
Abstract
From cradle to grave, the gastrointestinal (GI) system is a common source of symptoms. So, what does it matter that someone is aged 88 years rather than 18 years? The answer is ‘a lot’. Differences range from changes in physiology to a growing impact of other illnesses on GI function. For example, deteriorating dentition and appetite can interfere with input at the top end of the tract, and a myriad of factors may disrupt transit, absorption and sphincter control at the other end. A multitude of challenges can face people in later life. This article offers 10 essential points about GI function in later life for GPs to consider.
The GP curriculum and the gut in later life
Provide the primary management of patients who have a digestive problem Understand the epidemiology of digestive problems as they present in primary care and their often complex aetiology Interpret common symptoms in general practice, including dyspeptic symptoms, abdominal pain, nausea, vomiting, anorexia, weight loss, haematemesis and melaena, rectal bleeding, jaundice, diarrhoea and constipation, and dysphagia Demonstrate a systematic approach to investigating common digestive symptoms, taking into account the prevalence of these symptoms in primary care and the likelihood of conditions such as peptic ulcer, oesophageal varices, hepatitis, gastrointestinal cancers and post-operative complications Show an understanding that digestive symptoms are frequently linked to psychosocial factors and may be associated with alcohol and drug usage Understand the indications for urgent referral for suspected gastrointestinal cancer
An understanding of the physical factors, particularly diet, exercise, ambient temperature and sleep, that disproportionately affect the health of older people An understanding of special factors associated with drug treatment in later life, e.g. the physiology of absorption, metabolism and excretion of drugs An understanding of the management of conditions and problems commonly associated with old age, such as falls, continence issues, confusion, dementia and cancer
Older people have habits based on a lot of gastrointestinal experience
Ask a 20-year-old about their bowels and, unless they are one of the unlucky ones with a specific condition, most will look at you with a degree of laissez-faire. They take their gastrointestinal (GI) function for granted, just like so many other aspects of their health. However, later in life when most people have weathered the misery of heartburn, gastroenteritis, constipation and all the other common problems, and really earned their toileting stripes, they tend to know what suits them. Most have a personal habit that they like to stick to: they know what they can or cannot eat, what stirs up their dyspepsia, what makes them loose or constipated. Personal habits are just that – individual and sometimes right across the spectrum of normal. I frequently hear things that make me raise an eyebrow. However, interfere with them at your peril. Although they do not always have a detailed knowledge about GI physiology, older people know their own gut, which is the best grounding for self-management even if it needs a little extra support when things go haywire. So, any consultation on a gut topic must revolve around the patient’s own perspective, values and goals if an effective management plan is to be achieved.
Age alone is rarely an issue before the ninth decade
Understanding clearly definable changes in physiology with age is fundamental to an appreciation of the problems that can develop. However, the question of what can be ascribed to ‘normal ageing’ and what is pathological is often a topic of debate. Nevertheless, in recent years evidence has accumulated to reassure us that GI physiology remains fairly reliable until well into the ninth decade of life (Hall, 2002).
There is little difference, for example, between a 20-year-old and an 80-year-old in terms of quantity and quality of biliary, pancreatic, and intestinal secretions, the absorptive capacity of the small intestine, and general nutritional requirements for height and weight (although there may be increased emphasis on certain nutrients, e.g. the amount of protein intake in the diet required to counteract sarcopenia).
Despite this, numerous age-related changes within the gut have been identified. These include, for example, degeneration of the myenteric plexus with loss of myelinated and unmyelinated nerve fibres, abnormal remyelination, and more widespread axonal atrophy (Hall, 2002). As a result, nerve conduction velocity declines, and autonomic responses are reduced. Meanwhile changes in nitric oxide and neuronal calcium regulation in local control of motility by the myenteric plexus affect smooth muscle contraction (Gomes et al., 1997). Animal models suggest that prolonged, lower-amplitude colonic contractions lead to slower gastric emptying of liquids and decreased faecal transit. However, the significance of many of these changes for healthy older people is not very clear.
Another example of age-related change, which has a more familiar significance, is increased fibrosis within the intestines and an increase in intraluminal colonic pressure, possibly as a result of a shift in the character of contractions from peristaltic to non-peristaltic (Hobson and Roberts, 2004). Along with slowing of colonic transit, these may contribute to an increased tendency to mucosal herniation, explaining the steady increase in diverticulosis with age. Is this considered normal ageing or pathology? This is debatable, and perhaps what matters most is how much the changes affect an individual. Fortunately, most people have considerable functional reserve, which means that these physiological changes tend to have little impact. Up to two thirds of people over 80 years in age have diverticulosis but only 1 in 4 of these will develop problems (Hall, 2002). However, in more extreme old age (sometimes described as the ‘oldest-old’, aged 85 years and above) physiological changes may be far more pronounced and more likely to disrupt function (Evans et al., 1998).
Even before food enters the mouth there may be hurdles to overcome
The daily process of thinking about, selecting and preparing food can become a significant challenge, especially for the oldest old. Declines in taste, smell, and appetite mean that food intake often drops with ageing (Boyce and Shone, 2006). More than 75% of people over the age of 80 years have evidence of major olfactory impairment.
Older people tend to be consistently less hungry than younger people, eat smaller meals, and have fewer snacks between meals and eat more slowly (Chapman, 2004). Between 20 and 80 years in age, there is on average, a decrease in energy intake of approximately 30%. This can lead to weight loss, which is not just unwanted adipose tissue but lean skeletal muscle – a condition called sarcopenia. The loss of lean tissue is associated with reductions in muscle function, bone mass and cognitive function, anaemia, dysfunction of the immune system, slow wound healing and recovery from surgery, and consequentially an increase in both morbidity and mortality (Nowson, 2007).
Add in common problems, such as reduced mobility (not only to get out to the shops, but also even just along to the kitchen to make a meal) or cognitive issues (which interfere with the sequential processing needed to pull together a meal) and the intake of nutrients and energy may become very unreliable. Home visits often reveal a haphazard diet of easy access food – biscuits and whiskey seems to be one common combination in the affluent villages of Surrey, in my experience. Even when families do their best to stock up the freezer with meals that can be reheated, these often go unused, especially if the person is left on their own to sort out meals, rather than sharing food with a friend or relative. Its no good just asking someone how well he or she is eating – you need to root around for evidence. Our occupational therapists (OTs) on their home visits frequently discover fridges and freezers stuffed with out-of-date food, or crates of empty beer bottles.
Solutions range from lunch clubs to add a social meaning to food, to flavour enhancement or using supplements such as salt or monosodium glutamate to an improve food palatability (shown to improve immune status as determined by T- and B-cell levels and improve grip strength (Schiffman and Warwick, 1993)). However, to find an effective plan you will need to know your patient – some will embrace a lunch club whereas others will reel in horror.
Some parts of the GI tract age worse than others
The areas at greatest risk of ageing-related dysfunction are the upper GI tract, particularly the oropharynx and oesophagus, and the distal tract (colon and rectum). After midlife, swallowing and defaecation are, in practical terms, the two functions most likely to be affected.
Oral health is often poor
Deteriorating dentition (in a generation too old to have enjoyed the benefits of fluoride toothpaste) means many live with, at best, dentures and, more often, poor oral function and pain which disrupts nutrition. About 1-in-3 people over the age of 65 years are troubled by a dry mouth or xerostomi (Turner and Ship, 2007) which can cause problems with eating and nutrition, impaired immune defences, difficulty with communication, and discomfort that impairs quality of life. However, poor saliva production is not a normal event in growing older. Instead, it is important to be vigilant for causes including systemic diseases such as Sjögren’s syndrome or, more commonly, medications (such as anticholinergic drugs). A proper diagnosis and treatment of underlying cause where possible, is essential. Simple strategies to improve oral hydration, such as ensuring that a palatable drink is always within reach for sipping, as well as salivary replacement therapies can improve both oral health and comfort. However, as with every other dietary habit, finding something that works will be heavily dependent on the patient’s own likes and dislikes.
Swallow may become less reliable
Even if a person is hungry to eat and able to masticate, less efficient swallowing mechanisms, due to muscle weakness, disrupted motility and concurrent disease, increase the risk of aspiration and reflux. Dysphagia, or difficulty swallowing, is a very common problem with ageing, and is usually multifactorial (Shaker and Staff, 2001) due to factors such as poor dentition, slow transfer of the food bolus to the posterior oropharynx, an increase in asynchronous contractions of mylohyoid muscle, delayed closure of the larynx, delayed relaxation of the upper oesophageal sphincter with food reflux into the larynx (Hall, 2002). After review by the speech and language therapist (SALT), a number of tactics can be employed to help, from practising chin tucks during swallowing (which help to protect airway), repetitive head-raising (to develop the upper oesophageal muscles) or simply food thickening (to improve bolus transfer).
The oesophagus is subject to a general decline of motor function with age, leading to impaired transit of food. Abnormal peristalsis is more frequent in those aged 70+ (Ferriolli et al., 1998) and is aggravated by gastro oesophageal reflux disease (GORD). The oesophageal wall becomes less flexible in older people, and therefore it is probably less able to compensate for additional caustic injury. Hiatus hernia is also more common – more than 60% of those over 60 years in age have a hiatus hernia that tends to increase in size with age. GORD may play a part too, by compromising the competency of the gastro oesophageal (GO) sphincter (Wo, 2008).
Gastric changes are important
Important changes in the stomach include modest slowing of gastric emptying with a resultant prolonged exposure of small intestine to nutrients that can contribute to a physiological reduction in appetite. Meanwhile the capacity of gastric mucosa to resist damage may fall, due to reduced blood flow and a reduction in the production of prostaglandin, glutathione, bicarbonate, and mucus, leading to a steep increase in peptic ulcer disease in later life (Singhal and Bowling, 2000). The incidence of upper GI events such as peptic ulcer or haematemesis rises from 1.6/1000 person years to 6.96/1000 after the age of 90 years (Hippisley-Cox et al., 2005), which serves as a reminder of the dangers of drugs such as non-steroidal anti-inflammatory drugs (NSAIDs) in this age group. In others a fall in gastric acid secretion may result from atrophic gastritis – an endpoint of chronic inflammation secondary to Helicobacter Pylori infection or autoimmune disease. Reduced secretion of gastric acid, intrinsic factor and pepsin then reduces the absorption of vitamin B6, B12, folate, iron and calcium.
In the small intestine, there are no major changes in motility, transit, permeability or absorption in the healthy, but calcium absorption may be reduced by intestinal resistance to 1, 25-dihydroxyvitamin D (Pattanaungkul et al., 2000).
… to issues at the bottom end of the GI tract
The list of lower GI problems that become more common in later life is lengthy and includes: constipation, diverticular disease, haemorrhoids, anal fissures, colonic polyps and cancer, volvulus, ileus, and ischaemic colitis.
Less than 1% of people in the UK report fewer than three bowel movements per week (the Rome criteria for constipation) although a recent review exploring prevalence worldwide suggested a median frequency of constipation in 16% of the adult population (Mugie et al., 2011). However, among the oldest-old constipation is almost normal, affecting nearly 1-in-2 people aged over 80 years (Gandell et al., 2013).
Many theories have been proposed to explain constipation from an older perspective, from dietary changes to autonomic neuropathy, and disorders of both the enteric nervous system and neuroendocrine system. The ability of the bowel to empty may be hampered by an increased thickness of the internal anal sphincter (possibly in compensation for age-related thinning of the external anal sphincter) and a reduction in rectal pressure maximal squeeze pressure (Hall, 2002). Pelvic floor laxity also plays a part, especially in women.
Loss of faecal continence is a significant cause of distress in late life, and is associated with increasing age, long-term illness, mobility problems, GI disease including several of those described below as causes of diarrhoea, and urinary incontinence. A postal survey in the UK of around 16 000 over-40-year-olds showed about 6% of responders had some leakage, whereas major leakage (several times a month and soiling) troubled 1.4%, and disabling faecal incontinence affected 0.7% (Perry et al., 2002). However, in my experience among older patients, it is a topic people find hard to raise. Sometimes it is easier to gauge the extent of the problem by talking to the person who does the laundry than the patients themselves.
There is also a significant change in the gut microbiota in later life, with reduced diversity of organisms, and carriage of certain important commensal species such as bacteroides, bifidobacteria and lactobacilli, while opportunistic pathogens including enterobacteria, Clostridium perfringens and Clostridium difficile are increased in elderly people (Nagpal et al., 2018). The full implications of these changes have yet to be established, but they are likely to play an important part in the development of disease and frailty. As such, approaches that encourage a healthy gut microbiota, such as a very varied diet incorporating many unprocessed foods and prebiotic fibres may play a role in preventing problems ranging from constipation to infection and cognitive decline. We eagerly await the results of research.
However, in later life the GI tract is often not to blame for constipation
Despite efforts to explain constipation as a failure of the GI system, contributing factors unrelated to the physiology of the bowel itself are often to blame in older people. These may include changes in diet, especially a decrease in fibre intake, reduced fluid intake, diminished activity, impaired mobility (most bedridden patients are constipated and need proactive management), social factors, anxiety and depression, and especially medication, e.g. opiates; drugs with anticholinergic side effects such as neuroleptics, antihistamines; medications for Parkinson’s disease; tricyclic antidepressants; and drugs that impair calcium signalling, such as calcium channel antagonists. Attending to this soup of problems may do more for constipation than trying medication that tinkers with the gut itself.
Meanwhile patients themselves often have the possibility of a cancer at the back of their mind when discussing GI symptoms, even if they do not verbalise this fear. Although this is an important consideration that needs to be explored, initial care to discuss all the other possible contributing factors and, if indicated and the patient agrees, trying strategies such as dietary change may be better than jumping straight to referral to secondary care on the 2-week rule. Timely follow-up is critical though when there is a risk of malignancy.
…and diarrhoea is not so often due to infection
While considering causative factors, it is also important to remember that loose motions or diarrhoea is much less likely to be caused by infection than in younger adults. Diarrhoea may be secretory (actually mostly due to reduced fluid and electrolyte reabsorption than net secretion by gut, due to inhibition of reabsorption, rapid motility, bile acid malabsorption, microscopic colitis or drugs), osmotic, inflammatory, fatty (steatorrhoea) or pseudo-diarrhoea. Acute symptoms versus more chronic ones may be a clue, so after a check for an acute gastroenteritis or food poisoning, scrutinise medications, think motility disorders, diabetic neuropathy, irritable bowel syndrome, small bowel bacterial overgrowth, overflow constipation (which we see frequently in the hospital) endocrine problems (such as hyperthyroidism or Addison’s disease), cancers (including carcinoid), and vasculitis. Microscopic colitis encompassing collagenous colitis and lymphocytic colitis is increasingly recognised as a common cause of chronic diarrhea, especially in older women. Even so, older people do get gastroenteritis and although the usual pathogens are found, the risk of hospitalisation is four times higher than average for individuals aged over 75 years.
Among older people in residential or nursing homes, infectious causes become more significant, Bear in mind C.difficile infection, which is more common and spread more easily in an institutional setting (relapses are also more common in the elderly).
Symptoms in older people may be atypical or absent
A common mantra in working with older people is that the textbook symptoms and signs of many conditions may not be seen. The often-used example is fever and infection. The inflammatory response to sepsis may be very weak, and pyrexia absent, despite major infection. There may be a significant diminution of the acute response to GI inflammation and/or perforation. Increased confusion and fatigue may be the only signs of peritonitis, with traditional signs such as guarding or rigidity being absent. As a result, up to two thirds of initial emergency diagnoses of abdominal problems in this age group are found subsequently to be incorrect (Hall, 2002).
There are many other situations where textbook symptoms and signs cannot be found. Red flags are just as vital to spot in older adults, but often the flag may just be a tinge of pink, or not even waving.
Other conditions increasingly throw spanners into the creaking works
The shopping basket of co-morbidities we collect with age frequently add to the burden of GI problems, compound the physiological changes related to ageing, and drug treatments then have further consequences (see the next point). In the UK, around 50% of those over 65 years have two or more long-term conditions, and many of these can impact on GI function.
Careful thinking around co-morbidities and analysis of root causes of symptoms is vital in effective management. A myriad of diseases can impair smell and taste for example, including Alzheimer’s disease (which also reduces thirst or simply the motivation to eat or drink), epilepsy, head trauma, Parkinson’s disease (where olfactory impairment is increasingly recognised as an early symptom), cancer and its treatment, sinusitis, nasal polyps, hypothyroidism, diabetes and many other endocrine problems.
Bowel diaries can be extremely useful to pinpoint complex interactions, but often the issue is simple. For example, osteoarthritis may limit mobility and restrict a person’s ability to respond to the call to the toilet. Treating pain and stiffness effectively may be the key to improving incontinence (although of course, opiate painkillers often bring their own GI hazards).
However, teasing out the underlying causes of GI symptoms, and how they should be managed, is complex. Problems are often dynamic, fluctuating in time and with the state of other co-morbidities, and rarely answered by a single strategy.
And medicines, drugs, tablets and tinctures add grit to the grind
Some examples of common GI side effects from medication.

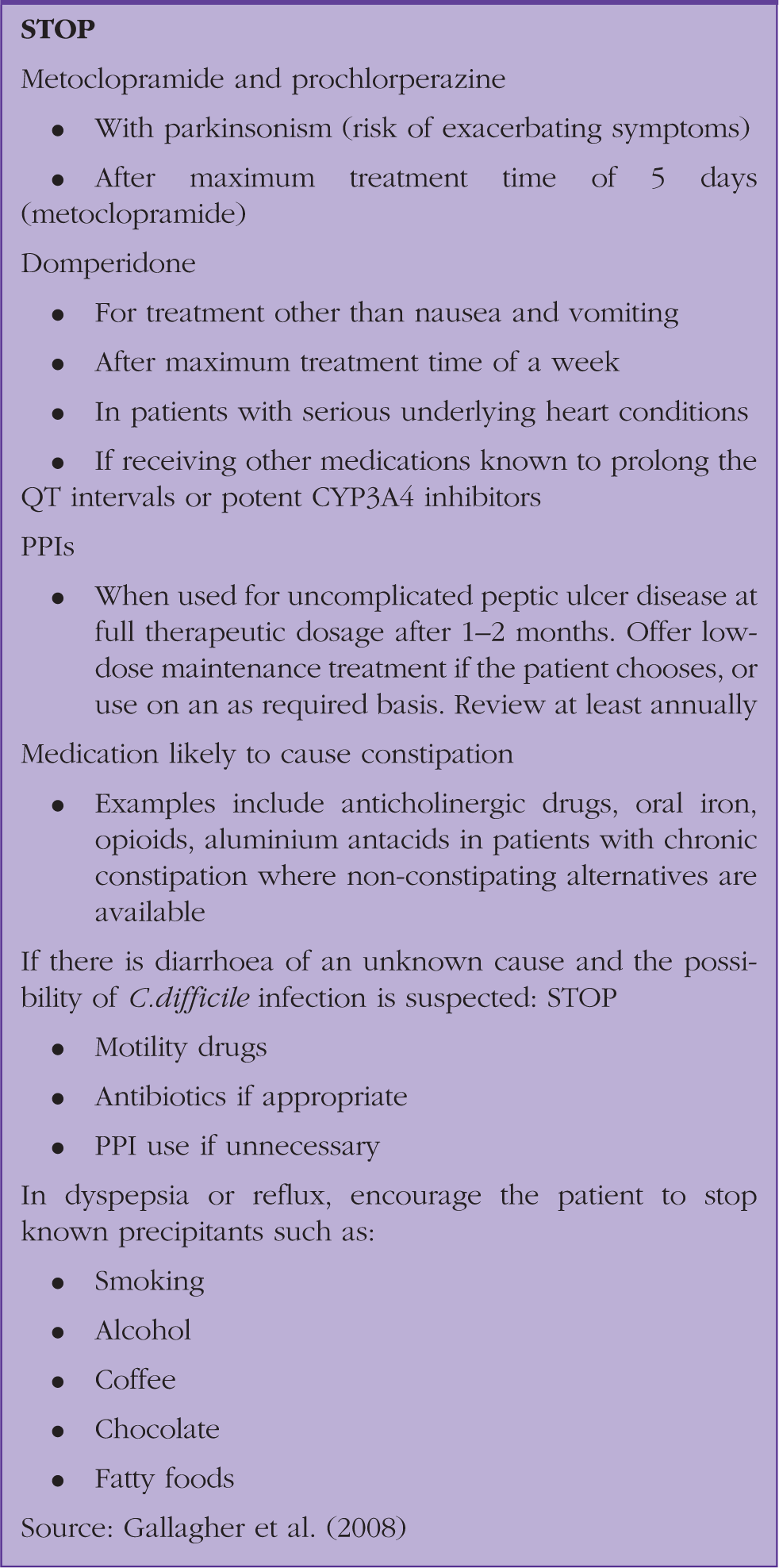
Examples of when to consider stopping particular medication being used for GI disease in older patients.
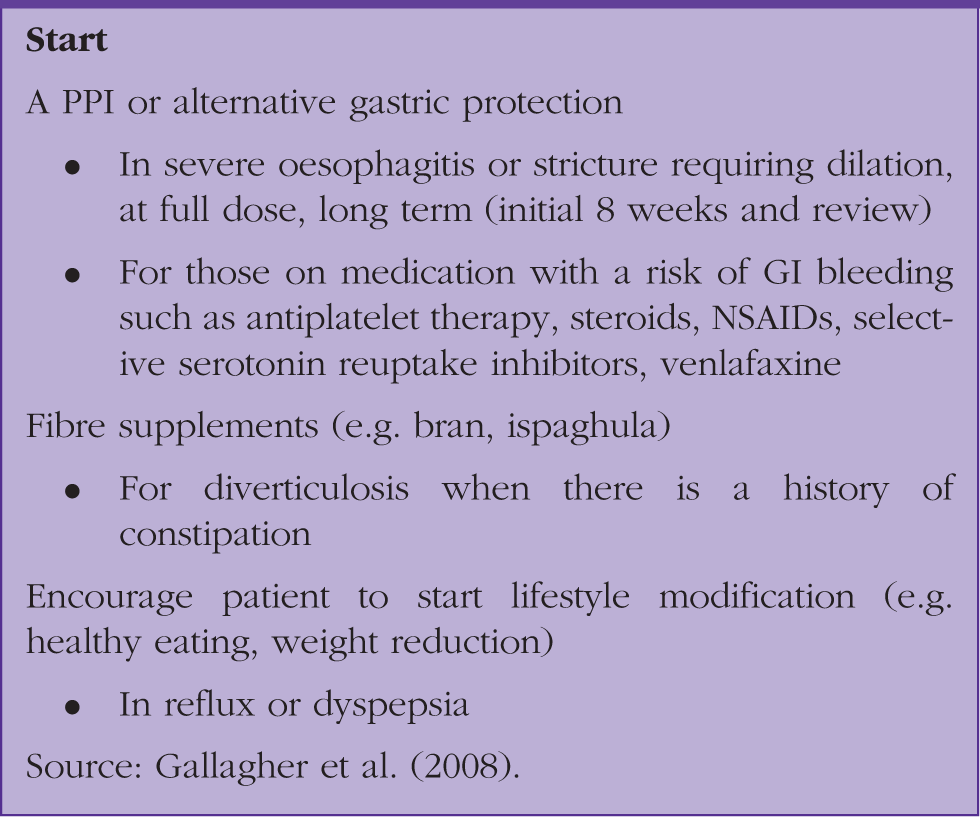
Examples of advice about what to consider starting in the management of GI disease in those over 65 years in age.
KEY POINTS
In the absence of GI disease, GI physiology can remain fairly predictable until well into the ninth decade of life; however, many common co-morbidities interfere with GI function much earlier GI habits are highly individual and subjective; what matters most is change from the usual Many diseases that become more common with age can affect gut function Most drugs and medicines have GI side effects, which are often relevant in older patients Social and psychological factors play an increasing part in digestive health as the years pass Use the STOPP START Tool to review both prescribed and over-the-counter medicines, and do not forget herbal or complementary remedies