
Abstract
Hip pain is one of the most common musculoskeletal presentations in general practice. There are multiples causes of hip pain, ranging from acute to chronic and traumatic to atraumatic. In general practice, it is important to identify the cause of hip pain, as management strategies vary depending on pathology. Some diagnoses need urgent referral to secondary care, whereas others can be managed in primary care. According to the RCGP, an estimated 1-in-5 consultations are for musculoskeletal conditions, so a good knowledge of management is important. In this article, we will discuss the anatomy of the hip, the most common causes of hip pain and their management.
The RCGP curriculum and adult hip pain
The role of the GP in the musculoskeletal health clinical topic guide is to:
Advise appropriately to support the self-care and prevention of problems Intervene urgently when patients present with emergencies or ‘red flag’ symptoms Coordinate care with other health professionals leading to effective and appropriate acute and chronic management. Coordinate the holistic care of complex patients presenting with symptoms affecting the musculoskeletal system Communicate effectively taking into account the psychosocial impact of musculoskeletal problems on the patient, their family, friends, dependants and employers.
Knowledge, skills and emerging issues in this article from the relevant topic guides:
The natural history of the untreated conditions including whether acute or chronic The prevalence and incidence across all ages and any changes over time Typical and atypical presentations Recognition of normal variations throughout life Risk factors, including lifestyle, socio-economic and cultural factors Diagnostic features and differential diagnosis Recognition of ‘alarm’ or ‘red flag’ features Appropriate and relevant investigations Interpretation of test results Management including self-care, initial, emergency and continuing care and chronic disease monitoring Patient information and education including self-care Prognosis
People are living longer, and remaining active for longer, therefore musculoskeletal problems are presenting to general practice more frequently.
Musculoskeletal conditions are a common cause of severe long-term pain and physical disability and are major causes for work limitation and early retirement.
In cases of suspected inflammatory arthritis, urgent referral to a rheumatologist can have a significant impact on patients’ disease in both the short and long term.
Anatomy
The hip joint is made up of the articulation between the femoral head and the acetabulum. The design of the joint provides stability in this articulation. The hip joint surface is most stable when weight-bearing, reducing the possibility of dislocation. There are many factors that contribute to the strength and stability of the hip joint:
Ligaments: The iliofemoral, pubofemoral and ischiofemoral ligaments surround the hip joint. The strongest one being the iliofemoral ligament Capsule: Encircles the head and the neck and is strongest anteriorly and superiorly. It is also reinforced by the ligaments described above
Examining a hip joint
After a detailed and thorough history, examine the hip joint. As with all orthopaedic examinations, follow a ‘Look, Feel, Move’ routine.
Look at the patient to assess posture and visible signs of disease. A hip joint should ideally be examined with the patient standing up to exaggerate any deformity; however, in practice, this may be difficult due to pain, frailty or the age of the patient. From the front, you may be able to identify scars from previous surgery. There may be visible deformity in the patient’s anatomy with pelvic tilt or quadriceps- wasting indicating muscular disease. The hip joint should be assessed by looking from the side and back, in particular, for lumbar lordosis, which may be reduced in patients with osteoarthritis. There may be other findings such as erythema and swelling.
Assessing the gait can give a good indication of hip pathology. A Trendelenburg gait is a common pathological gait caused by weakness of hip abductors, usually after hip replacement surgery.
The hip joint can be palpated, first, around the anterior tissues of the hip. Any tenderness or warmth to touch may indicate an inflammatory or infective process. Always remember to compare hips to assess whether any pathology is bilateral or unilateral. Infective processes are more likely to be unilateral. In particular palpate the area overlying the greater trochanter. Any point tenderness here may indicate a diagnosis of greater trochanter pain syndrome.
Movements and the responsible muscles of the hip joint.

Atraumatic causes of hip pain
A large number of patients presenting in primary care with hip pain will report chronic atraumatic pain. We will consider some of the more common causes of hip pain not associated with trauma or injury.
Osteoarthritis
The most common cause of hip pain in adults presenting in general practice is osteoarthritis. It is defined as degeneration caused by breakdown of cartilage in one or more joints (Arthritis Foundation, 2019). It commonly affects the knees, hips, hands and spine, presenting with pain and stiffness. In more severe cases patients suffer with joint deformity and significantly reduced mobility secondary to pain. Symptomatic osteoarthritis is estimated to affect up to 8 500 000 people in the UK, and although the cause is not well understood it is more prevalent in older patients.
Under the age of 45 years, osteoarthritis is more common in men, but women have a greater incidence than men after the menopause, suggesting that hormonal factors may have an influence. Other risk factors include obesity, family history, occupation and previous joint injury (Musumeci et al., 2015).
Diagnosis can be made with a combination of history, examination and basic imaging techniques such as X-ray scans. The history will describe joint stiffness, worse after periods of inactivity, such as in the morning. There may be crepitus of the joints affected and a reduced range of movement. Plain radiographs are not usually needed to confirm the diagnosis, but can help in cases of uncertainty or to rule out other causes.
There are four cardinal signs of osteoarthritis on plain X-ray:
Joint space narrowing Osteophyte formation Subchondral cysts Subchondral sclerosis
The diagnostic criteria according to the National Institute for Health and Care Excellence (NICE) include an age above 45 years, activity-related joint pain and either no morning joint-related stiffness or morning stiffness lasting no longer than 30 minutes (NICE, 2014).
Osteoarthritis can be managed primarily in general practice. A conservative approach can be used initially in nearly all patients if diagnosed early. This will focus on risk factor management, such as encouraging weight loss and gentle exercise. The patient may be referred for physiotherapy to encourage and improve strengthening. Medical management will include analgesia based on the World Health Organisation’s analgesic ladder. If both conservative and medical strategies prove ineffective, then referral to secondary care is advised. A steroid joint injection may provide relief in some patients. Surgical procedures include total hip replacement and hip resurfacing procedures to restore joint integrity.
Rheumatoid arthritis
Rheumatoid arthritis (RA) is an autoimmune condition that causes pain, swelling and stiffness in joints. Symptoms can fluctuate, with flare-ups a feature of RA. Although RA affects smaller joints more commonly, it can affect the hip joint. A mono-articular presentation of RA in the hip is rare, and examination to detect disease, particularly in the small joints of the hands and feet, is important. If RA does affect the hip, as with all types of arthritis, pain and stiffness are the first symptoms. More severe disease can cause deformity and severely reduce the patient’s mobility.
Investigations can include blood tests, with specific markers such as rheumatoid factor and anti-cyclic citrullinated peptide to aid diagnosis. NICE recommend that patients with persistent symptoms in keeping with RA should be referred to a rheumatologist and be seen within 3 weeks of referral (NICE, 2019).
Treatment aims to reduce flare-ups and prevent the long-term complications of the disease. Surgery is only indicated in patients with destructive arthropathy to restore joint integrity and structure. Management of RA is mainly medical with immune-modulators and disease-modifying anti-rheumatic drugs being the mainstay of treatment.
Greater trochanter pain syndrome
Greater trochanteric pain syndrome (GTPS), more commonly known as trochanteric bursitis, is widely defined as inflammation of the trochanteric bursa. It is not true inflammation, as it tends to not have three of the four cardinal signs of inflammation. The bursa lies on the lateral side of the femur adjacent to the greater trochanter. The pathognomonic presentation is localised lateral hip pain, with a focal point of tenderness over the greater trochanter. The pain is worse on activity and can be exacerbated when lying on the affected side.
The prevalence for unilateral GTPS is reported to be 15.0% in women and 6.6% in men (Segal et al., 2007). The increased prevalence in women is thought to be due to altered pelvic biomechanics from an increased pelvic width, and perhaps a tighter iliotibial band as a result of this feature. However, this has not been substantiated by research.
GTPS is caused by a variety of mechanisms. Although the exact pathology is not fully understood, the most common theory is that friction between the greater trochanter and iliotibial band causes chronic micro-trauma to the gluteal tendons inserting into the greater trochanter. This results in local inflammation with localised and focal pain. The diagnosis can usually be made just on history and examination, with other investigations only necessary to rule out other diagnoses.
GTPS is usually self-limiting, although some cases do persist. The patient should be advised to rest and cool the area. Exercise, weight loss, physiotherapy and non-steroidal anti-inflammatory agents such as ibuprofen can be useful to aid both pain relief and healing. If the pain does not respond to these basic measures then a peri-trochanteric corticosteroid injection may useful in the short term to enable effective and intensive physiotherapy (NICE, 2016). Reid et al. found that high doses of corticosteroid injection show significant benefits in pain relief in the first 3 months, with a peak benefit at 6 weeks.
Other strategies such as platelet-rich plasma injections or shockwave therapy have been investigated, but are not recommended by NICE, however, they may have a role in refractory cases.
Malignancy and metastasis
Patients may also present with hip pain, with an underlying diagnosis of malignancy, either primary or secondary. Primary malignancies are rare in adults, however, diagnoses such as osteosarcoma should always be considered. More commonly, hip pain is a sign of metastasis from another primary tumour. Cancers well known to affect the pelvis and femur include:
Breast Lung Kidney Prostate
The common presenting complaint will be hip pain that is gradually becoming worse, to the point of limiting function, or a fracture of the hip after minimal or no trauma (a pathological fracture). The patient may also complain of constitutional symptoms such as unintentional weight loss, fatigue and loss of appetite.
Plain radiographs may show lytic or sclerotic lesions indicating malignancy and require referral to secondary care for further investigation under a 2-week rule pathway, with, for example, computed tomography (CT) or magnetic resonance imaging (MRI) scans. Further investigations such as tumour markers, endoscopy and CT scans (chest, abdomen pelvis) may be required to identify the primary tumour.
Mirel classification.
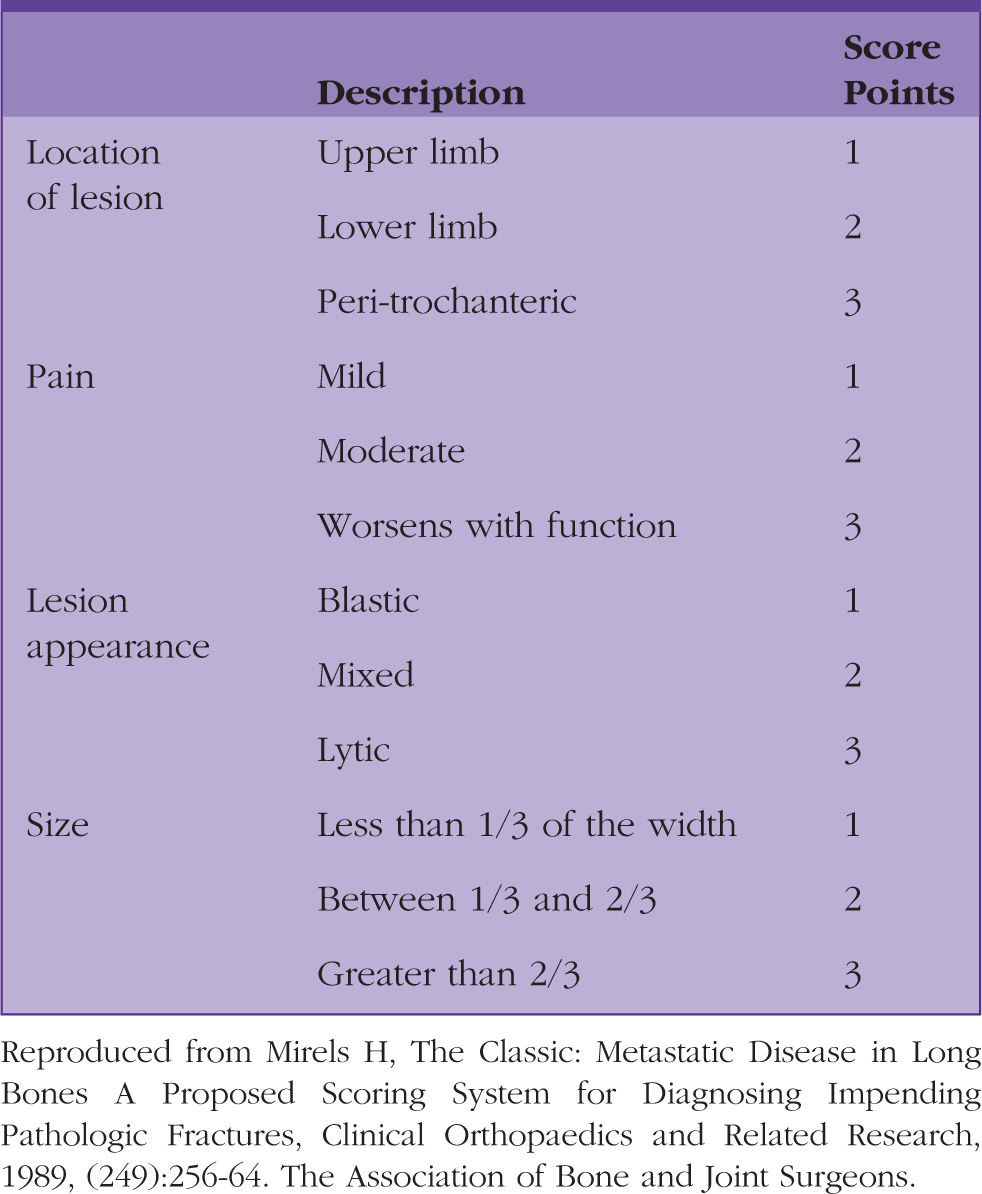
Reproduced from Mirels H, The Classic: Metastatic Disease in Long Bones A Proposed Scoring System for Diagnosing Impending Pathologic Fractures, Clinical Orthopaedics and Related Research, 1989, (249):256-64. The Association of Bone and Joint Surgeons.
This tool is used regularly in secondary care to govern the management of pathological fractures. As a rule of thumb, a combined score of greater than eight warrants prophylactic fixation with an intramedullary nail due to the high risk of pathological fracture. In cases where bone tumours, either primary or secondary, are identified, the opinion of an orthopaedic surgeon is needed for further management and follow-up.
Septic arthritis
Septic arthritis is possibly one of the most common emergencies that orthopaedic surgeons are asked to rule out by primary care, and a sound understanding can allow quick diagnosis and onward referral for definitive management. Septic arthritis is a painful infection within a joint. The spread of micro-organisms may be hematogenous or from a penetrating injury. It is one of the few orthopaedic emergencies that require urgent operative intervention; it most commonly affects the hips and knees.
Septic arthritis is extremely uncommon, with incidence being approximately 2 to 6 cases per 100 000-person years in industrialised countries. However, the fatality rate per case is 11%, which is why early diagnosis is essential (Garcia-Arias et al., 2011). Risk factors include immunosuppression, penetrating trauma, previous or current blood-borne infections and intravenous drug use. Patients with recent joint surgery, such as a total hip replacement or hemiarthroplasty, are also at risk and prompt diagnosis needs awareness of this fact. Staphylococcus aureus is the most common organism responsible for a septic joint.
The non-specific presentation of septic arthritis means there are a number of conditions that can mimic septic arthritis, including gout and even osteoarthritis. Septic arthritis presents with severe pain, redness and swelling of the affected joint. Other features that can aid diagnosis include high temperature, difficulty in weight-bearing or reduced range of movement.
Reactive arthritis is an important differential diagnosis. In reactive arthritis, the immune system cross-reacts with the joint synovium causing pain, usually in the hips, knees, ankles and feet. It usually presents 1 to 4 weeks after the initial infection, but can have a relapsing and remitting course for some time. It is difficult in primary care to distinguish between reactive arthritis and septic arthritis, as the signs and symptoms are the same or very similar. If there is diagnostic doubt, or difficulty, consider urgent secondary care referral. If septic arthritis is suspected, immediate referral to secondary care orthopaedics is indicated.
Subsequent investigation will include plain radiographs and blood tests to assess the inflammatory markers and any soft tissue reaction. These may be normal, making diagnosis more difficult. Further investigation may require joint aspiration, but this requires caution, as in cases of cellulitis overlying the joint bacteria can be seeded into the joint. Gram staining of the aspirated sample enables detection of bacteria within the joint fluid and if confirmed a washout of the joint can be conducted to further define and isolate the micro-organism.
S.aureus is the most common cause of septic arthritis in all countries; however, other bacteria can be responsible for infection. In children, Haemophilus Infleunza and Group A Streptococci can be implicated in septic arthritis. Neisseria Gonorrhoeae may be a cause in sexually active patients under the age of 40 years.
Treatment is intravenous antibiotics based on local microbiology guidance; it is initiated once a sample has been obtained either via an aspirate or a more extensive joint washout unless the patient’s condition warrants earlier initiation of treatment.
Trauma
Acute trauma patients can present in general practice and depending on the suspicion of bony injury these patients generally need secondary care referral more urgently than atraumatic causes.
Hip fractures
Hip fractures not only constitute a large drain on healthcare resources nationally, but are also responsible for significant morbidity and mortality. Data suggests that hip fracture mortality rates are 10% at 1 month, rising to 30% at 1 year (Lisk and Yeong, 2014). There are multiple factors producing these grave statistics. Patients affected by hip fractures tend to be vulnerable and frail, with a higher associated risk of chest infection and other illnesses immediately post-operative and during rehabilitation from the injury.
Clinical findings typically include a shortened and externally rotated limb and severe pain at rest. Plain radiographs are the first line investigation. However, with impacted neck of femur fractures it can be difficult to identify a small fracture on an X-ray scan. NICE guidance recommends MRI imaging in such cases if the clinical picture suggests a neck of femur fracture. If MRI imaging is not available within 24 hours a CT scan is recommended (NICE, 2011).
Management is usually surgical. There are many classifications of hip fractures in the literature and these inform what type of implant or fixation is required. The Garden classification is the most used classification (Fig. 1).
Garden classification.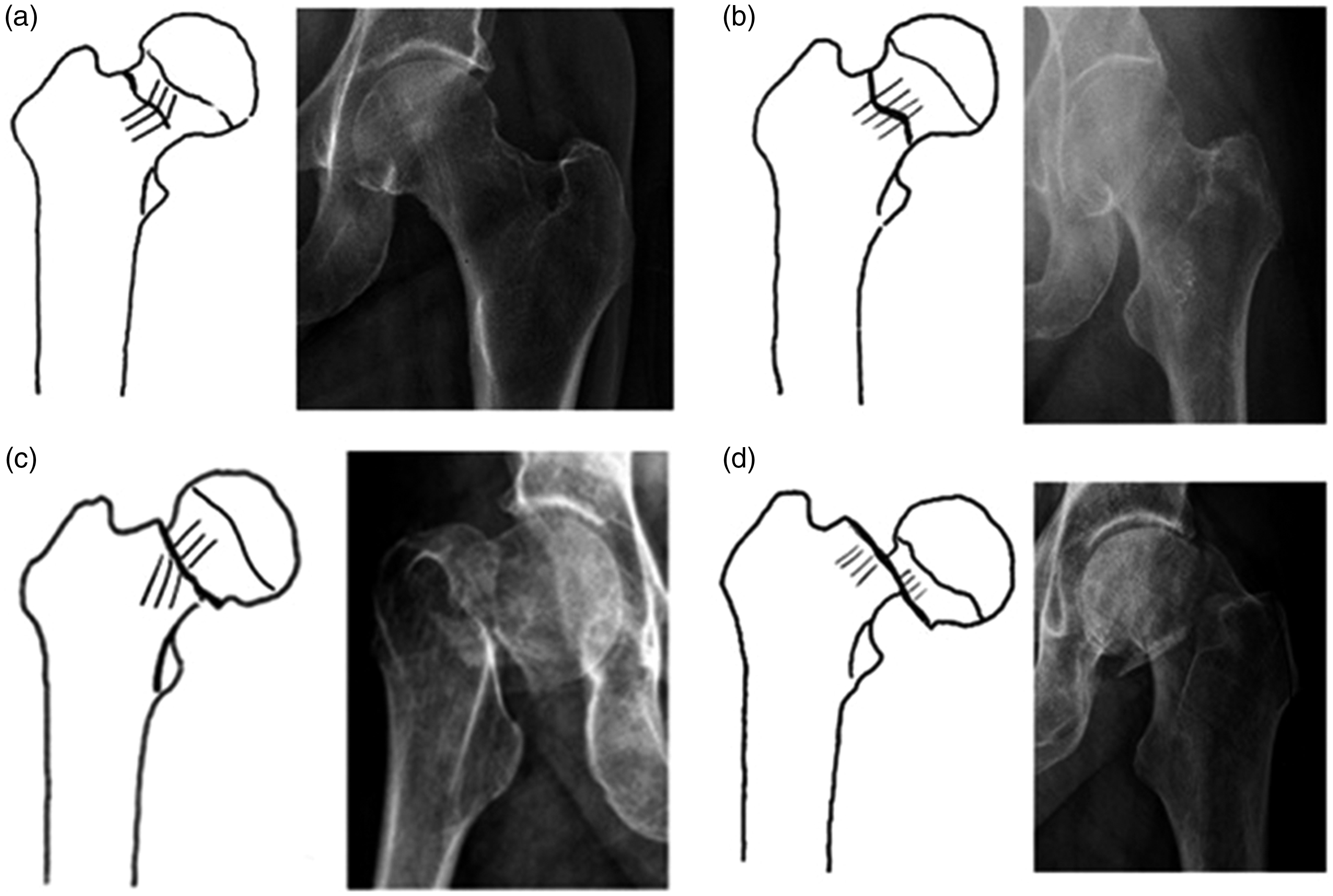
Garden I and II fractures are treated with fixation (either a dynamic hip screw or intramedullary nail). Garden III and IV fractures are treated with hip hemiarthroplasty or total hip replacement, depending on the patient’s comorbidities and mobility. The aim of treatment is to allow the patient to weight-bear from day 1 and to thus reduce the risk of further complications.
Avascular necrosis
The blood flow to the femoral head originates from an anastomosis of the medial and lateral circumflex arteries. It is retrograde and essentially governs the choice of surgical procedures in hip fractures. Avascular necrosis (AVN) of the hip occurs when this retrograde blood is obstructed causing death of the femoral head. The most common cause is traumatic interruption of blood flow to the femoral head from a fracture. Patients may complain of difficulty weight-bearing on the affected joint. Late presentation may feature pain while lying down. Pain is typically referred to the groin, thigh or buttock. AVN is also associated with atraumatic causes from, for example, long-term use of steroid medication or excessive alcohol intake (Mayo Clinic, 2018).
A history of worsening pain, exacerbated by weight-bearing on the affected limb, is typical. The pain is usually centered at the thigh and groin. Examination findings include a reduced range of joint motion, joint tenderness on palpation and pain on passive or active joint movement.
When the diagnosis of AVN is considered, orthopaedic referral is required. Diagnosis is with plain X-rays. The X-ray signs include subchondral lucency on the proximal part of the femoral head, known as the ‘crescent sign’ (Radiopedia, 2019). Other features include joint effusion or signs of degenerative change. Further investigation includes CT or MRI scanning.
Psychological impacts of musculoskeletal pain
Musculoskeletal disorders can have a major impact on patients’ quality of life and mental health. They can cause problems such as depression. However, the wider social impact includes lengthy absences from work and more dependence on an already stretched social support system. For example, one study in a rural population in Greece found that patients with musculoskeletal disorders had much lower SF-36 scores (a quality of life questionnaire) and much higher rates of depression (Antonopoulou et al., 2009).
Although definitive management of acute trauma is in secondary care, GPs manage the wider and continuing impact of a wide range of musculoskeletal disorders on patients’ mental health and quality of life.
KEY POINTS
Hip pain in adults is a very common presenting complaint in primary care Diagnosis can usually be made on history and examination with plain radiographs often used, for example, to investigate and rule out bony injury Osteoarthritis is the most common cause of atraumatic hip pain In a red, hot and swollen joint with pain and a limited range of joint movement septic arthritis should be considered If a hip fracture is suspected, but plain radiographs are inconclusive, further scans using CT or MRI is required If AVN or septic arthritis are suspected, urgent orthopaedic referral is required