
Abstract
Anxiety is the physiological state of fear, unease or apprehension experienced by an individual in the face of an uncertain outcome. Anxiety disorders are characterised by recurrent symptoms of anxiety disproportionate to the eliciting situation, and are the most common disorders of emotion among young people in the UK. They have an early onset and increasing prevalence. This article provides a detailed insight into causes, diagnosis and management strategies for the different anxiety disorders in young people within primary care and the wider community.
Causes of anxiety in children and adolescents
Excessive levels of anxiety often interfere with a young person’s daily life and mental wellbeing. Although family aggregation and genetic studies suggest a vulnerability to anxiety in children of individuals with anxiety (Murray et al., 2009), a range of other predisposing environmental and health factors have been identified.
Environmental factors are significant in the development and maintenance of anxiety. Traumatic or ongoing stressful life events affect a child’s wellbeing, increasing vulnerability to anxiety and other mental health difficulties. Learning and mimicking of parental anxiety-related behaviours, social interactions, and maladaptive coping strategies by children have been reported (Eley et al., 2015). Commonly identified triggers of anxiety include experience of abuse, neglect, traumatic injuries, bereavement, overprotective or anxious parenting, witnessing domestic violence, alcoholism or frequent arguments at home, or community/school-related issues (exam pressure, bullying).
Anxiety commonly occurs alongside or secondary to other mental and physical health disorders. Young people with physical health disorders are significantly more likely to develop anxiety than peers, with lifetime prevalence as high as 40% (Balázs et al., 2018). Clinically significant symptoms of anxiety have been reported in between 30 and 40% of children with attention deficit hyperactivity disorder (ADHD) or autistic spectrum disorder (Van Steensel et al., 2011). Comorbid anxiety is often unrecognised in young people, and has a poorer response to treatment.
Different types of anxiety in children
A number of anxiety disorders have been described in children and adolescents. Symptoms depend on the individual, their age, stage of development, life experiences and circumstances. A summary of common disorders follows.
Generalised anxiety disorder
Generalised anxiety disorder (GAD) is characterised by persistent and excessive worry about multiple topics. Sufferers experience feelings of severe worry and tension, often without provocation. Excessive worry about everyday activities and anticipation of disaster are common.
Separation anxiety disorder
Separation anxiety disorder is an excessive fear or anxiety concerning separation from home, parents or caregivers, exceeding what would be expected at the child’s developmental level. Separation anxiety is a normal stage of development for infants and toddlers, only becoming clinically relevant when persisting beyond the age of 3 years (NHS, 2019). School refusal is common in separation anxiety, with poor school attendance negatively impacting on academic performance.
Selective mutism
In selective mutism, the child feels unable to speak in specific social situations or to certain people as a means of self-protection during intense anxiety. This physical inability to speak in certain social settings is frequently misunderstood to be a conscious decision. More than 90% of children with selective mutism also have social phobia or social anxiety (Shipon-Blum, 2019).
Social anxiety disorder
Children with social anxiety disorder have an irrational fear of engaging in social activities, triggered by perceived or actual scrutiny from others. Social anxiety disorder can lead to avoidance and withdrawal from specific, or in extreme cases, any form of social interaction. Childhood symptoms can include: a lack of eye contact, clinging to parents, hiding or running away, crying, immobility, emotional outbursts or significant anxiety at public exposure, for example eating in public, having photographs or videos taken, using public toilets (Beidel et al., 1999).
Obsessive–compulsive disorder
Obsessions are unwanted, persistent and intrusive thoughts, urges, or images commonly causing significant anxiety or distress. Often there are efforts to ignore, suppress, or cancel obsessions with another thought or action. Compulsions are repetitive behaviours or mental acts that the child feels driven to perform in response to an obsession or rules that must be applied rigidly. Insight into symptoms will vary by age. Although the child may be aware that their behaviour is irrational, they struggle to control their obsessive–compulsive tendencies.
Panic disorder
Panic disorder is characterised by recurrent spontaneous panic attacks, with or without reason. Episodes can last from seconds to hours. Symptoms may include feelings of sudden and intense anxiety, an increase in heart rate, chest pain, shortness of breath, weakness, dizziness, shaking, nausea and dry mouth.
Phobias
Phobias manifest themselves through exaggerated, irrational fear and distress brought on by specific objects or situations. Childhood phobias can be specific in focus and have a trigger event, for example animals, insects, blood, heights, closed spaces, or flying. Complex phobias, such as agoraphobia, often have a less easily identified cause. The distress associated with the phobia and the need to avoid the trigger can significantly affect a child’s mental health.
Assessment
Anxiety
Young people with anxiety may present to primary care with a parent/carer, friend, or independently. Assessment for a potential anxiety disorder will depend on the age and developmental stage of the young person. Consultations need to be sensitive, non-judgemental, and allow time to build rapport. Spending time with the parent(s) and young person separately may help the young person to share how they are feeling. Use of effective communications skills is essential, for example, with open questions, relatable examples, avoidance of medical terms and non-verbal cues. Symptoms assessment scores such as the open access Revised Children’s Anxiety and Depression Scale may support diagnosis and can be completed by the young person in the waiting room (Child Outcomes Research Consortium, 2019). Numerical or pictorial Likert scales may help young people to express degrees of pain, happiness and the impact of symptoms. It is important to consider the potential for anxiety disorders in young people with another chronic mental or physical health condition. Topics to explore when assessing anxiety should include:
The nature of symptoms Symptom severity and perceived impact Exacerbating and relieving factors (including screen time and social media) The home, school and social situation What support and treatments have been or would be acceptable Which, if any, support services have already been accessed Any warning signs for abuse, exploitation, substance misuse, self-harm and suicidal ideation
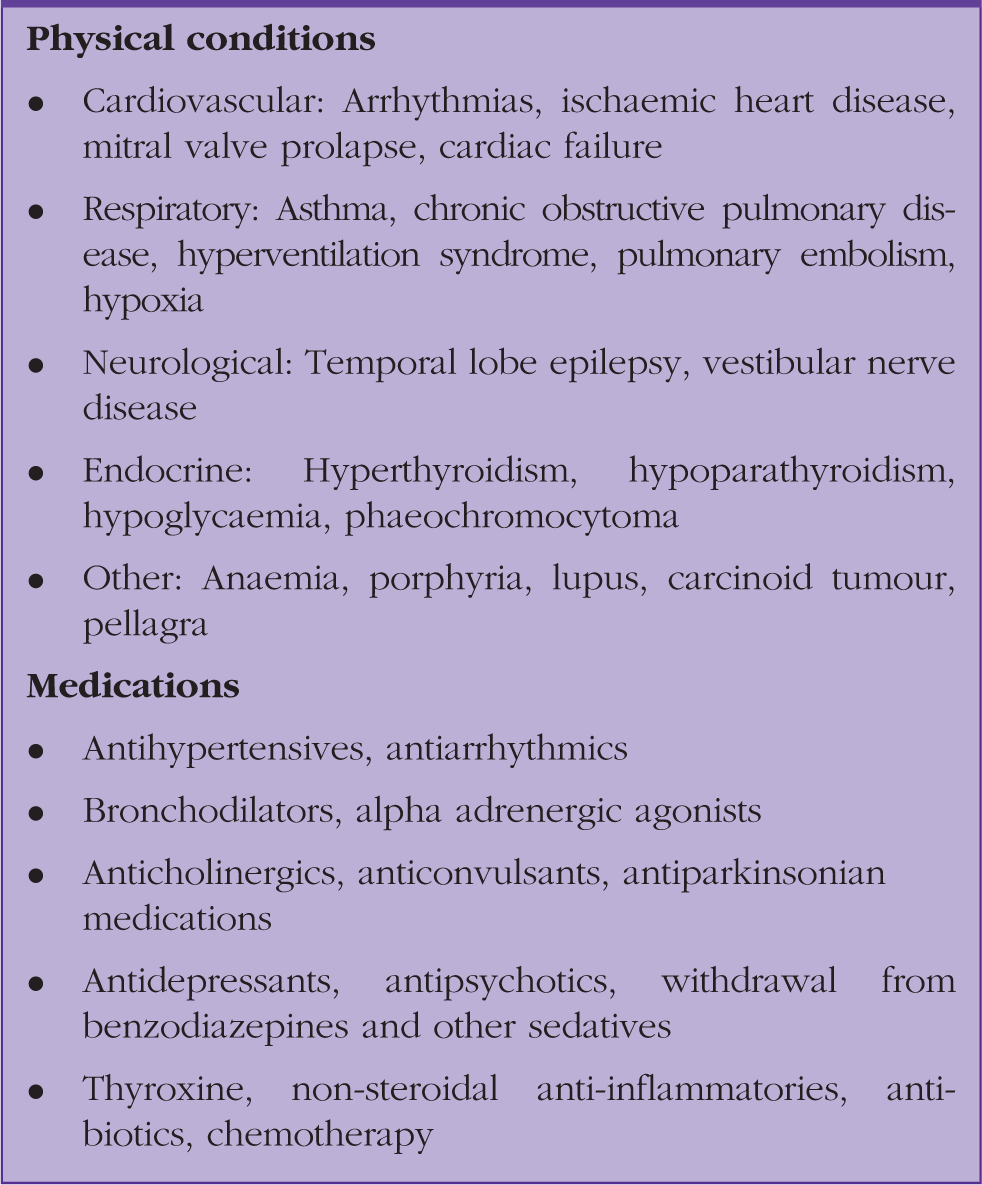
Differential diagnoses
Differential diagnoses for symptoms and triggers of anxiety in young people.
Safeguarding
Exposure to maltreatment during childhood, including abuse and neglect, increases the risk of developing a mental health disorder (Semple and Smyth, 2013). There is a strong association between emotional abuse, difficulties with emotion regulation and development of anxiety (Bruce et al., 2012). Primary care often allows an insight into the family, social, and home environment of a young person. Discussing topics relating to safeguarding can be a challenge, and it will often require a relationship of trust to be built prior to disclosure. National Institute for Health and Care Excellence (NICE) clinical guideline CG89 describes steps to screen young people for abuse, neglect, and sexual or other exploitation (NICE, 2009). Any cases of safeguarding concern should be reported to the local safeguarding lead, with potential escalation as appropriate to ensure that the young person under consideration, and any other young or vulnerable people living with them, remains safe.
Management
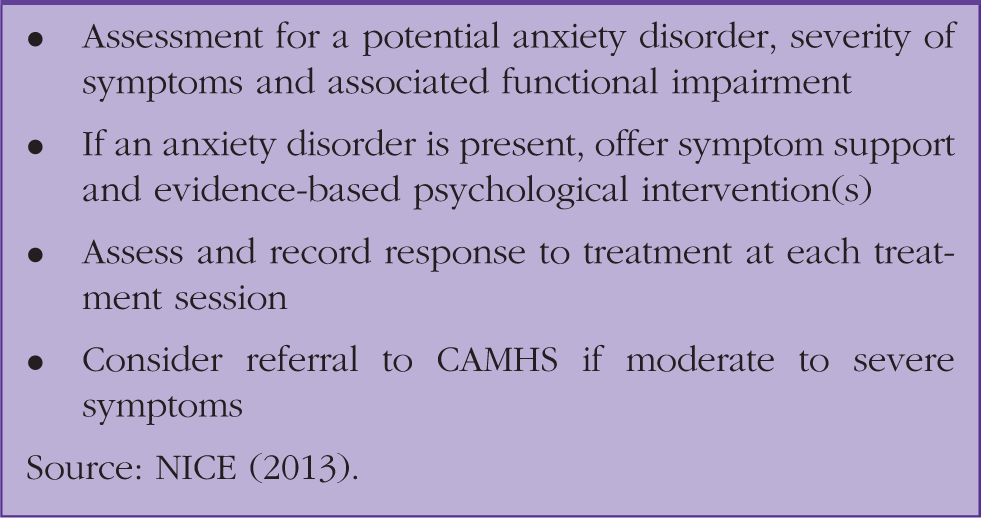
A summary of the management of young people with anxiety.
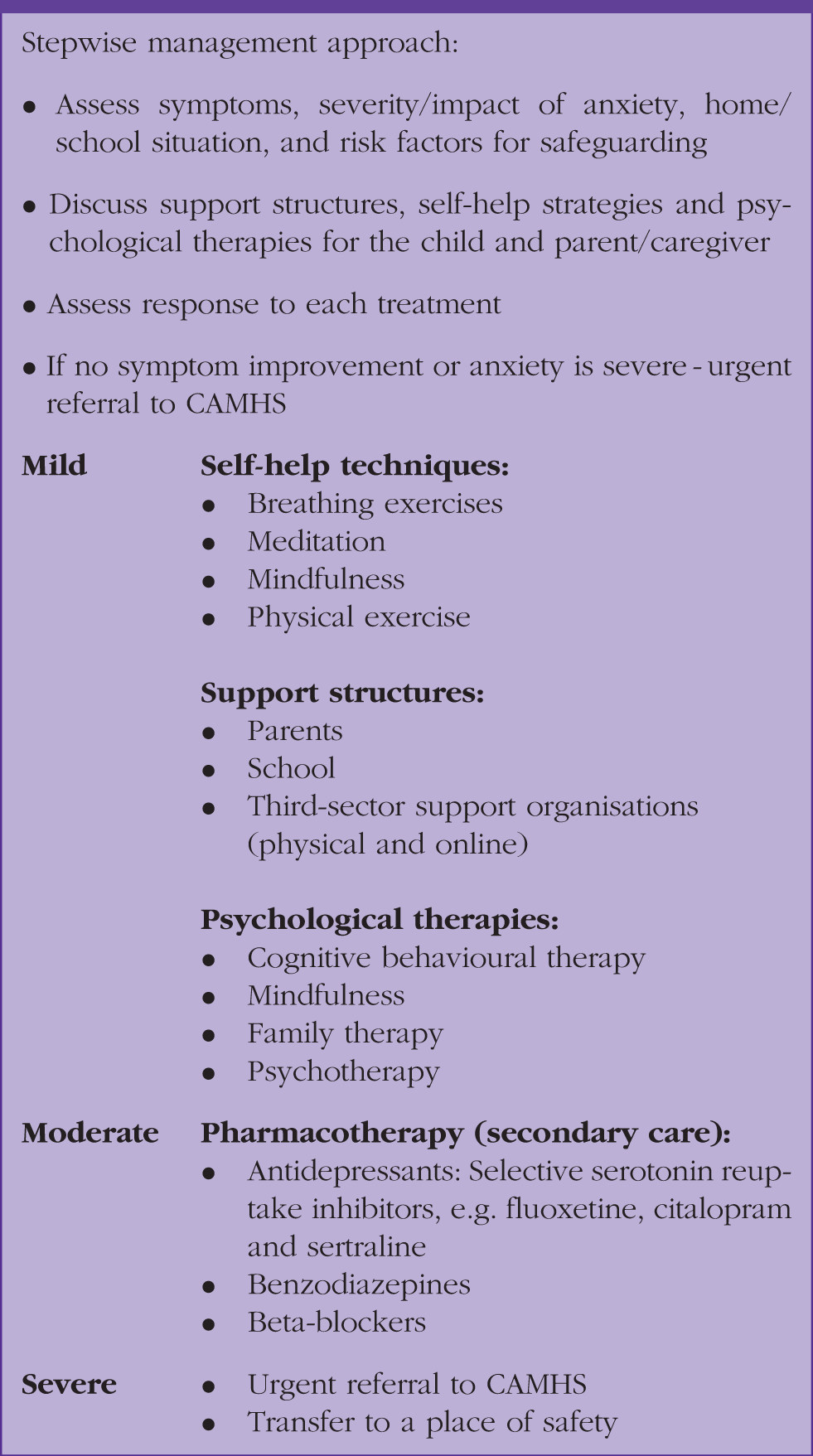
Stepwise management of a suspected anxiety disorder based on NICE guidelines.
Self-help techniques
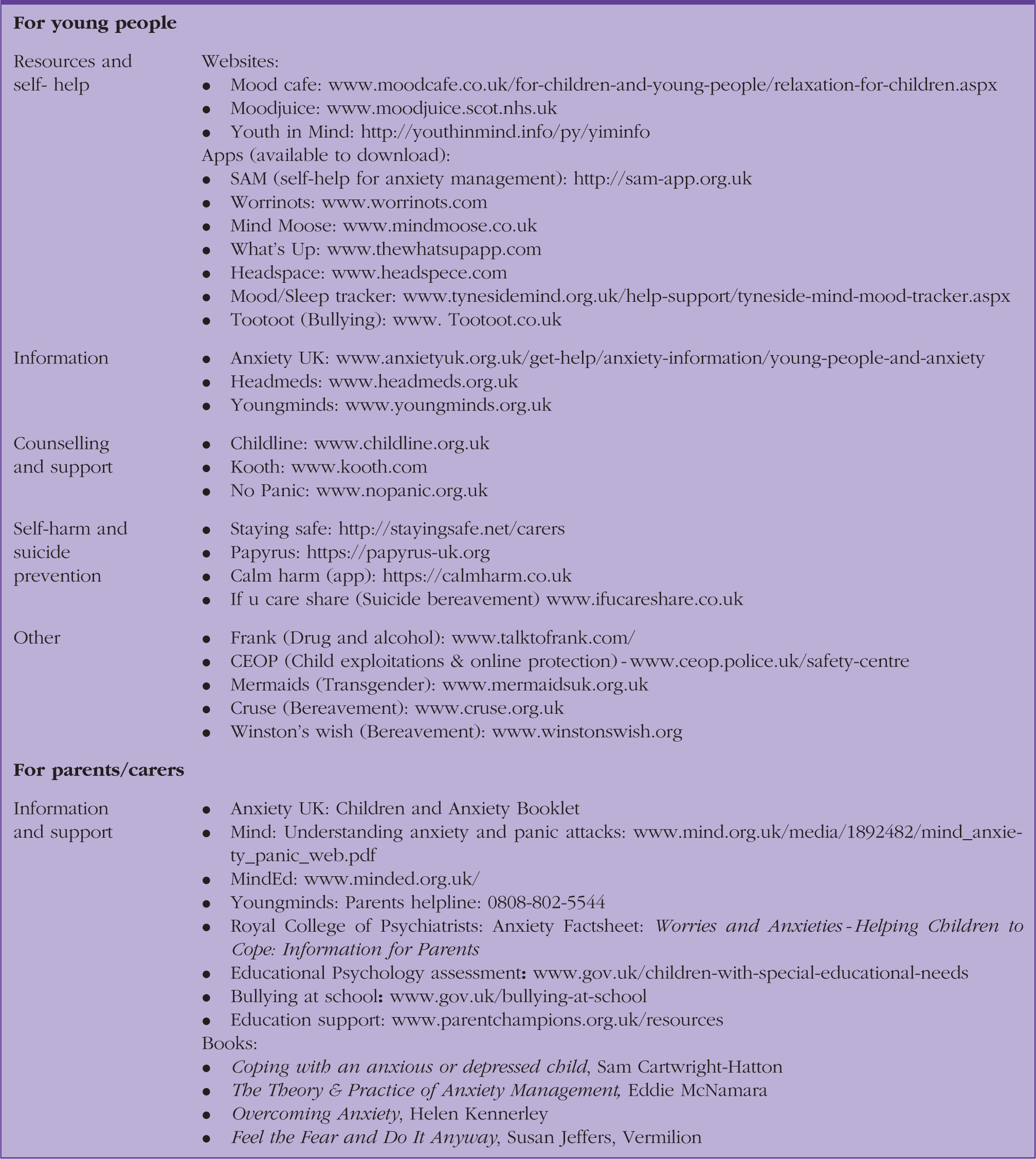
Anxiety management resources and support for young people and their parents.
Parents and caregivers can have a significant impact on symptoms and burden of anxiety. Parent–child interventions are thought to be more effective than individual and group child-focused CBT applied to cases of anxiety (Brendel and Maynard, 2014). Parental involvement in promoting self-help techniques and resources, pastoral strategies at school and seeking appropriate professional support can improve the efficacy of interventions. Signposting parents and caregivers with anxiety or other mental/physical health conditions to appropriate support and treatment providers may help parental engagement and reduce home stressors experienced by the child. In cases where co-diagnosis with autism or ADHD is suspected, parents can consider contacting their local Parent Partnership, a statutory agency which provides assistance in obtaining an educational psychology assessment and implementing advice. Parents of children with significant needs may approach the local authority and apply for additional help including Special Educational Needs support (UK Government, 2019a).
Multi-professional networks
Children are part of a wider community including local family, schools, community organisations, and health and social care. Such organisations may be able to provide specific support for young people suffering with anxiety, in addition to practical support relating to traumatic life events, family crises, bereavement, divorce, bullying or exam stress.
Although dependent on the available resources within a school, young people with anxiety may be eligible for tailored support or adaptations. Any contact with a young person’s school requires consent from either their parent(s) (age < 16 years) or the young person (age ≥ 16 years). Potential examples of support include: warnings before major changes; preferential seating; clear expectations; pastoral meetings; trigger minimisation (e.g. not reading aloud or filming presentations); ‘time out’ passes to leave the classroom; and timetable changes. Additional support during exacerbations or after a school absence can be provided through provision of class notes and limiting the burden of missed homework or assignments. All schools are required to address instances of bullying in line with the ‘Anti-Bullying Act’ (UK Government, 2019b). Developing an effective strategy to manage anxiety at school can take time and may require regular review meetings between the young person, parent(s) and their educational team. Informing the school of secondary care and service involvement can help direct such strategies.
A number of third-sector organisations provide support for young people with anxiety and their parent(s) (see Table 2). Support organisations for specific physical or mental health conditions also provide support for individuals with concomitant anxiety, for example The National Autistic Society and the ADHD Foundation.
Psychological treatments
Psychological
NICE (2013) recommends consideration of psychological therapies as first-line treatment for children and adolescents suffering with an anxiety disorder. This are most commonly provided through CAMHS and third-sector organisations.
Cognitive behavioural therapy
CBT works to help children identify and change problematic thinking styles or behaviour patterns. Children are taught to employ strategies to challenge and overcome distorted thoughts and destructive patterns of behaviour resulting from negative thinking patterns. CBT tailored to children is efficacious for mood and anxiety symptoms, with benefit exceeding that of medication (Hofmann et al., 2012).
Mindfulness
Mindfulness involves focusing on difficult thoughts and feeling, rather than avoiding them, so that the fear gradually lessens. This often entails meditation, yoga and breathing exercises. Mindfulness is often combined with CBT.
Family therapy
Family therapy involves the whole family undergoing counselling with a family therapist to identify and resolve any issues they are collectively facing. Improved parent–child communication is also encouraged.
Psychotherapy
Psychotherapy is a long-term therapy where the impact of past events is discussed in an attempt to ameliorate their long-term effects. Psychotherapy should be reserved for those children with a relatively good prognosis, reserving more intensive treatments for those who do not respond to the first-line treatment and those whose prognostic profile indicates that they require more input.
Pharmacological treatments
The routine prescription of pharmacological treatments for anxiety in children and adolescents is not recommended within primary care. Pharmacotherapy is prescribed within secondary care in cases of moderate to severe anxiety. Primary care may, however, be responsible for monitoring and review of young people commenced on licensed medications.
Selective Serotonin Reuptake Inhibitors (SSRIs), e.g. fluoxetine, citalopram and sertraline, are prescribed for moderate to severe anxiety in children and adolescents. Close monitoring is required because of an increased risk of suicide.
Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs), e.g. duloxetine and venlafaxine, are sometimes prescribed to adolescents with anxiety.
Benzodiazepines are occasionally commenced in secondary care for young people with acute anxiety as a short-term treatment for immediate symptom relief. The risks of benzodiazepines, including tolerance, abuse, and dependence, are similar to adults, with cessation risking withdrawal symptoms and seizures.
Beta-blockers (e.g. propranolol) can provide short-acting relief of physical symptoms of anxiety, such as palpitations and tremors. Similar to benzodiazepines, they are not recommended for long-term use in children or adolescents.
Referral to CAMHS
Urgent referral to CAMHS should be considered in cases of anxiety felt to be severe or associated with self-harm, suicidal ideation, or attempted suicide. Given the high level of clinical demand faced by CAMHS, it is important that any ‘non-urgent’ cases are directed towards guided self-management and community support services prior to consideration of CAMHS referral. Ideally referrals should include information of any service access, outcomes from educational psychology reports and symptom assessment scores.
Screen time and social media
Screen time, media and social media usage is high among many young people. Although increased rates of anxiety, depression and sleeping difficulties have been reported in frequent users (Roal Society of Public Health, 2017), protective benefits including distraction, connecting peers and building social networks have also been described (Morgan and Jorm, 2008).
Anxiety in children and adolescents secondary to media exposure is not a recent phenomenon, with anxiety-induced sleep disturbance and trauma-like symptoms reported after viewing age-inappropriate television and online content. Social media often presents attractive individuals living idealised lives. Resultant comparison, negative self-evaluation and personal dissatisfaction have been noted in children and adolescents, with anxiety focusing on how they are perceived by others (Best et al., 2014).
Digital distraction from symptoms of anxiety or distress has been linked with avoidance of emotional experience rather than learning emotional regulation. Problems with emotional regulation are associated with anxiety and depression (Menninet al., 2002). Time online can displace young people’s face-to-face interactions. Preference for communication via texting, messaging, and email risks reinforcement of any pre-existing social impairments, anxiety, and avoidance, thereby, increasing the likelihood of low mood and compromised wellbeing (Leung, 2011). The interruption of a social technology or delay in responding to received messages have been associated with increased anxiety in young adults, with greater degrees of connection being associated with increased anxiety, depression and dependence (Durocher et al., 2011).
Recent US and UK guidance promotes parent–child discussion of screen time limits based on a child’s needs, reasons for screen use, content accessed, impact on physical or social activity and sleep (American Psychological Association, 2019; Royal College of Paediatrics and Child Health, 2018).
Cyberbullying
Cyberbullying is common among adolescents. Affected individuals have an increased risk of emotional, mental and physical health issues, including self-harm and suicidal ideation (Daine et al., 2013). Exposure to suicide-related content online, including details and encouragement, results in normalisation and increased suicidal ideation in some young people and aversion in others (Messina and Iwasaki, 2011).
Conclusion
The prevalence of anxiety in young people and the resultant number of primary care presentations is increasing. It is fundamental that GPs are able to promptly identify, assess and effectively manage anxiety in children and adolescents. GPs can preemptively explore predisposing factors while considering the wider context of the child. Effective management requires a multifactorial approach, building a relationship with the young person and their caregivers. External influences including home, school, social and social media need to be considered. A wide range of support services and resources are available for anxiety in young people, allowing management of many cases within primary care. Referral to CAMHS may, be required in urgent, severe, or refractive cases. Supporting the emotional development of children and adolescents should be seen as a long-term investment, giving them the best chance of wellbeing throughout their lives.
Case study
Emma (age 12 years) is brought to see you, her GP, by her mum. Her school have threatened to impose fines due to an increasingly erratic level of attendance. Mum has noticed that Emma increasingly seems ‘on edge’ and snaps at her regularly. Mum says that Emma is meeting friends less frequently. Emma worries about a wide range of things. She reports that she spends large amounts of her free time on her phone, particularly on Instagram and Snapchat, but also uses Reddit and other online forums. Mum and dad are separated, and mum admits to suffering with anxiety and depression herself.
Emma and her mother consent to you speaking with Emma alone. Emma tells you that she often uses her phone late at night and then struggles to sleep. She finds it hard to know who her real friends are, as people write things online that they do not say at school. She had a boyfriend, but he broke up with her online so that ‘everyone knew about it’. She tells you that she does not smoke, drink alcohol, or self-harm. However, she has friends who do and she has thought about harming herself. She has not told teachers at school that she struggles with anxiety, as she feels she might be singled out by them in front of her class. She feels her life is not as good as her classmates. This led to her having a panic attack. Some peers have made fun of this event. All of this, along with her regular tiredness, means that she often does not want to go to school.
You invite Emma’s mother back into the room and talk with them about sleep hygiene and Emma’s social media use. You encourage them to tell the pastoral team at school about how Emma is feeling and reassure them that she can discuss any plans that are put in place. You encourage more open dialogue between Emma and her mum. You also direct them towards the Moodcafe website for self-help resources on anxiety. You agree to see them again in 2 weeks and as required thereafter.
KEY POINTS
Prevalence of anxiety is increasing in children and adolescents A number of anxiety disorders exist, including: Generalised anxiety disorder, separation anxiety disorder, selective mutism, social anxiety disorder, obsessive–compulsive disorder, panic disorder and phobias Anxiety secondary to other physical and mental disorders in children and adolescents is common Social assessment including home, school and online situations can identify anxiety triggers Support, self-help and psychological therapies are first-line management; a large range of anxiety management resources and support are available for young people, their parents and carers Assessment for CAMHS involvement is recommended in urgent, severe or refractory cases, including self-harm and suicidal ideation