
Abstract
Nephrotic syndrome is characterised by proteinuria, hypoalbuminaemia and oedema. The renal function is often normal and symptoms may mimic other common pathologies presenting in the community. The underlying aetiology is more heterogenous in adults compared with children, further confounding the diagnostic process and leading to delays in recognition. It is a relatively rare presentation in primary care, but the consequences of nephrotic syndrome can be significant. Complications include hyperlipidaemia, hypercoaguability, increased risk of infection and end-stage renal failure. It is, therefore, important to diagnose, investigate and manage nephrotic syndrome appropriately.
The RCGP curriculum and nephrotic syndrome
The role of the GP in the kidney and urology clinical topic guide is to:
Identify and manage acute kidney injury (AKI), including taking early action, such as stopping medications, to reduce the risk of AKI Be alert to possible indicators of urinary tract malignancy Know when to refer and when not to refer, avoiding futile investigation and escalation and encouraging supportive care Increasing awareness that a significant proportion of AKI starts in the community, so GPs have a key role in early identification and management Knowledge of typical and atypical presentations Identification of risk factors Recognition of diagnostic features and differential diagnosis Appropriate and relevant investigation Interpretation of test results
Emerging issues, knowledge and skills relevant to this article include:
Pathophysiology
Nephrotic syndrome is an overarching term to describe a heterogenous group of different disorders. Although there are several pathophysiological processes contributing to the phenotype, at the core appears to be glomerular dysfunction (Gupta et al., 2018). This leads to the classic triad of proteinuria (greater than 3.5 g/day in adults and greater than 40 mg/m2 in children), hypoalbuminaemia and oedema (Vivarelli et al., 2017). Patients with proteinuria in the absence of the other features have nephrotic-range proteinuria, usually attributed to underlying glomerular disease.
Proteinuria
The filtration of albumin by the glomerulus is usually restricted by its overall net negative charge and large size. Any albumin that does leak out is reabsorbed in the proximal tubule. In nephrotic syndrome there is a failure of this process, suggesting a problem with the glomerular filter. Abnormalities of podocytes and/or the slit diaphragm are thought to be responsible. Proteinuria itself will lead to tubulointerstitial inflammation and fibrosis, contributing to worsening renal function; proteinuria is also an independent risk factor for cardiovascular disease (Matsushita et al., 2010).
Hypoalbuminaemia
Proteinuria may contribute to the subsequent hypoalbuminaemia, but the liver should be able to produce sufficient albumin to compensate for these losses. There are a number of theories to explain the continued loss of albumin. For example, circulating cytokines may alter albumin production by the liver (Gupta et al., 2018).
Oedema
There are two broad hypotheses for the development of oedema in nephrotic syndrome (Gupta at al., 2018). The ‘underfill’ hypothesis is that low oncotic pressure secondary to hypoalbuminaemia leads to sodium and water retention in the extracellular space. Conversely the ‘overfill’ hypothesis suggests that the proteinuria leads to an increase in sodium, and thus, water resorption in the tubules.
Associated features
The reduced plasma oncotic pressure can lead to increased lipid metabolism in the liver, leading to hyperlipidaemia (Agrawal et al., 2018). There is also increased production of procoagulant factors, increased urinary loss of anticoagulant factors (antithrombin III) and a functional change in platelets, leading to a prothombotic state in patients with nephrotic syndrome, especially in membranous nephropathy (Mirrakhimov et al., 2014). The loss of immunoglobulins and complement through the leaky glomerulus can increase the risk of infection. The underlying pathology and proteinuria itself can also lead to acute kidney injury (AKI) and in some cases, end-stage renal failure if left untreated.
Aetiology
Causes of nephrotic syndrome.
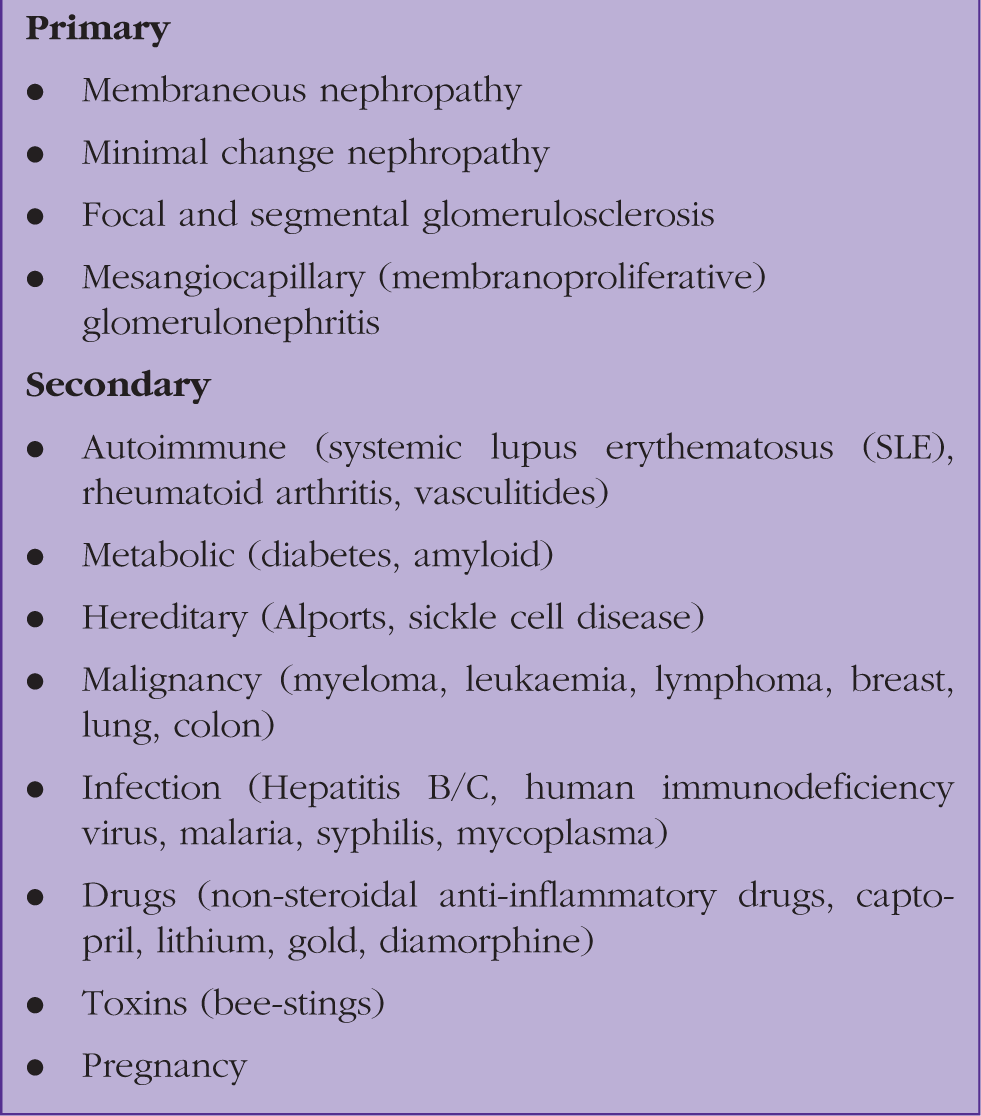
The main primary causes of nephrotic syndrome are minimal change disease (MCD), membranous nephropathy (MN), focal and segmental glomerulosclerosis (FSGS) and mesangiocapillary (membranoproliferative) glomerulonephritis (MCGN). MCD is more common in children, FSGS in young adults and MN in older patients.
Assessment
Presentation
Patient narrative.
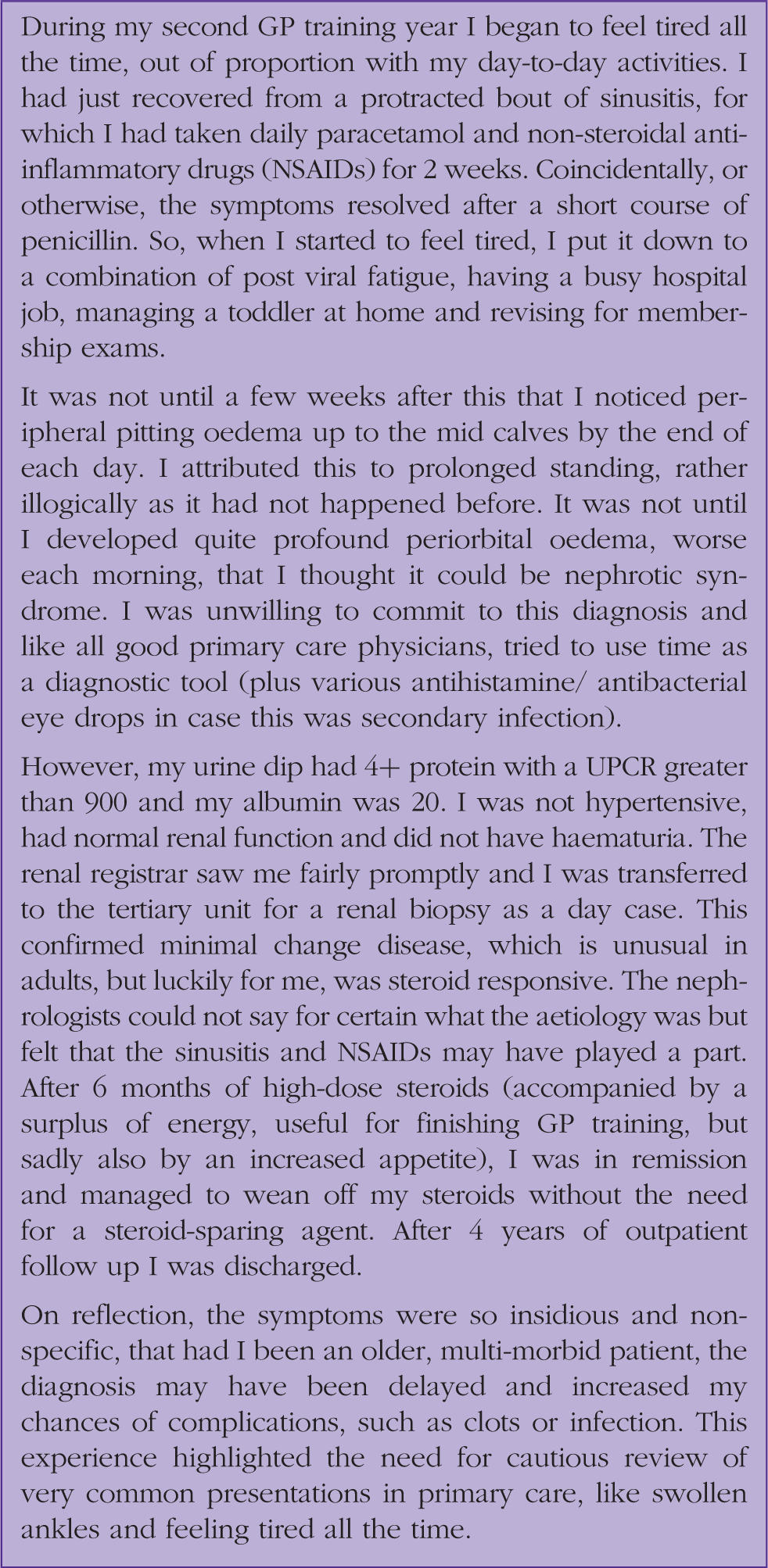
As in Box 2, many patients present with non-specific symptoms, or with the classic peripheral and periorbital oedema. If profound oedema is left untreated, this may progress to anasarca (gross generalised oedema with subcutaneous fluid accumulation and organ failure) and symptoms thereof. These include breathlessness from pleural effusions, heart failure or ascites, and symptoms and signs of AKI. Patients may also notice frothy urine secondary to heavy proteinuria (the detergent effect). The low albumin can manifest as leukonychia in the nails and tiredness.
If nephrotic syndrome is suspected, look for other clues that might point to a secondary pathology. For example, look for new rashes suggesting vasculitis or lupus. In an older patient with risk factors and constitutional symptoms, it is important to consider cancer. A family history in younger patients is useful as a number of renal diseases leading to nephrosis are congenital (Alport’s syndrome). A comprehensive drug history is also important, especially with nephrosis in the context of AKI.
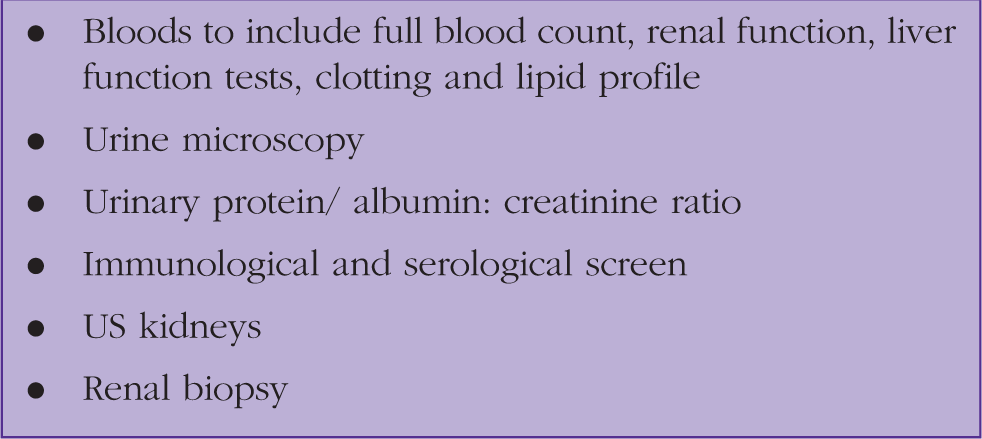
Investigation
Investigating nephrotic syndrome.
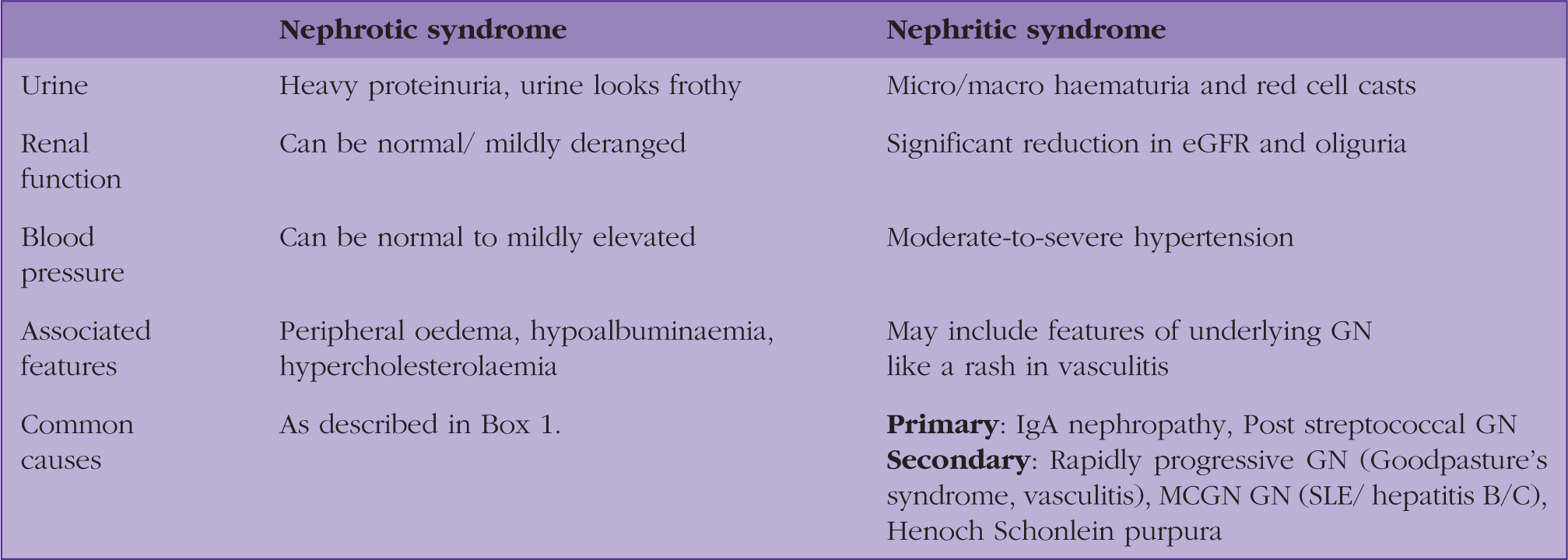
Nephrotic versus nephritic syndrome.
A spot test for protein-to-creatinine ratio provides sufficiently accurate information and is more practical than obtaining a 24-hour urine collection, which remains the gold standard.
All patients with nephrotic syndrome will require referral to nephrology, however, a discussion with the on-call nephrologist or paediatrician may be useful at this point to avoid delay in further management. Many adults may also require a renal biopsy to guide treatment. The majority of children with nephrotic syndrome hase idiopathic MCD and respond to steroids (Eddy and Symons, 2003). Therefore, they are less likely to need a biopsy, and would only require one if steroid resistant.
Principles of management
This is multifaceted and should be organised by the secondary care nephrology team. Its primary aims are to address the underlying aetiology (if there is one) and complications of nephrosis (Fig. 1). The oedema can be treated with salt restriction and diuresis with a loop diuretic (Gupta et al., 2018). For example, furosemide 40 mg once a day (OD) and titrate up to 250 mg OD. One should aim for a weight loss of 0.5 to 1 kg a day. If this is proving difficult to achieve and in profound oedema, the patient may need admission for intravenous diuresis to overcome oral malabsorption caused by gut oedema. Add on diuretics that act synergistically with high-dose loop diuretics are thiazide-types, such as metolazone (2.5–5 mg a day) (Crew et al., 2004), and should be used cautiously with regular blood tests to monitor for electrolyte disturbances. This combination, however, is not always successful and there are case reports of resistant oedema (Gupta et al., 2018).
Principles of management.
Proteinuria can be treated with angiotensin converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB) medications, which are also first line for hypertension in these patients (Matsushita et al., 2010). The risk for thrombosis is raised, especially with very low albumin less than 20 g/L or if the patient has underlying membranous nephropathy. Prophylactic low-molecular-weight heparin in high-risk patients may be an option and should be guided by the nephrologist, as there is no robust evidence currently available to recommend this action (Mirrakhimov et al., 2014). Treatment should only cease when the nephrosis is resolved. Patients are additionally at an increased risk of infection due to loss of immunoglobulins and complement through impaired glomeruli, however, there is no current consensus for the role of prophylactic antibiotics (Wu et al., 2012).
Minimal change disease
Minimal change disease is the most common cause of nephrotic syndrome in children (Eddy and Symons, 2003) and contributes between 15 and 25% of adult presentations (Vivarelli et al., 2017). The name is derived from the relatively minimal change seen on light microscopy of fixed tissue; electron microscopy is required to visualise the podocyte foot process effacement that characterises this disease. Although a biopsy is sometimes necessary in adults, this is rarely required in children. The aetiology is often idiopathic, but can also be secondary to medication such as non-steroidal anti-inflammatory drugs NSAIDS and antimicrobials, haematological malignancies and rarely infections such as tuberculosis or human immunodeficiency virus (HIV).
Beyond symptomatic treatment as described above, MCD is usually steroid responsive and the majority of adults will go into remission within 3 months (Kidney Disease: Improving Global Outcomes (KDIGO), 2012). Relapse rates are quoted as between 30 and 70%, and clearly those patients who have recurrent relapses will be more difficult to treat. In this event, the histology has to be reviewed to ensure the diagnosis is correct and other immunosuppressive agents can be considered such as ciclosporin or tacrolimus.
Membranous nephropathy
MN is the most common cause of non-diabetic nephrotic syndrome worldwide in adults, more prevalent in women between the fourth and sixth decades of life (Couser, 2017). Most presentations are idiopathic in nature and require a biopsy to guide treatment. Microscopy shows a thickened basement membrane with immunofluorescence highlighting granular IgG deposition in the capillary walls. Secondary causes include malignancy, which may or may not be preceded by nephrotic syndrome by several years; its development may also be the sign of a cancer relapse.
Management of both primary and secondary MN requires symptomatic treatment (Fig. 1) and for the latter, one should treat the underlying condition. For primary MN, one third of patients spontaneously remit, another third will have persistent mild proteinuria and the last third will progress to end-stage renal failure. For this reason, after diagnosis patients are observed for a short period to detect remission. If there is deterioration clinically or biochemically, disease-modifying treatment can be considered. Current advice is for a course of alternating monthly cycles of steroids with alkylating agents such as cyclophosphamide for 6 months, and evaluation of the response thereafter (KDIGO, 2012).
Focal and segmental glomerulosclerosis
FSGS is both a disease process and histological diagnosis describing sclerosis of parts (segmental) of some (focal) of the glomeruli (NICE, 2016). Primary (idiopathic) FSGS is the main cause of nephrotic syndrome in black patients, for whom there is a worse prognosis as compared with other ethnicities. They can also present with heavy proteinuria. It can recur in transplanted kidneys and may be associated with hypertension, renal dysfunction and microscopic haematuria (D'Agati et al., 2011). Although secondary FSGS presents with less hypoalbuminaemia and proteinuria, it is more likely to lead to chronic hidney disease. Causes include infection, like HIV, and any cause of progressive renal scarring such as vasculitis or pre-eclampsia.
Almost half the patients will progress to end-stage renal failure if left untreated. The mainstay of treatment for primary FSGS causing nephrotic syndrome is steroids, bearing in mind that FSGS is slower to respond than, for example, MCD (NICE, 2016). Patients usually require a minimum of 4 weeks treatment. Those that do not respond to this can be considered for calcineurin inhibitors such as ciclosporin or tacrolimus. Rituximab may also be an option for refractory cases, however, the recommendations are drawn from observational studies with low participant numbers (NICE, 2016). Secondary FSGS will not be as steroid responsive and requires reduction in intraglomerular pressure and treatment of the underlying cause (D'Agati et al., 2011).
Mesangiocapillary (membranoproliferative) glomerulonephritis
This term describes the histology found on renal biopsy of these patients: intense glomerular hypercellularity due to mesangial proliferation and glomerular basement membrane thickening (Sethi and Fervenza, 2012). As with the above causes of nephrotic syndrome, this can be a primary and idiopathic pathology, or associated with another illness, like an infection (HIV, hepatitis C or malaria) or Systemic lupus erythematosis. There are currently no evidenced-based treatment options for MCGN although immunomodulation with steroids and monoclonal antibodies may have a role in management (Sethi and Fervenza, 2012).
KEY POINTS
Nephrotic syndrome is caused by a diversity of disease processes and can present non-specifically and/or similar to common pathologies seen in primary care It is a rare, but important, presentation of kidney disease with serious complications that include thrombosis, infection and renal failure Investigation focuses on finding the underlying aetiology Management is multifaceted focusing on symptom management and ensuring that any underlying aetiology if found, is treated All patients require referral to the nephrology team and may require a renal biopsy