
Abstract
Growing numbers of people live with multi-morbidity. As patients’ lists of co-morbidities grow, so do the lists of their medications. Polypharmacy presents a significant challenge for both patients and clinicians. Polypharmacy can be appropriate, improving quality of life and life expectancy, but problematic, especially for patients living with frailty, and a growing burden. The task of trying to rationalise an extensive list of medications in a 10-minute appointment can seem like an impossible task. Guidance and support specifically aimed at trainees is limited. This article offers a starting point for GP trainees to stimulate their own exploration of this rapidly evolving subject.
The RCGP curriculum and polypharmacy
The role of the GP in the improving quality, safety and prescribing professional topic guide requires:
Targeted assessment of the patient and other sources An appropriately detailed understanding of the patient’s history Wherever possible, an agreement with the patient and their carers on the treatment proposed That the prescription is in the patient’s best interests, correctly and clearly prescribed, and accurately documented within the patient record Review by a suitable healthcare professional at an appropriate time Diagnose, investigate and manage older adults taking into account theories of ageing, differences in epidemiology and risk factors of disease in the elderly population Communicate appropriately with patients, their families and carers Coordinate with other organisations and professionals Review medications and repeat prescriptions effectively, potentially working with pharmacists Ensure care promotes patients’ sense of identity, independence, personal dignity and that the patient is not discriminated against as a result of their age Co-morbidity and physical factors disproportionately affect the health of older people and will influence the management of existing disease A problem-based approach is important, taking in the ‘big picture’, rather than a disease- based approach to the care of older people Risks of polypharmacy (including the increased risks of significant cross-reactions and side effects)
Life stages topic guide: Older adults As a GP, your role is to:
Key knowledge and skills: Recognising As a GP, you should recognise that:
Polypharmacy: The challenge for trainees
Defining appropriate and problematic polypharmacy.
A consultation with Bob.
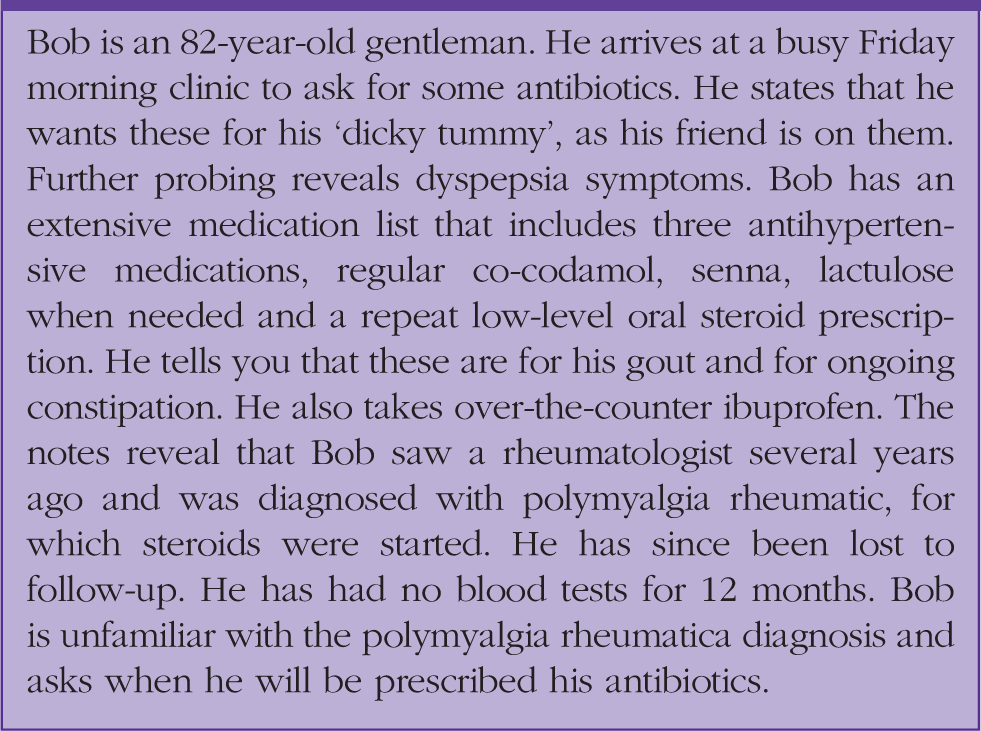
This consultation with Bob raises many questions. It appears that Bob is burdened with the use of regular laxatives, due to his on-going opioid use, and possibly by the use of multiple antihypertensive medications. There is a question about whether his use of steroids has contributed to his dyspepsia symptoms. Can the steroids be titrated down in light of the polymyalgia rheumatica (PMR) diagnosis? What effect has the ibuprofen had on both his dyspepsia and his kidney function? How can we educate the patient about the complex effects of these medications on the body? The patient wants antibiotics to treat his abdominal pain, now. How can we navigate all these issues for the patient? Above all else, how do we manage this in whatever is left of the 10-minute appointment slot?
Within this array of questions, a number of core GP principles are highlighted: the importance of exploring and checking a patient’s understanding and expectations, of follow-up and review of both medication and diagnoses in a patient with long-term conditions. Many of the challenges in polypharmacy consultations can be managed using good general practice consultation skills. Managing polypharmacy requires evidence-based knowledge of not only the mechanisms of action of medications, their side effects and interactions, but also an understanding of how multiple medical issues affect our patients.
Polypharmacy, however well intentioned, is far from benign and is associated with increased risks of adverse drug reactions (ADRs). A team using data from the UK Biobank project (Hanlon et al., 2018), identified that patients with chronic obstructive pulmonary disease (COPD) who were also suffering from other co-morbidities were more likely than similar patients without COPD to be prescribed medication contributing towards falls, constipation, urinary retention, central nervous system depression, bleeding and renal injury. We prescribe opioids for pain relief, which causes constipation, and in turn, we then prescribe laxatives for the treatment of constipation. However, elderly patients on laxatives are twice as likely to fall (Bloch et al., 2010). Thus, we have increased the patients’ risk of injury and hospital admission. It is not only the use of medicines associated with ADRs that is of concern to the clinician. Evidence indicates that 5–20% of prescriptions contain errors (Avery et al., 2012). The more medication a patient is taking, the higher the chance that one of the prescriptions will contain an error. Iatrogenic illness in patients with multi-morbidity can cause considerable harm. We must be mindful of how we educate patients about the risks and benefits of on-going medication, so that they are able to make informed decisions about the management of their own health conditions.
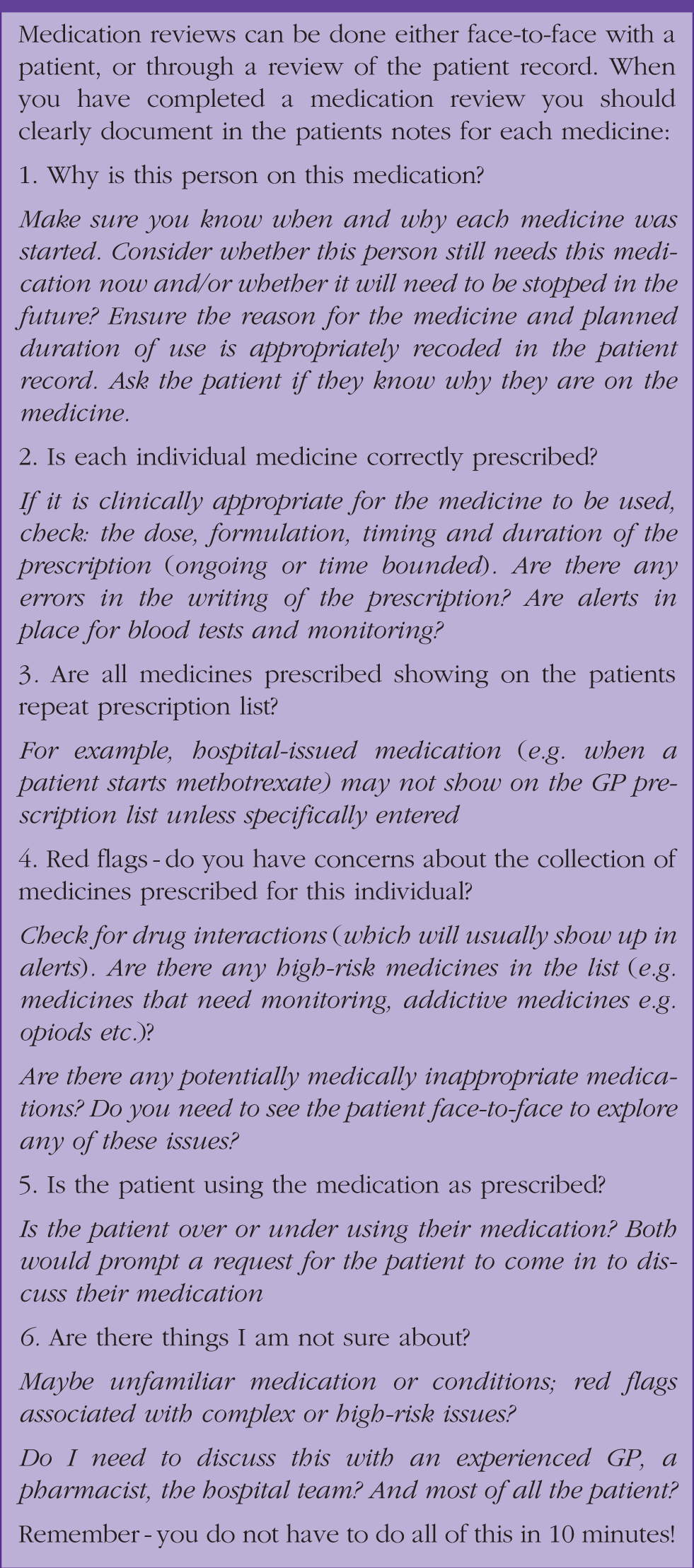
Optimising medicines: A medication review check list.
Bob was fortunate to see an excellent GP trainee who reviewed his PMR diagnosis, was able to wean him off his steroid and so discontinue many of the associated medication. However, Bob still had raised blood pressure and was prescribed multiple antihypertensive medications. He came back to see the trainee (whom he now regarded as his regular GP) and reported still feeling burdened by all his tablets. ‘Doctor, do I really need all of these tablets?’ he asked.
Bob’s question now comes into the complex territory of problematic polypharmacy (Box 2). The intended benefit from a medical perspective is to control blood pressure, but Bob’s perception of benefit may differ. There may be a need for compromise between the goals of medicine and the goals of the patient (Duerden et al., 2013).
Polypharmacy: The challenge for patients
Appropriate polypharmacy applies evidence-based medical practice to improve outcomes for patients. However, a growing evidence base highlights what can be appropriate from a medical perspective, may be problematic from a patient/personal perspective (Denford et al., 2014).
Despite moving away from the age of paternal medicine and towards shared decision making, insufficient attention has been given to the demands placed on patients when trying to comply with the prescription of multiple medications. There is growing recognition of the burden for patients of taking multiple medicines, even when prescribed appropriately. The average number of items dispensed per head of population has risen from 15.5 (2007) to 20.0 (2016) (NHS Digital, 2019). This increase in prescribing is particularly high in the elderly, with 10% of over 65 year olds being prescribed over 10 simultaneous medications (Guthrie and Makubate, 2012). Patients report feeling burdened by the work of taking their medicines: 40% of people taking five or more medicines a day report feeling burdened by their medication (Krska et al., 2018), which may explain why 30–50% of medication is not taken as intended. When we start to think about rationalisation and optimisation of medication to support individual patient health and wellbeing we may need to recognise that the compliance of the patient may be more of a key to delivering optimised care than, for example, adding a second antihypertensive medication.
The patient’s perspective on their medication is an important consideration for clinicians. A patient with too many medications may frequently miss doses. Patients who become fed up with taking too many pills many choose to omit the ones that they feel offer no benefit. This may be particularly true for medication used in primary prevention. If such medication is effective, the patient will be none the wiser and never experience symptomatic benefit. Compliance can also be impaired by side effects, more likely with polypharmacy. Just because it is biomedically appropriate to prescribe, does not mean it is right for the patient. We may sometimes forget that there is more to our patients’ lives than taking pills! Patient experience is essential in developing appropriate prescribing guidelines, but often overlooked. A review of reports on medicines optimisation published by the Royal Pharmaceutical Society, The King's Fund and National Institute for Health and Social Care Excellence between 2013 and 2017 (Heaton et al., 2017) showed a paucity of attention to the issue of patient experience in published guidelines on the use of medication. In fact, only The King’s Fund considered evidence from qualitative studies of people's use of medicines. This highlights an important issue with evidence-based guidelines. Guidelines aim to inform the best care for the broad majority of the cohort in question, but this can be at the expense of truly individualised care. The good clinician knows when to deviate from guidelines to provide optimal care for the individual patient.
Finding solutions: Rethinking how we use medicines for person-centred care
So how do we find a way to optimise medication use for our patients? Individualisation of prescribing is the key to safe and effective prescribing in multi-morbidity. However, there is a lack of clarity in the literature over what direction individualisation should take (Denford et al., 2014). There is a considerable amount of research that is focused on the exciting field of pharmacogenetics, but little attention on studies involving how patients and clinicians can work together to create optimised person-centred treatment plans. Denford et al. (2014) suggest ‘mutually agreed tailoring’ as a method of developing treatment plans with patients. These plans encourage patients to take a greater role in their own care and include patients having more knowledge about side-effect profiles (including advice on which side effects may be tolerable), how to monitor medication effects at home, and having an input on what times are best for patients to take their medication.
Trainees – and indeed the wider profession – need more help and guidance to IDENTIFY those burdened rather than benefited by their medicines and so to MANAGE deprescribing when patients want to discuss stopping tablets. However, the evidence on what to do and how to do this is limited (Avery and Bell, 2019). This may explain why clinicians find it hard, in practice, to tailor medication to the individual needs of patients. A recent study examined professional barriers to tailoring medication (Reeve et al., 2018). GPs recognised the objective of starting medication, in line with guidelines and patient expectation. Stopping medication requires more cognitive input than is required when following well-used guidelines for commencing medication. Clinicians reported not having the opportunity (or 'the headspace’) to engage with the rationalisation of medication as often as they would have liked. GPs expressed concern about the lack of professional training given to deprescribing. Finally, physicians expressed anxiety about working outside of (and in some cases directly against) guidelines. Specifically, in light of growing litigation, GPs felt vulnerable and concerned about the consequences of not following guidelines.
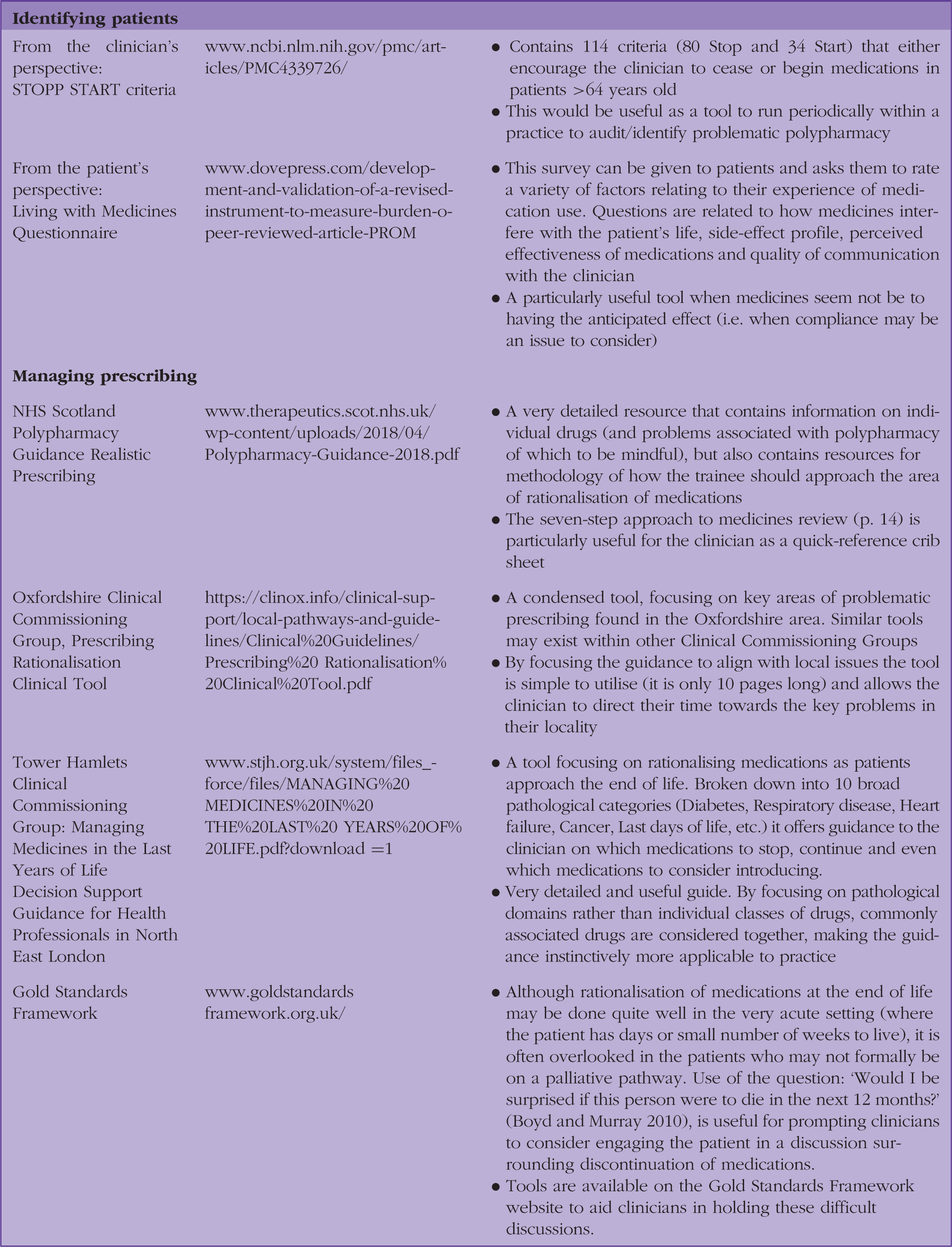
There are now a number of tools being developed to support clinicians in rationalising medication. Evidence of an impact on medication load and on patient mortality remains limited (Avery and Bell, 2019). One meta-analysis suggests a decrease in medication of only 0.2 drugs per patient, on average, following use of such tools. Another meta-analysis showed no overall reduction in patient mortality from such interventions (Page et al., 2016). However, the tools may help individual clinicians and patients to work together safely and achieve person-centred decisions about medication.
Tools available to identify and manage problematic polypharmacy.
Gaps still to fill: A rapidly evolving field of practice
Education around deprescribing is being rolled out as part of junior doctor training (Poots et al., 2017). Tools are available to aid clinicians with overcoming problems associated with polypharmacy. These tools are varied and with interrogation of the literature clinicians are likely to find tools that fit their own practice. These tools are far from perfect, however. Reviewing a patent’s medication in a systematic way is a significantly time-consuming task; it may be complicated by patients’ cognitive impairment or poor understanding of how their medication works. It may be necessary to involve carers or nursing home staff in effective rationalisation of medication and to ensure that medication is optimised to individual patient’s needs.
It would be neglectful to consider rationalisation of medication without recognition of the on-going GP workforce crisis. According to the survey undertaken by Reeve et al. (2018), GPs want to engage more with deprescribing and individualisation of prescribing, but feel constrained by the lack of time. In addition, 32% of GPs report burnout (Patel, 2019). How can GPs incorporate new methods of working into practice? Neural networks and deep learning may offer assistance to the over-burdened GP. A team in Stanford, USA has developed a neural network named Decagon to look at documented side-effect profiles of medications alongside protein–protein interactions that can predict side effects associated with polypharmacy (Zitnik et al., 2018). Such tools may be used to alert prescribers to interactions that would otherwise be missed in high-pressure short-duration consultations; they will become invaluable as polypharmacy continues to increase in prevalence.
GPs no longer work alone in practices. The rise of the multi-disciplinary team is beginning to ease the pressure on GP workloads across the country. The work associated with rationalising medications and identifying those at-risk from the perils of polypharmacy need not fall entirely on the shoulders of GPs. Practice pharmacists will be able to help tackle this problem. There is NHS funding for 20 000 new staff (NHS England, 2019), and an opportunity for rationalisation of medications and identification protocols for problematic polypharmacy to be part of everyday practice. This aim and opportunity is recognised by our pharmacist colleagues (McClay and Gyimah, 2019).
Conclusion
Managing polypharmacy – especially problematic polypharmacy – is a challenge for trainees and qualified clinicians alike. Many of the issues arising can be dealt with using good evidence-based medicines management, and the core principles of good general practice including whole-person assessment, good communication skills and continuity of care.
However, problematic polypharmacy requires medical practice to pay greater attention not only to the disease that people have, but to the delivery of whole-person care based on the principles and practice of expert generalist medicine. Tools and ways of working are evolving, but the needs of patients are also evolving and present a challenge to evidence-based practice. Good team work is needed to define, deliver and educate in all aspects of this important, emerging area of practice.
KEY POINTS
When considering polypharmacy and rationalisation of medication remember the principles of good general practice and person-centred care Explore the ideas, concerns and expectations that patients have about their medication Ask patients if they feel burdened by their medication and invite them to work with you to identify possible areas for compromise Identify and use tools to help with the management of polypharmacy and rationalisation of medication; with your trainer reflect and learn from use of these tools Complex management and decisions deserve time, attention and teamwork Remember you are part of a team: share complex decisions to benefit from the critical, collaborative and thoughtful involvement of other GPs and pharmacists
ORCID iD
Joanne Reeve https://orcid.org/0000-0002-3184-7955