
Abstract
Measurement of urinary protein is an essential part of the evaluation of chronic kidney disease; it has both diagnostic and prognostic significance. Proteinuria is an independent risk factor for progression of renal disease, but is also independently associated with increased cardiovascular mortality. Despite its far-reaching implications, the definition, diagnosis and treatment of proteinuria can cause confusion in primary care. Early detection of proteinuria in the context of diabetes or otherwise is vital given the potential for intervention to reduce urinary protein losses and improve renal and cardiovascular outcomes. This article will focus on the definition, potential causes and management of proteinuria, including which individuals should be referred to secondary care.
The RCGP curriculum and proteinuria
The role of the GP in the kidney and urology clinical topic guide is to:
Identify and manage chronic kidney disease and understand the interventions that can delay its progression and reduce the associated increased cardiovascular morbidity and mortality Know when to refer and when not to refer, avoiding futile investigation and escalation and encouraging supportive care Diagnostic features and differential diagnosis Appropriate and relevant investigations Interpretation of test results Management including chronic disease monitoring
The knowledge and skills guide states GPs should consider:
Background
Proteinuria is a broad term for the presence of protein in the urine. This largely occurs when increased glomerular permeability, due to alterations in the basement membrane and glycocalyx, cause abnormal loss of proteins normally present within plasma (Kidney Disease Improving Global Outcomes (KDIGO), 2012a). Due to its charge, quantity, and molecular mass, albumin makes up most of the urinary protein loss in most kidney diseases, and hence, the term albuminuria is often used.
Some confusion may arise about the difference between proteinuria and albuminuria. For simplicity, proteinuria should be considered the overarching term for the pathological presence of protein in the urine with albuminuria referring to its most common constituent. Clinical practice is now moving towards measurement of albumin, given its role in the majority of kidney diseases and more specifically, given the relationship between the level of albumin in the urine and kidney and cardiovascular risk (KDIGO, 2012a). The urine albumin creatinine ratio (ACR) will detect lower levels of protein in the urine and is a more sensitive marker of kidney damage than protein creatinine ratio (PCR). ACR is therefore recommended in the diagnosis of chronic kidney disease (CKD) (The National Institute for Health and Care Excellence (NICE), 2015a).
Diagnosis
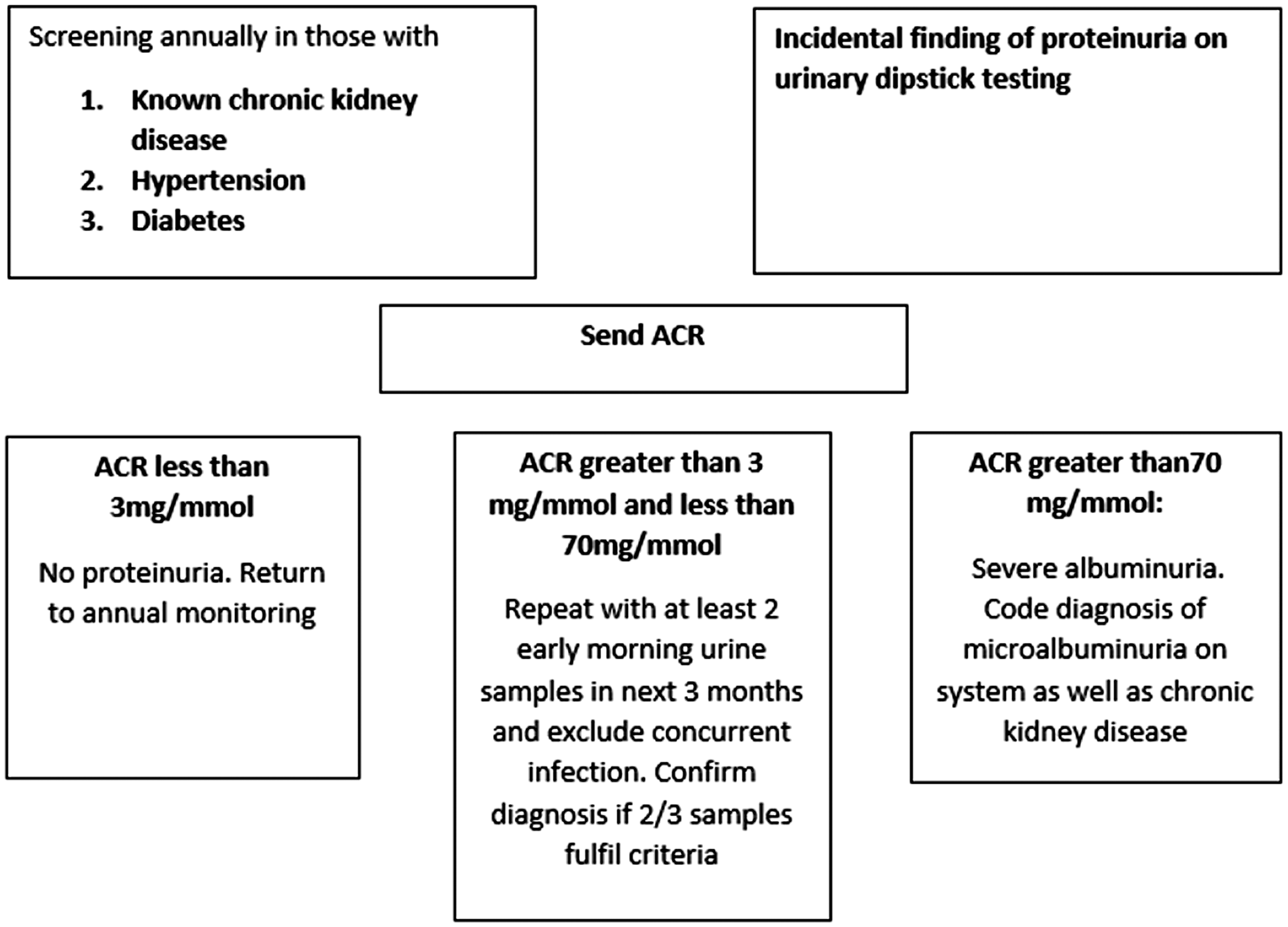
The interpretation of urinary ACR measurements.

CKD is defined as a decreased estimated glomerular filtration rate (eGFR) of less than 60 ml/min/1.73 m2, and/or markers of kidney damage, for at least 3 months duration, regardless of the underlying aetiology. An important point is that irrespective of eGFR, the KDIGO classification considers persistent albuminuria to represent CKD (KDIGO, 2012a). Figure 1 illustrates this classification with the various colours of green, yellow, amber and red indicating degrees of risk of progression to end-stage kidney disease.
KDIGO classification. Risk of CKD progression to end-stage kidney disease by eGFR and albuminuria category. Green, low risk (if no other markers of kidney disease, no CKD); Yellow, moderately increased risk; Orange, high risk; Red, very high risk.
‘Kidney diseases’ are in the top-20 leading causes of death worldwide, and projections for 2030 from the World Health Organisation (WHO) indicate this will remain the case where they are implicated in 1.6% of all deaths (WHO, 2013).
Increased ACR and decreased eGFR, respectively, act in combination to multiply the risk of adverse outcomes. Early detection of disease progression can allow for timely preparation for renal replacement therapy for people with CKD stage 4 before progression to stage 5 disease (NICE, 2015a).
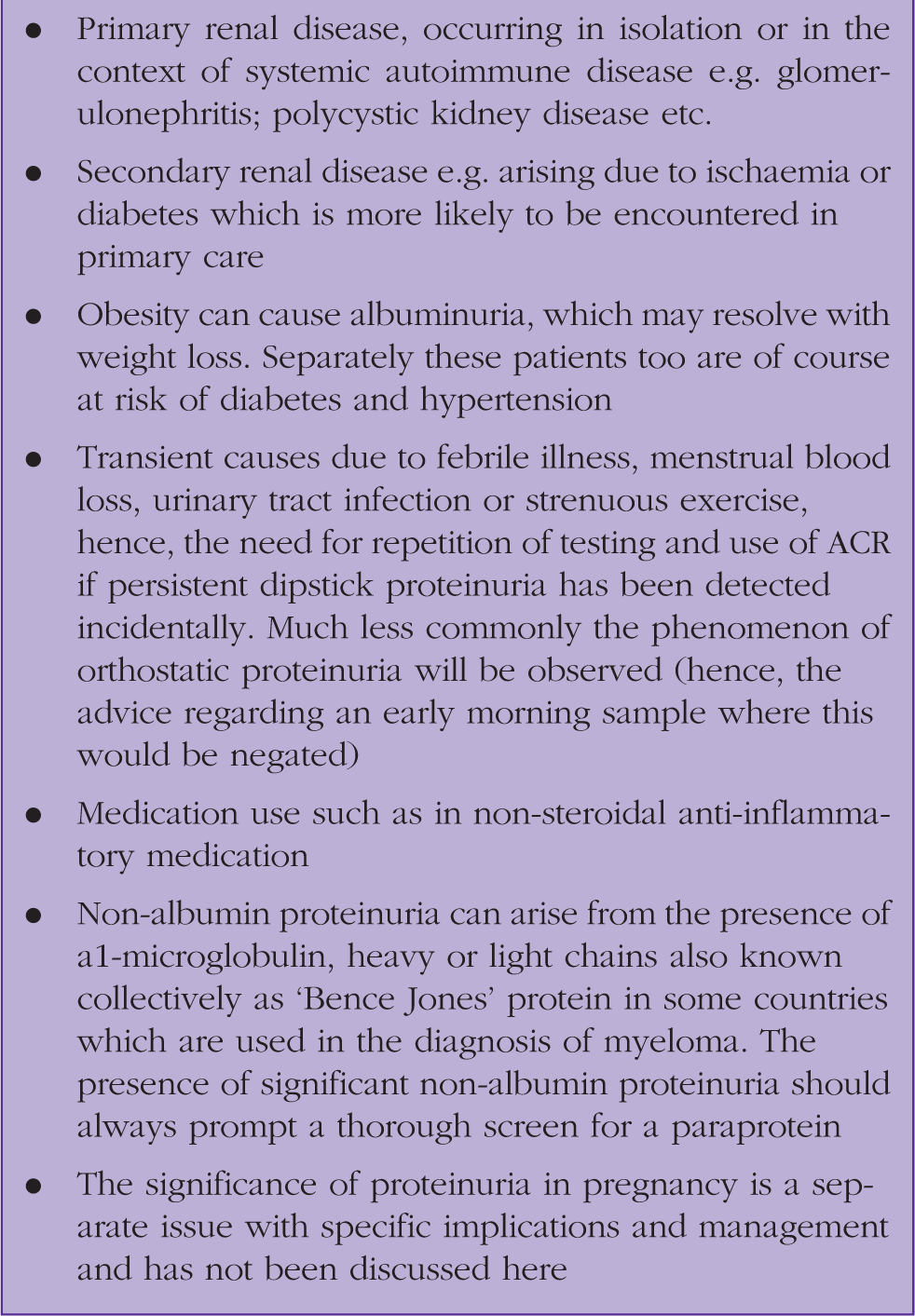
Causes of proteinuria.
Clinical features
Proteinuria is generally a silent condition. However, if lost in massive quantities, this can present as nephrotic syndrome, in which case the urinary protein losses are sufficient to deplete serum albumin and result in peripheral oedema and other complications. There is good evidence that albuminuria detected via ACR is the earliest marker of glomerular disease in many kidney diseases where it may appear before a reduction in eGFR, and hence, present a useful opportunity for intervention (KDIGO, 2012a).
Measurement
Screening for CKD via ACR in the general population is not advised. Quantification of proteinuria via ACR is, however, recommended in specific instances (NICE, 2015a) (Fig. 2):
Patients with diabetes CKD established by a decreased eGFR (at diagnosis) and annually for monitoring Situations where there is a strong suspicion of CKD even if eGFR is normal Patients with hypertension on initial diagnosis and annually as part of monitoring Patients with cardiovascular disease on initial diagnosis Patients with structural renal tract disease Patients with multisystem diseases with potential renal involvement, e.g. systemic lupus erythematosus Patients with a family history of end-stage kidney disease When haematuria is opportunistically identified A summary based on NICE guidance on detecting proteinuria.
An early morning urine spot test is sufficient for analysis and counteracts any spurious results that could arise from orthostatic effects. There is no requirement to complete a 24-hour collection.
The National Diabetes Audit 2017–18 for England and Wales unfortunately highlights the inconsistencies in screening for renal disease in diabetics. The level of urine albumin was checked in 52.3% of individuals with type 1 diabetes, whereas 66.2% of patients with type 2 diabetes were checked (National Diabetes Audit, 2018). Similarly, The National Chronic Kidney Disease Audit found that in population studies in England and Wales, of those with hypertension, less than 30% of people had an ACR performed (National Chronic Kidney Disease Audit). Moreover, this indicator has also been removed from the Quality and Outcomes Framework in England in Wales for CKD which may exacerbate existing confusion over the role and importance of albuminuria testing in primary care now this incentivising feature is absent (Fraser et al., 2016).
Management
Management of proteinuria comprises blood pressure control, especially with inhibitors of the renin-angiotensin system such as the angiotensin converting enzyme inhibitor (ACEi) and angiotensin receptor blocker (ARB) medications, which have direct anti-proteinuric benefits as well as blood pressure (BP)-lowering effects. Management of the underlying cause of kidney disease should be optimised where possible, such as by improved glycaemic control in patients with diabetes, and escalated immunosuppression in the context of autoimmune diseases (the latter managed more commonly in secondary care and beyond the scope of this article).
Blood pressure control
The appropriate target for BP in the presence of proteinuria will vary. Tighter control is desirable in those with diabetes and/or higher ACR (NICE, 2015a). An individualised approach should be taken in primary care where co-morbidities, coexisting medications, age and perceived tolerability of treatment will be important considerations in addition to rigid guidance. Figure 3 summaries these principles.
A summary of BP control in relation to proteinuria.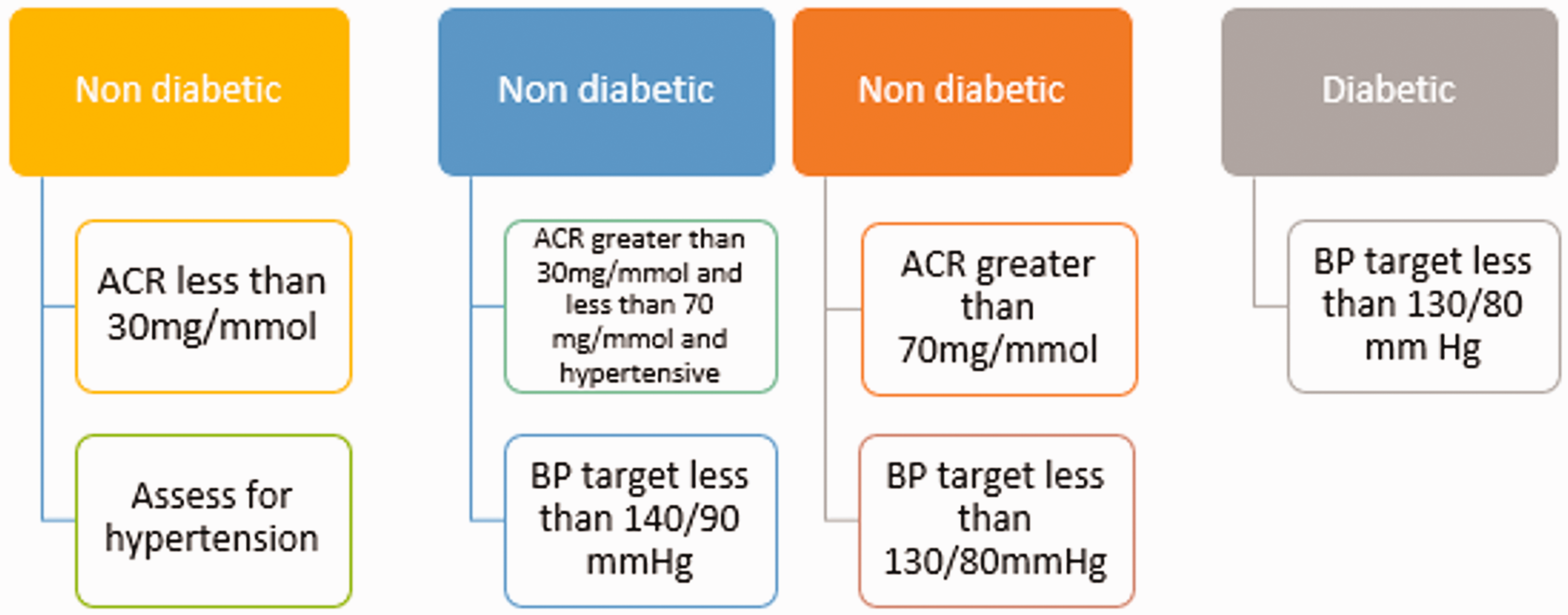
Renin angiotensin system blockade
ACEi and ARB medications are effective anti-hypertensives, but also reduce proteinuria independently of their BP-lowering effect. In several landmark trials in the 1990s the anti-proteinuric effect was established initially in type 1 diabetes, then type 2 diabetes and other proteinuric kidney diseases (Maschio et al.,1996; Parving et al., 2001; Viberti et al., 1994). ACEi and ARB medications are the first line anti-hypertensives of choice for those requiring BP-lowering treatment, apart from those with African or Caribbean family origin, where hypertension is less renin angiotensin dependent.
Patients with ACR greater than 70 mg/mmol and no contraindications should receive an ACEi or ARB if tolerated, irrespective of BP or cardiovascular disease. Those with ACR between 30 and 70 mg/mmol and hypertension should receive ACEi or ARB medication for dual treatment of BP and proteinuria. However, individuals with ACR less than 30 mg/mmol and hypertension should be managed based on standard hypertension guidelines and not automatically receive an ACEi or ARB.
Patients with diabetes mellitus with a urinary ACR of 3 mg/mmol or more and no contraindications should receive an ACEi/ARB to achieve the optimal tolerated dose. There is currently no benefit to treatment with an ARB/ACEi, and as these are also associated with an increased risk of hyperkalaemia and acute kidney injury, this approach is not recommended (Fried et al., 2013).
ACEi and ARB medications cannot be taken during pregnancy and should be converted to alternative anti-hypertensive agents during pre-conception planning. Management of hypertension and proteinuria during pregnancy and breast-feeding is beyond the scope of this article and should be managed with specialist advice.
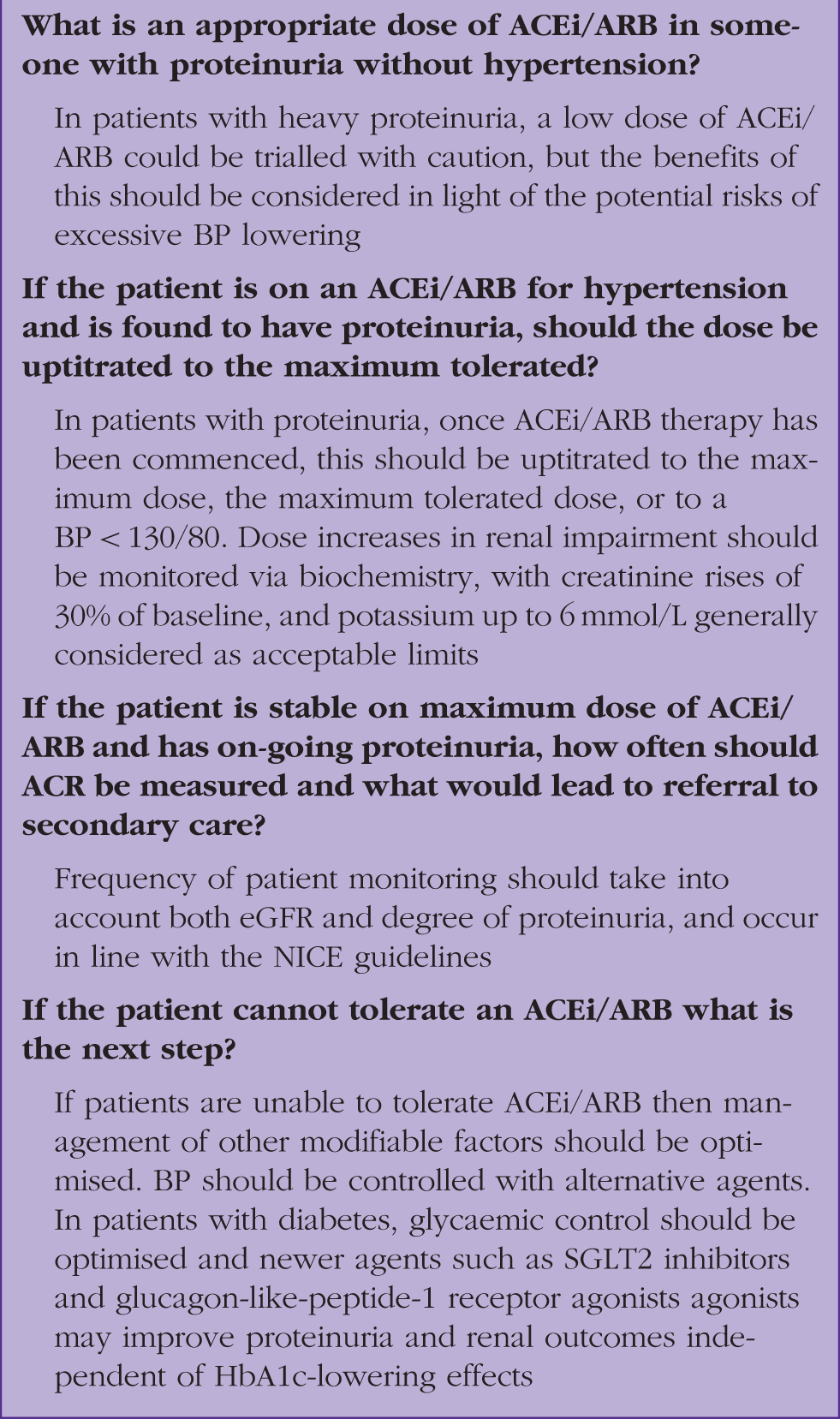
Troubleshooting and ACEi/ARB
Answers to queries about ACEi and ARB prescribing.
Glycaemic control
The landmark Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT) trial demonstrated the efficacy of intensive glycaemic control in reducing proteinuria in patients with type 1diabetes, and the UK Prospective Diabetes Study (UKPS) did the sme for types 2 diabetes. HbA1c targets should, however, always be individualised, taking into account other factors such as medication burden and risk of hypoglycaemia. More recently, sodium-glucose transporter protein 2 (SGLT2) inhibitors have shown impressive efficacy in reducing progression of proteinuria and renal impairment in diabetic kidney disease. Although perhaps not directly anti-proteinuria, these agents are recommended as second line therapy in patients with type 2 diabetes without contraindications and should be prioritised in patients with evidence of diabetic kidney disease (NICE, 2015b; Perkovic, 2019).
Supportive treatment
For all patients with CKD, treatment with a statin as part of primary prevention of cardiovascular disease should be offered without the need for formal risk assessment. Current guidance would dictate using atorvastatin at a dose of 20 mg (NICE, 2015a).
In addition, lifestyle modification should be supported given the association with cardiovascular risk. Smoking cessation, weight loss and exercise remain cornerstones of effective treatment.
Who should be referred to secondary care in the context of proteinuria?
Any patient with an ACR of 70 mg/mmol or more should be referred to secondary care, unless this occurs in the context of diabetes. The rationale for this approach is that this level of proteinuria raises the likelihood of a glomerulopathy and these patients may require nephrology review, an auto-antibody screen, and often a kidney biopsy, for further evaluation. Please note that the KDIGO guidance suggests considering referral to specialist care at a lower threshold of 30 mg/mmol as opposed to the NICE suggestion of greater than 70 mg/mmol.
Those with an ACR of 30 mg/mmol or greater with persistent haematuria after a urinary tract infection has been excluded should also be referred for similar reasons to above. Intuitively, an urgent nephrology referral is warranted if nephrotic level proteinuria (ACR greater than 250 mg/mmol) is detected.
Other cases should be considered on an individual basis and after consulting local referral guidance. A fictional case study is outlined to illustrate the potential pitfalls that can occur in primary care concerning proteinuria.
Case study 1
John, a 65-year-old patient has had a diagnosis of hypertension for 3 years. He is currently on monotherapy with amlodipine 5 mg. He has recently changed practice and has attended the practice nurse for a ‘new-patient’ review.
His BP in clinic is 158/96 mmHg in the best of three readings. You notice he has failed to attend for his annual BP review for the past 2 years. His final ACR at his last practice was 22 mg/mmol, but has not been repeated since this initial reading. He has a body mass index of 31 kg/m2.
John hands in a repeat early morning sample on two occasions with ACR of 25 mg/mmol and 29 mg/mmol, respectively. His urea and electrolyte (U&E) levels are tested and his eGFR is found to be 56 ml/min/1.73 m2. He is coded with a diagnosis of albuminuria on the computer system and commenced on an ACEi with ongoing BP monitoring. His U&E levels are monitored due to the ACEi treatment, but remain static at an eGFR of 54 ml/min/1.73 m2.
As a result of these findings John is diagnosed with CKD stage 3 and added to annual recall for optimised monitoring. His BP improves to 129/77 mmHg on treatment and he is commenced on statin therapy. John is keen to lose weight and is referred to a local organisation that will provide him with a supported exercise regime to help weight loss.
KEY POINTS
Primary care plays an important role in the identification and monitoring of CKD Primary care clinicians need to understand the relevance of the findings of albuminuria to the staging of CKD Adverse cardiovascular outcomes are a significant potential consequence of albuminuria Persistent albuminuria of greater than 3 mg/mmol is not a benign finding and should be acted upon and recorded appropriately within clinical coding systems Adequate BP control, glycaemic control, management of dyslipidaemia and treatment with ACEi or ARB form the mainstay of treatment of proteinuria and reduction in progression of proteinuric CKD as a result
ORCID iD
Dr Lauren Copeland https://orcid.org/0000-0001-9827-965X