
Abstract
Musculoskeletal pain is a common presentation in primary care. Although septic arthritis is a rare cause of joint pain, expeditious diagnosis and treatment is of paramount importance to avoid the local destruction of intra-articular cartilage and sepsis. In this article risk factors, pathology, presentation, referral and treatment of suspected septic arthritis are explained, to help GPs identify and manage this potentially life-threatening condition.
Pathogenesis
There are several routes via which pathogens can enter the normally sterile joint environment:
Haematogenous spread can occur in patients with a systemic bacteraemia. In both native and prosthetic joints, bacterial seeding can occur across the highly vascularised joint synovium resulting in joint inflammation and septic arthritis (Sreenivas et al., 2013) Direct inoculation of the joint can result from penetrating trauma Iatrogenic, due to either joint injection or surgery Local bacterial spread can occur either from areas of adjacent osteomyelitis or from cellulitis overlying the joint
Following joint colonisation, bacteria undergo rapid proliferation and trigger an acute inflammatory response. This protective immunological response aims to eradicate the infective pathogens via macrophage- mediated bacterial phagocytosis. Cytokines involved in this inflammatory process cause matrix metalloproteases and other proteolytic enzymes to be released; resulting in chondrolysis of articular cartilage (Shirtliff and Mader, 2002). In addition, synovial hyperaemia and increased production of synovial fluid causes a joint effusion. The resulting rise in articular hydrostatic pressure causes direct cartilage degeneration (Sreenivas et al., 2013).
Risk factors
Septic arthritis is relatively rare, with an incidence of between 2 and 10 per 100 000 (Goldberg, 1998). It is more prevalent at extremes of age, and in those with diabetes, renal failure, hepatic failure and human immunodeficiency virus.
The association between rheumatoid arthritis (RA) and septic arthritis is well recognised, but the exact underlying pathogenesis is debated. Patients with RA also have several iatrogenic risk factors, including systemic immunosuppressive medications, and often receive intra-articular steroid injections (Wang and Tambyah, 2015). Gout, the most common crystal arthropathy, has also been linked to an increased susceptibility to septic arthritis (Lim et al., 2015). In patients with RA, gout, and indeed osteoarthritis, there is often a delay in the diagnosis of septic arthritis, as symptoms may be attributed to the pre-existing musculoskeletal pathology.
Although rare, septic arthritis is a recognised complication of orthopaedic surgery, but remains most concerning after joint replacement, where prosthetic joint infection is associated with significant morbidity and mortality (Chew et al., 2015). Substance abuse also increases the risk of septic arthritis; particularly in intravenous drug use where immunodeficiency and haematogenous spread of infection is common.
Microbiology
Septic arthritis is typically caused by bacteria, although rarely it can be caused by a fungal or viral infection. An understanding of the most common causative organisms is important in targeting early empirical treatment. Although there are an extensive number of bacterial causes, there are common organisms linked to patient age and specific patient cohorts.
Staphylococcus aureus is a prevalent skin flora and is recognised as the most common causative organism in septic arthritis (Jung et al., 2018). Methicillin-Resistant Staphylococcus aureus (MRSA) is a rare cause of septic arthritis, but must be considered in patients in both the hospital and nursing home settings, and in intra-venous drug users. Streptococci are more commonly isolated in patients who are immunocompromised, have chronic skin ulcers or long-standing dermatological conditions. Gram negative organisms, such as Escherichia Coli and Pseudomonas aeruginosa, are most prevalent in the elderly and in immunosuppressed patients (Shirtliff and Mader, 2002). Neisseria Gonorrhoea must be considered in the sexually active patient.
The most common causative organisms in children are similar to those in the adult population, but not the same. Haemophilus influenza has declined as a cause in this age group, thanks to vaccination programmes. After S. aureus, in order of decreasing prevalence, the common organisms in the paediatric population are MRSA, Streptococcus pneumonia, Streptococcus Pyogenes and Group B Streptococcus (Goergens et al., 2005).
Presentation
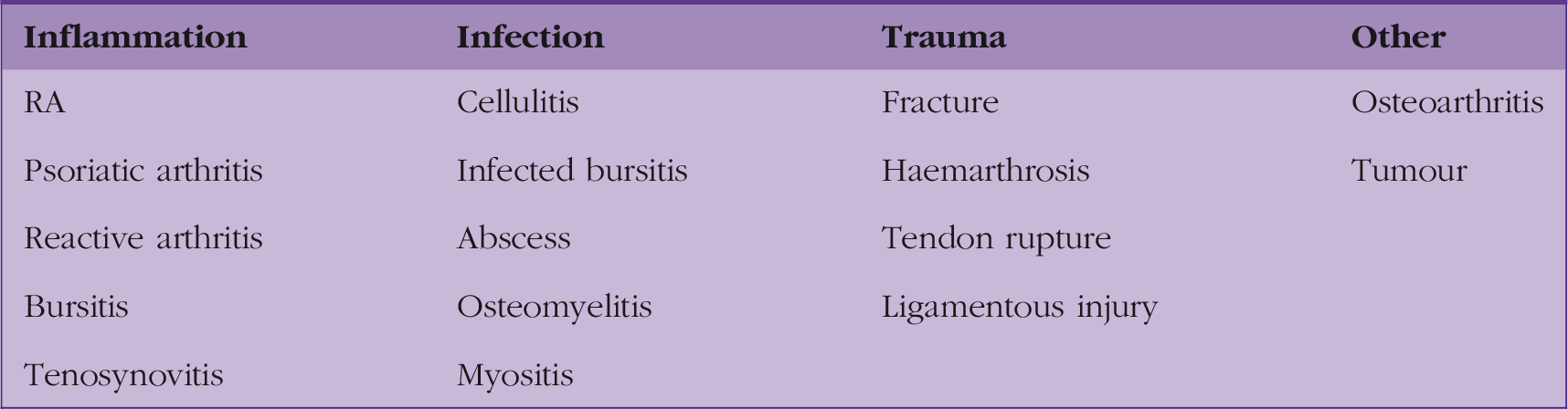
Differential diagnosis for joint pain.
The vast majority of septic arthritis is mono-articular. In the adult, it most commonly affects (Lauper et al., 2018): the knee (33%), followed by the shoulder (24%), inter-digital joints of the hand or foot (23%), and the hip (11%).
History
Presenting symptoms include: Joint pain, effusion, erythema, an increased joint temperature, a reduced range of movement, and systemic symptoms of infection. It is important to elicit the onset and duration of symptoms, including any preceding systemic symptoms of infection, recent surgery or joint injections, and any history of acute or long-standing skin wounds. Pain is usually progressive, and is associated with systemic symptoms of sepsis in approximately 30% of patients at diagnosis (Jung et al., 2018). In individuals with pre-existing joint disease, attention should be paid to acute worsening of chronic symptoms.
Any risk factors should be identified in the past medical history and medication list. Alcohol intake and smoking status should also be documented.
Examination
As the patient walks into the consulting room, note that an inability to weight-bear or a new antalgic gait pattern should increase the suspicion of a septic joint. When examining the patient, take a full set of observations: tachycardia and pyrexia should raise the clinical suspicion of a septic arthritis, although patients with a septic arthritis often have normal observations on presentation.
Before examining the affected joint, obtain adequate exposure of the joint above and below. Inspect for signs of an effusion, erythema, surgical scars and skin wounds, comparing with the contralateral side.
On palpation the joint will typically be warm compared with the contralateral side. Check for a joint effusion, which is often tense in septic arthritis. A reduction from the patient’s usual range of movement is often of key importance in the differentiation of septic arthritis from other causes of joint pain.
Investigations
In adults there is no widely used validated scoring system to accurately help identify individuals with septic arthritis. Diagnosis should combine the full clinical picture, taking into account: patient risk factors, the clinical presentation, examination findings and results of appropriate investigations. In primary care, if there is a clinical suspicion of septic arthritis the patient should be referred as an emergency for assessment in secondary care.
Blood tests performed in secondary care should include the inflammatory markers of white cell count (WCC), C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), radiological assessment, joint aspiration and blood cultures. CRP and ESR are typically raised in septic arthritis, but these acute phase reactants can be elevated in any inflammatory condition. A high WCC is often present in septic arthritis, but the diagnostic predictive value of serum tests is poor with widespread heterogeneity of both sensitivity and specificity reported in the literature (Carpenter et al., 2011). Normal inflammatory markers do not exclude a septic arthritis, and serum markers should not be used alone in diagnosis of septic arthritis. Although serum urate is often performed when investigating a swollen joint, it is important to note that evidence shows no diagnostic value of serum urate levels in acute gout or sepsis (Coakley et al., 2006).
Plain radiographs are useful in identifying other differential causes of joint pain, such as intra-articular fracture, osteomyelitis and tumour. However, they are of limited value in reliably delineating between septic arthritis and other degenerative joint disease. In septic arthritis magnetic resonance imaging features correlate with septic arthritis, but are most often utilised to rule out osteomyelitis or investigate for other differential diagnoses. Ultrasound can assess for joint effusion but is most advantageous in guiding arthrocentesis as part of the diagnostic workup (Costales and Butler-Wu, 2018).
Arthrocentesis is the gold standard for diagnosing septic arthritis. In the native joint, aspiration should be performed at the earliest possible opportunity and using a strictly aseptic technique. In the prosthetic joint, aspiration must be performed by the orthopaedic team in the sterile operating theatre environment. Aspiration should not be delayed while awaiting serum investigations or in patients on anti-platelet or anticoagulant medication when there is a clinical suspicion of septic arthritis.
Joint aspirate should be inspected for its macroscopic appearance, and then sent for urgent gram stain, cell count and culture. Identifying the infective pathogen with culture and antibiotic sensitivities is the key in guiding targeted antibiotic therapy. Although gram stain is an important part of the clinical picture, the sensitivity of gram stain for diagnosing septic arthritis is low (Carpenter et al., 2011). Common cell count diagnostic criteria quoted are a WBC > 50 000/L and/or >90% neutrophils (Agout et al., 2015). However, there is widespread variation reported in sensitivity and specificity of the WBC in the literature, which questions its value as a diagnostic tool in septic arthritis (Carpenter et al., 2011). Cytology of joint aspirate is useful for ruling out the common differentials of gout and pseudo-gout.
Management
Anyone with suspected septic arthritis should be urgently referred to secondary care for on-the-day review by the orthopaedic team. There are three key principles in the treatment of septic arthritis:
Obtain a joint aspirate for microbiology analysis Reduce the bacterial load of the infected joint Administer empirical antibiotic therapy, then targeted therapy based on microbiology results
Obtaining a joint aspirate before giving antibiotics is of paramount importance. Administering empirical antibiotics prior to diagnostic aspiration significantly decreases the sensitivity of both microscopy and culture in identifying the causative organism (Hindle et al., 2012). Antibiotics administered before joint washout cause diagnostic delay to definitive treatment and increase the complication rate (MacLean et al., 2015).
Reducing the bacterial load of the septic joint is typically performed by surgical washout, but in the elderly co-morbid patient with significant anaesthetic risk, needle aspiration to dryness may be considered. Research comparing the two techniques is limited and based on retrospective studies with small case numbers (Ravindran et al., 2009). Surgical washout can be performed via an arthroscopic or open technique. Typically, arthroscopic washout is utilised in joints more amenable to the arthroscopic technique (e.g. knee, shoulder) compared with open washout (e.g. hip).
Antibiotic therapy should be started empirically and then tailored to the causative organism, based on results of microscopy and culture sensitivities. Broad-spectrum empirical antibiotic cover should be governed by local microbiology guidelines and the most common causative organisms. Common empirical antimicrobial agents include flucloxacillin or second- and third-generation cephalosporins such as cefuroxime (Mathews et al., 2007). Targeted antibiotic therapy and duration of treatment should be tailored to the individual patient, involve specialist microbiology input, and be guided by culture and sensitivity results.
Outcomes after septic arthritis are variable. Systemic sepsis at diagnosis is related to duration of symptoms and is associated with poorer patient outcome (Jung et al., 2018). Delay to surgical treatment and the degree of degeneration seen at initial arthroscopy are both associated with a poorer functional outcome (Yanmis et al., 2011).
Septic arthritis in a child
Over 80% of cases of septic arthritis in children occur in those below the age of 5 years (Agout et al., 2015). Haematogenous spread is more common in children, and particularly in infants where capillaries crossing the epiphyseal growth plate are a direct route for transmission of pathogens into the joint (Shirtliff and Mader, 2002). The two most commonly involved joints in children are the hip and the knee, accounting for two thirds of all paediatric cases of septic arthritis (Goergens et al., 2005).
Joint pain and limp remain the two principal presenting symptoms, but it is not uncommon, particularly in infants, for septic arthritis to present with systemic symptoms alone, such as pyrexia and general malaise. In addition to a limp and pain on passive joint movement, children with hip septic arthritis often hold the leg abducted and externally rotated. This position represents that of maximal intra-articular volume reducing capsular pressure and pain. A child with knee pain may be experiencing referred pain from the hip; hence, the importance of always examining not only the painful joint, but also the joint above and below.
Kocher’s criteria for paediatric septic arthritis.

Prosthetic joint infection
Over 100 000 primary knee arthroplasty and over 90 000 primary hip arthroplasty procedures were performed in the UK in 2017 (National Joint Registry, 2018). Although prosthetic joint infection (PJI) is rare (commonly quoted as between 1 and 2% for primary arthroplasty procedures) it results in significant morbidity and mortality (Chew et al., 2015).
PJI can result from colonisation at the time of procedure, contagious spread from adjacent sites of infection, and haematogenous seeding from systemic bateraemia. It is commonly defined as early onset (less than 3 months), delayed onset (2 to 12 months) and late onset (more than 12 months). Although there are several well-recognised peri-operative factors that influence PJI rates, diabetes, obesity and RA are the most important patient risk factors in lower limb arthroplasty (Tande and Patel, 2014).
Biofilm is an important concept in explaining the challenge faced in treating PJI. After implant colonisation, bacterial adherence to the implant is followed by the formation of an overlying protective extracellular polysaccharide glycocalyx or ‘biofilm’ (Taha et al., 2018). Biofilm walls off bacteria from the host immune system and prevents antibiotic penetration (Shirtliff and Mader, 2002).
In the post-operative period erythema, wound discharge, decrease range of movement, inability to weight-bear and systemic symptoms of infection should raise suspicion of septic arthritis. Late infection, where there is often a decreased host immunological response, can be more challenging to diagnose.
Two-stage revision has long been the gold standard in PJI. This involves initial debridement and hardware removal followed by a period of systemic antibiotic treatment prior to delayed implantation of new arthroplasty components. Chronic antibiotic suppression is a non-surgical treatment option that may be used in elderly patients with advanced co-morbidities at significant surgical and anaesthetic risk.
KEY POINTS
Have a high clinical suspicion of septic arthritis in patients presenting with joint pain, effusion, erythema and a reduced range of movement When septic arthritis is suspected, patients should be urgently referred to hospital for orthopaedic review Empirical antibiotics should not be administered until a joint aspirate is obtained High-risk patients include those with immunosuppression, RA, prosthetic joints and the limping child Diagnosis is based on the combination of clinical history, examination, serum and radiological investigations, but arthrocentesis remains the gold standard Treatment involves prompt surgical washout and appropriate antibiotic therapy, which should be guided by microbiology advice