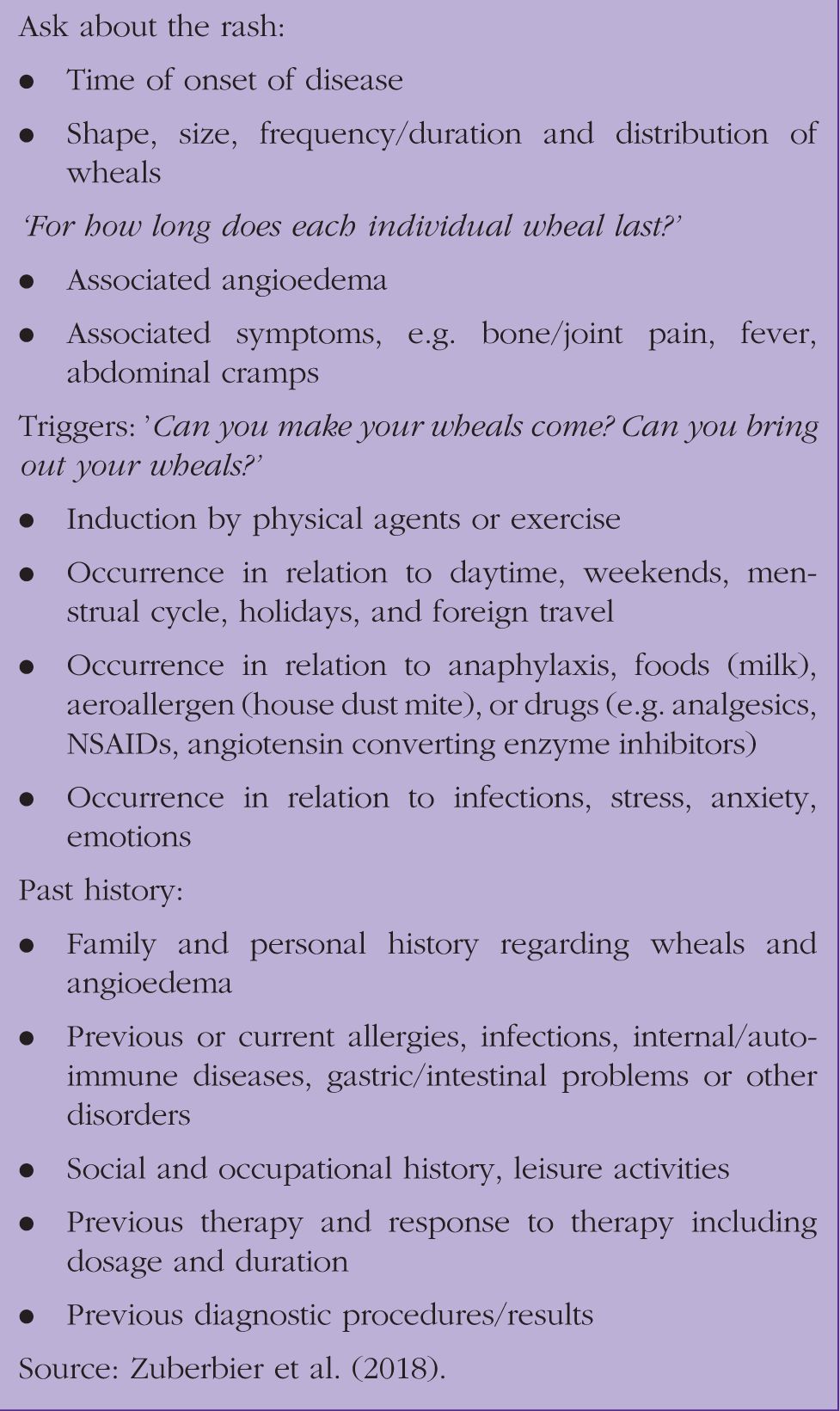
In children, CU is mainly a clinical diagnosis, where focused history and detailed physical examination play a fundamental role. Clinical history should include detailed questions on the frequency, timing and duration of attacks, pattern of recurrence, specific triggers and associated symptoms such as pruritus or pain. Drug and family history should be fully documented. Photographs are often helpful in the diagnostic process and patients may have compiled a symptom diary, which can be useful in identifying possible triggers for the rash.
Taking a good history.
Investigation
Children with CU are frequently over-investigated. As mentioned above, clinical history is very important in this context. In patients with a history strongly suggestive of CIndU, referral should be made to the tertiary allergy specialists for provocation testing. This should be performed by experienced specialists, due to the possibility of severe allergic responses during provocation testing. These could range from mild systemic symptoms, such as dizziness, diarrhea/vomiting and wheeze, to anaphylactic shock (Magerl et al., 2016). Such tests include the ‘ice cube test’ for cold-induced urticaria, the dermatographism test, the pressure test and an ‘exercise test’ for cholinergic urticaria.
There has been a recent change in the recommended first line diagnostic tests of CSU (Zuberbier et al., 2018). A series of multiple blood tests to exclude differential diagnoses in CU are no longer recommended. If a focused clinical history and examination are strongly suggestive of CSU, investigations are not required in most cases. The only three suggested first line laboratory tests are: differential full blood count (FBC), erythrocyte sedimentation rate and C-reactive protein.
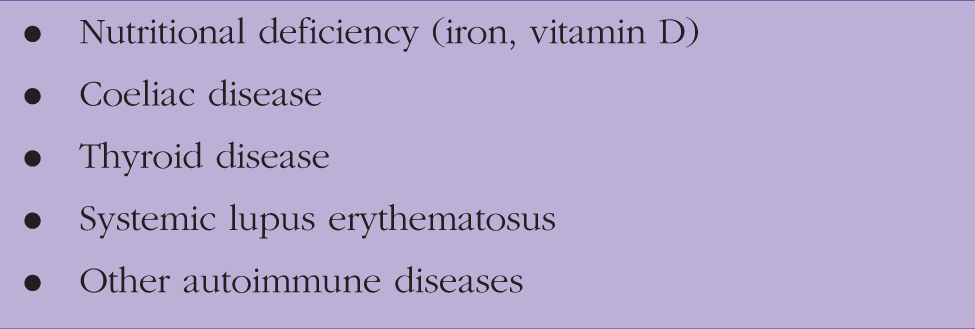
Further second and third line diagnostic tests are deemed necessary only if a strong relevant clinical history is present. Referral to secondary or tertiary paediatric care is warranted in these cases. Final complex investigations might be undertaken once referred to tertiary care to exclude other rarer associated conditions, as listed in Box 2. These tests are shown in Fig. 4.
Recommended diagnostic workup of chronic urticaria. Conditions diagnosed in infants and children with CSU.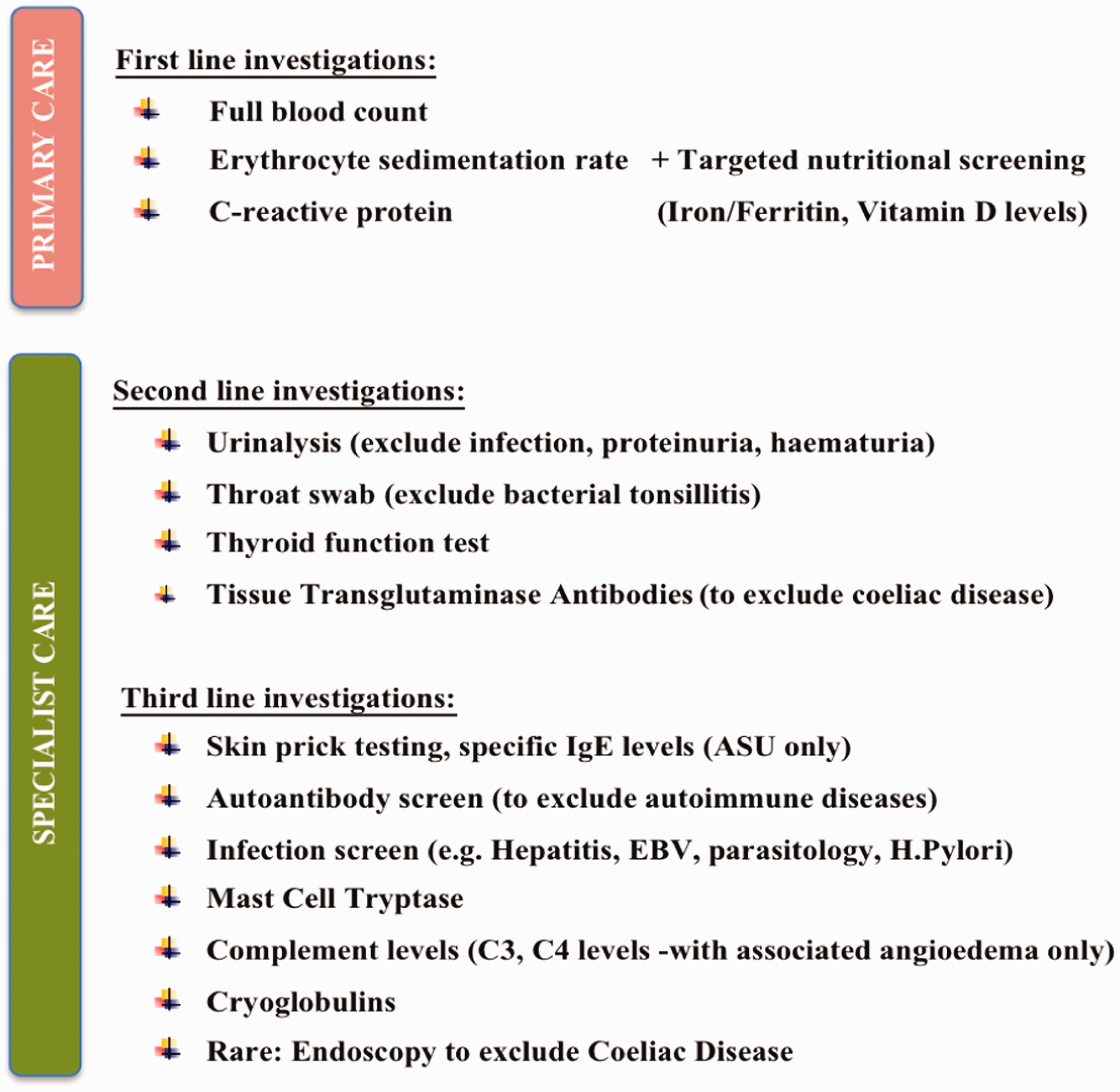
The UAS7: The suggested assessment tool for disease severity in CSU.
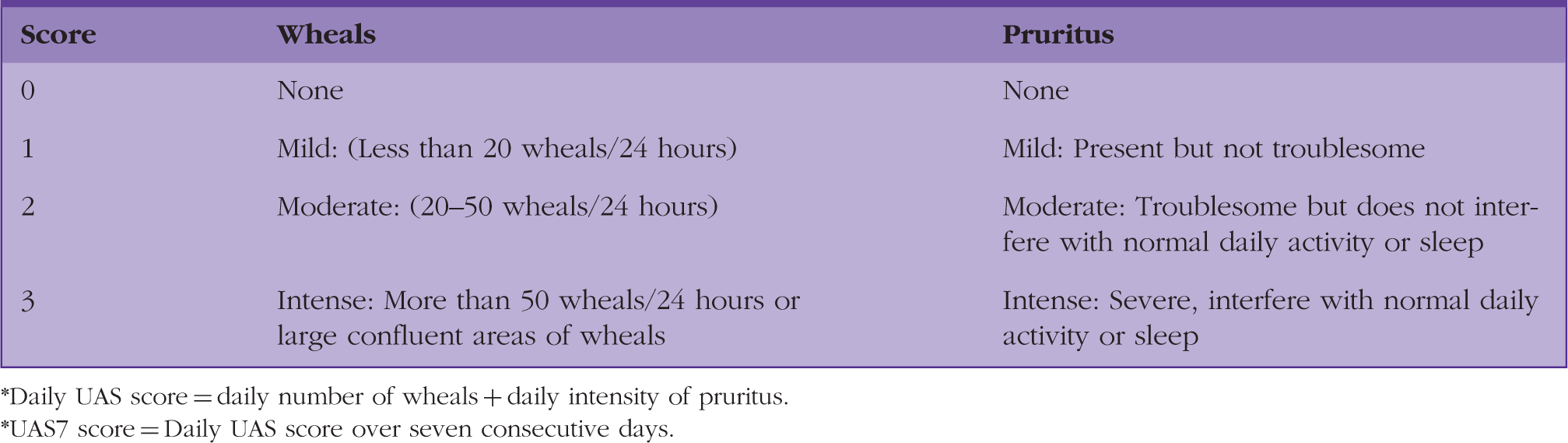
Daily UAS score = daily number of wheals + daily intensity of pruritus.
UAS7 score = Daily UAS score over seven consecutive days.
Current treatment of CSU
CSU is a disabling and challenging condition to treat. H1-antihistamines were the mainstay of symptomatic treatment for CSU until Omalizumab was introduced in early 2014. We have outlined the recommended guidance in the treatment of CSU below (Zuberbier et al., 2018).
First and second line pharmacological treatment
Antihistamines have been the treatment of choice for urticaria since the 1950s. The second-generation H1-antihistamines (SgAH) are now the first line treatment of CSU for both adults and children. Unlike the older first-generation antihistamines, they are safe to use with fewer non-sedative and anticholinergic side effects. Common SgAH medications include Cetirizine and Loratadine.
If there is no improvement with a SgAH at the licensed dose, the EAACI guideline 2018 recommends increasing the dose gradually up to a maximum of four times the licensed dose. Starting a second SgAH in patients with unresponsive CSU is strongly discouraged. Use of leukotriene receptor antagonists (e.g. Montelukast) is also no longer recommended, due to limited evidence of its efficacy (Zuberbier et al., 2018). If symptoms are refractory despite a high dose of SgAH, referral to the tertiary allergy services is warranted.
Third line pharmacological treatment
Omalizumab (Xolair®) is a monoclonal anti-IgE antibody that binds to IgE at its binding site to the high-affinity IgE receptor (Metz et al., 2017). It interferes with the activation of mast cells, which then prevents release of vasoactive mediators. It is given by injection subcutaneously in a tertiary hospital setting. It has been approved to treat refractory CSU, as an add-on therapy with high dose H1-antihistamines in patients above 12 years in age (Saini et al., 2015). There is still very limited evidence of the use of Omalizumab in infants and children, particularly on its clinical efficacy and safety. Alongside optimisation of compliance it is our experience that a trigger of the CSU in children can usually be found or it ‘burns itself out’ by adulthood.
Ciclosporin A is considered in severe cases where disease is resistant to Omalizumab with maximum dose of SgAH. It suppresses T-cell activity and subsequently blocks inflammatory infiltration to the dermis. Figure 5 illustrates an adaptation of the recommended treatment algorithm for CSU from the EAACI guideline of 2018. A similar algorithm can be used, with caution in children and pregnant or lactating women.
Treatment algorithm of CSU management.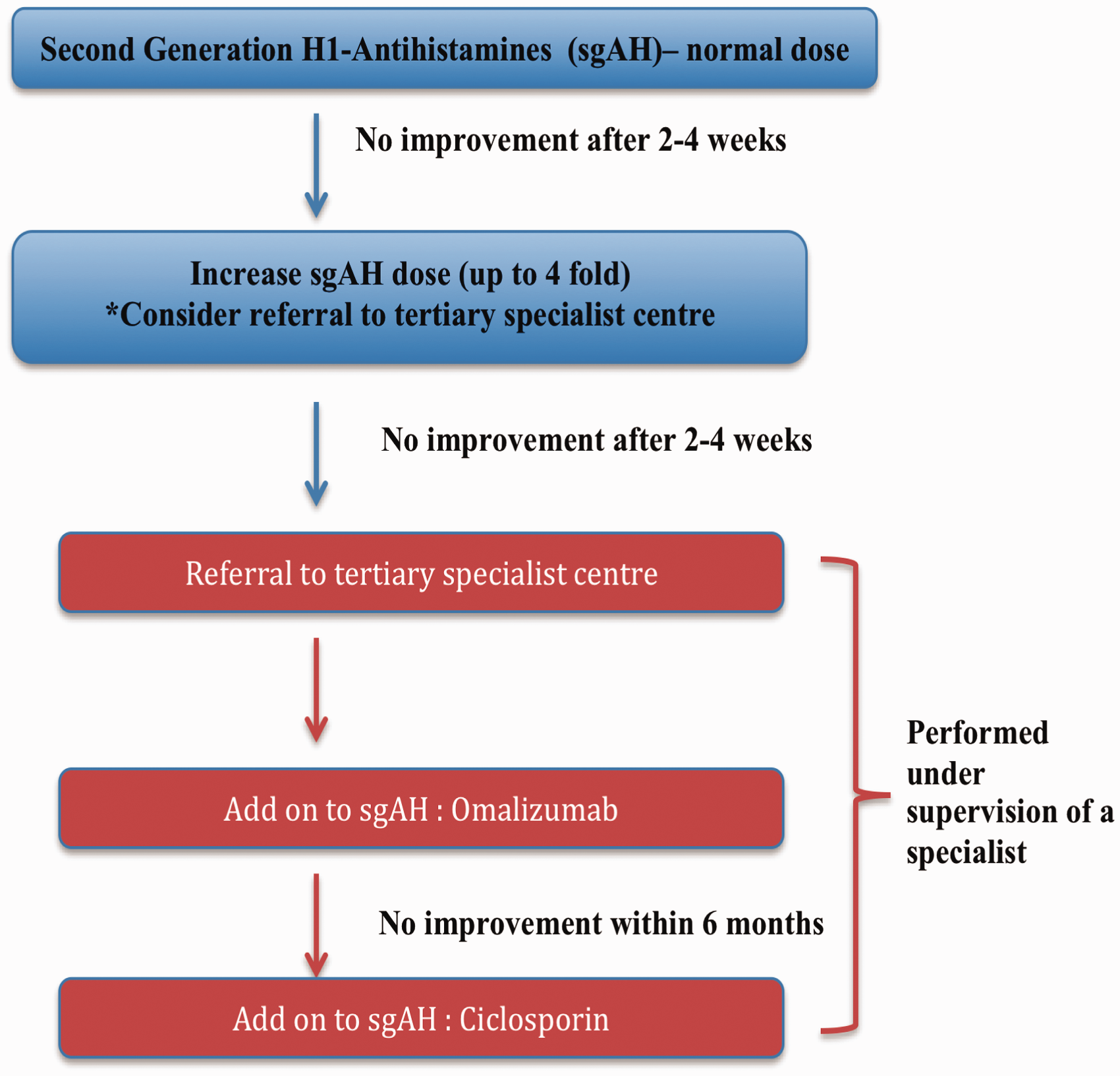
Targeted nutritional supplementation: A potential immunomodulator
A recent retrospective study at The Great North Children’s Hospital in Newcastle upon Tyne has demonstrated a potential relationship between CSU and certain nutritional deficiencies: particularly iron (Mahadevan et al., 2015). The study found that optimising the diet of infants and nutritionally deficient children (vitamin D and iron) can lead to resolution of CSU symptoms. Therefore, a targeted nutritional screen (FBC with hematinic screen) and supplementation of iron for infants and children with confirmed iron deficiency can be useful in primary care before further investigations or referral to allergy services.
Rare alternative approaches in treatment
There are alternative methods of managing refractory CSU, such as Sulfasalazine, Methotrexate, Dapsone, Mycophenolate Mofetil, phototherapy, intravenous immunoglobulin. Although systemic corticosteroids continue to be occasionally used for acute exacerbations, very little is known about the clinical efficacy of these drugs, and therefore, careful consideration by tertiary specialists is required prior to the use of these off-license medications.
The use of third line add-on options for CSU (i.e. Omalizumab) in paediatrics is uncommon, due to the debatable evidence and unclear long-term outcomes. The main treatment strategy involves identifying and treating the cause, ensuring compliance of H1-antihistamines and correcting nutritional deficiencies. All of these steps are effective in tackling severe CSU according to the available evidence.
Current treatment of CIndU
The management of CIndU is similar to CSU; however, ‘on demand’ treatment may be more useful in certain forms of physical urticarial (Zuberbier et al., 2018). Patients are encouraged to take antihistamines before anticipated contact with the trigger, for example, before swimming in patients with cold-induced urticaria.
KEY POINTS
CU is a disabling condition commonly seen in primary care CU is diagnosed primarily from clinical history and examination A detailed nutritional history is also essential Non-sedative antihistamines remain the first line pharmacotherapy Montelukast is no longer recommended as second line treatment Targeted nutritional supplementation, particularly vitamin D and iron, can play an important role in complete resolution of CSU