
Abstract
Medication-related osteonecrosis of the jaw (MRONJ) is a rare, but well-documented, complication following the administration of anti-resorptive and anti-angiogenic drugs. MRONJ has a negative effect on quality of life, and can result in reduced social contact, pain and masticatory difficulties. Prescription of implicated medication is within the remit of GPs, and thus National Institute for Health and Care Excellence (NICE) guidelines have been published to inform prescribing. Careful consideration of the potential deleterious oral side-effects of these drugs is needed. NICE guidelines on the prescribing of bisphosphonates for osteoporosis acknowledge that osteonecrosis of the jaw was not included in the adverse events when the economic model was assessed. This article provides an overview of MRONJ, highlighting key areas for possible GP intervention when caring for patients at risk of developing MRONJ, and what to do if MRONJ is suspected.
The RCGP curriculum and osteonecrosis of the jaw
The role of the GP in the ear, nose and throat, speech and hearing clinical topic guide includes:
Identify symptoms that fall within the range of normal or are caused by self-limiting conditions Know the epidemiology and understand how to recognise oral, head and neck cancers including the risk factors, and identify unhealthy behaviour, as well as being able to refer appropriately Perform effective assessment including conducting or interpreting more detailed tests and treatment including procedures where indicated Demonstrate empathy and compassion towards patients with ear, nose and throat (ENT) symptoms that may prove difficult to manage, e.g. tinnitus, facial pain, unsteadiness, hearing loss Offer smoking cessation advice and treatment Head and neck cancer rates are increasing, and outcomes depend on early diagnosis Guidelines for appropriate management are now widely available, but not always used
This article considers some emerging issues in the care of people with ENT and mouth problems:
Defining and diagnosing medication-related osteonecrosis of the jaw
When diagnosing a patient with medication- related osteonecrosis of the jaw (MRONJ), all of the following five criteria need to be satisfied (Ruggiero et al., 2014):
The patient presents with exposed bone, or bone that can be probed through a fistula: Either intra-orally, or extra-orally The bone has been exposed for at least 8 weeks within the maxillofacial region The patient has a history of using anti-resorptive or anti-angiogenic drugs There is no patient history of head and neck radiotherapy There is no recognisable metastatic disease to the head and neck region
Pathogenesis of MRONJ
The exact pathogenesis of MRONJ is not fully understood. Current theories implicate suppressed bone turnover, infection, inflammation and the inhibition of angiogenesis (Ruggiero et al., 2014). Current theories cannot determine whether infection precedes necrosis of the bone or vice versa (Khan et al., 2015). There is also evidence that genetic mutations may predispose patients to MRONJ (Marini et al., 2011).
Medication and risk factors for MRONJ
Common drugs implicated in MRONJ.
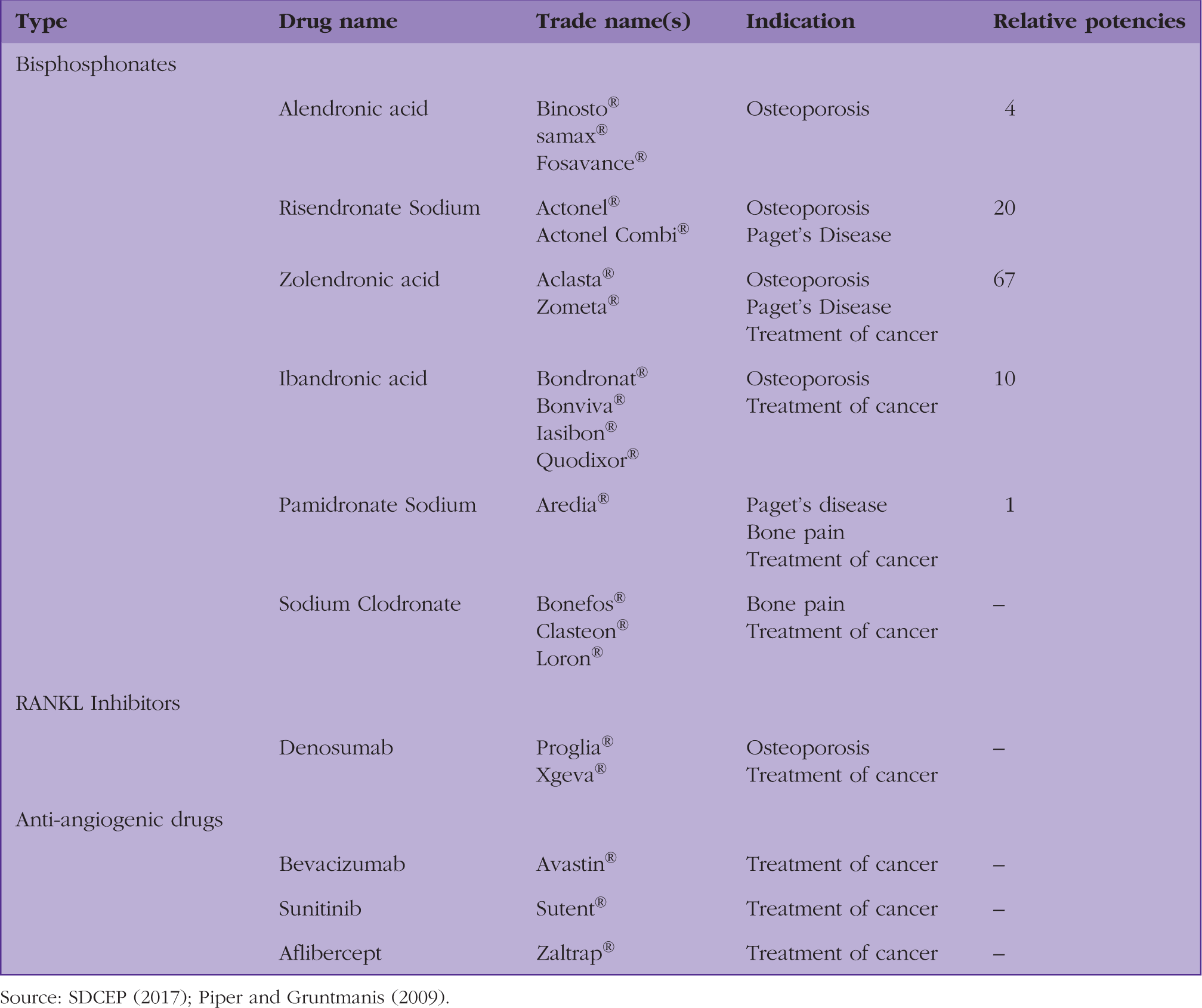
Source: SDCEP (2017); Piper and Gruntmanis (2009).
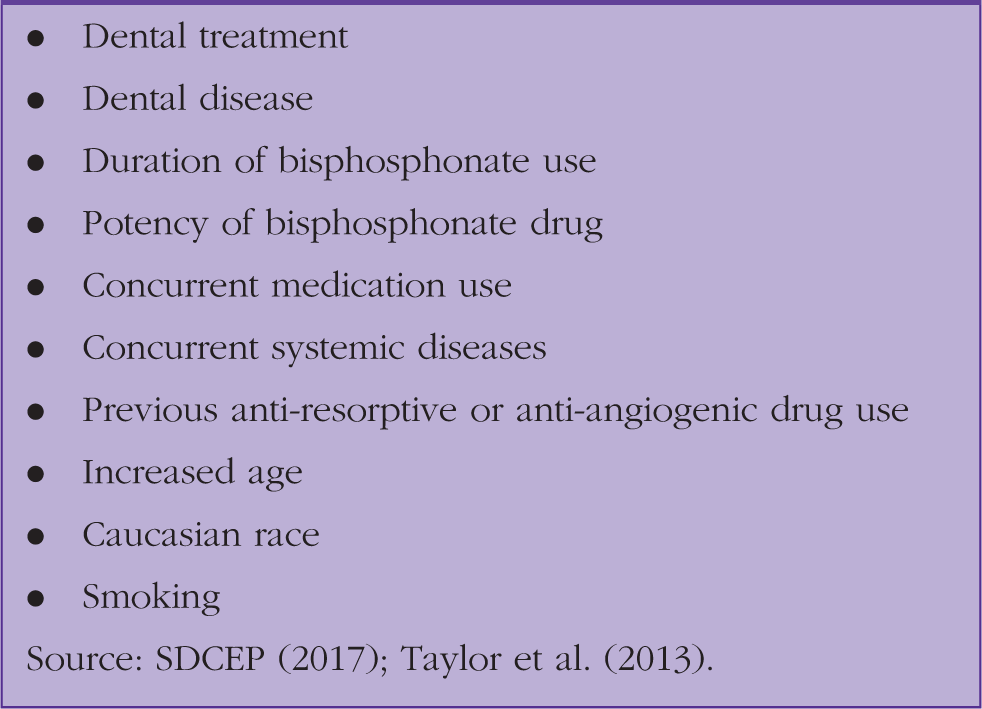
Risk factors for developing MRONJ.
Dental treatment and dental disease
Dental treatment is a known risk factor for developing MRONJ (Marx et al., 2005). Treatments that impact on the bone, or its healing, are those most commonly implicated as being risk factors including dental extractions. Mucosal trauma can also result in MRONJ, often precipitated by ill-fitting dentures or dental trauma. Dental disease, such as gum disease and infection associated with a non-vital root canal system (or dental pulp tissue), has also been implicated as a risk factor (Thumbigere-Math et al., 2014). However, MRONJ can develop spontaneously, without any precipitating dental treatment (SDCEP, 2017).
Medication type and duration
Bisphosphonates work by disrupting osteoclastic activity. They have a lengthy half-life, for example, the half-life of alendronic acid is approximately 10 years (Kahn et al., 1997). Therefore, the greater the duration of treatment with bisphosphonate medication, the higher is the risk of developing MRONJ. This has been found to be the case in patients taking oral alendronate (Lo et al., 2010).
As cumulative dose is pivotal in assessing risk, a drug’s relative potency needs to be taken into consideration. More potent medications, such as zolendronate or risedronate confer a higher risk of developing MRONJ in susceptible patients. The relative potencies of different bisphosphonate medications can be seen in Table 1.
Denosumab also exhibits osteoclastic function and has similar indications for use as bisphosphonates. It is normally injected on a 6 monthly basis, subcutaneously. It does not bind to bone constituents, unlike bisphosphonates, and therefore, the actions reduce after 9 months.
Concurrent medication use
There is an increased risk of MRONJ if a patient takes anti-resorptive medications, as well as anti-angiogenic ones (Saad et al., 2012). The latter category of drug is prescribed primarily for treatment of cancer. These drugs work by inhibiting the formation of new blood vessels. Specifically, those drugs targeting vascular endothelial growth factor and receptor tyrosine kinase are implicated in MRONJ. There is also an increased risk in patients who are taking systemic glucocorticoid medication (Saad et al., 2012; Taylor et al., 2013).
Incidence of MRONJ
The incidence of MRONJ is affected by the indication for anti-resorptive or anti-angiogenic medications. Oncology patients who have been prescribed them for management of their tumours will typically be prescribed higher potentcy drugs. Consequently, the incidence of MRONJ is higher. Considering evidence from systematic reviews and appropriately conducted randomised controlled clinical trials, the incidence of developing MRONJ in this cohort of patients is 1%. This is an estimated value, and this may vary on the drug administered, and the cancer for which the patient is being treated. There is less published literature on the use of anti-angiogenic medication, and the current incidence in this group is estimated, for example, to be 0.2% in patients treated with bevacizumab (Guarneri et al., 2010).
Those taking oral anti-resorptive medications for osteoporosis are at a much lower risk of developing MRONJ, and this is reflected in the lower incidence in these patients. Within the UK, the incidence of MRONJ in these patients is estimated at between 0.0001% and 0.001% (Rogers et al., 2015). Studies specifically investigating the role of oral alendronate on MRONJ put the incidence at 0.043% (Sammut et al., 2016). SDCEP guidelines (SDCEP, 2017) estimate the incidence of MRONJ in patients treated with anti-resorptive drugs for osteoporosis at 0.01 to 0.1%.
Presentation of MRONJ
Staging of MRONJ.
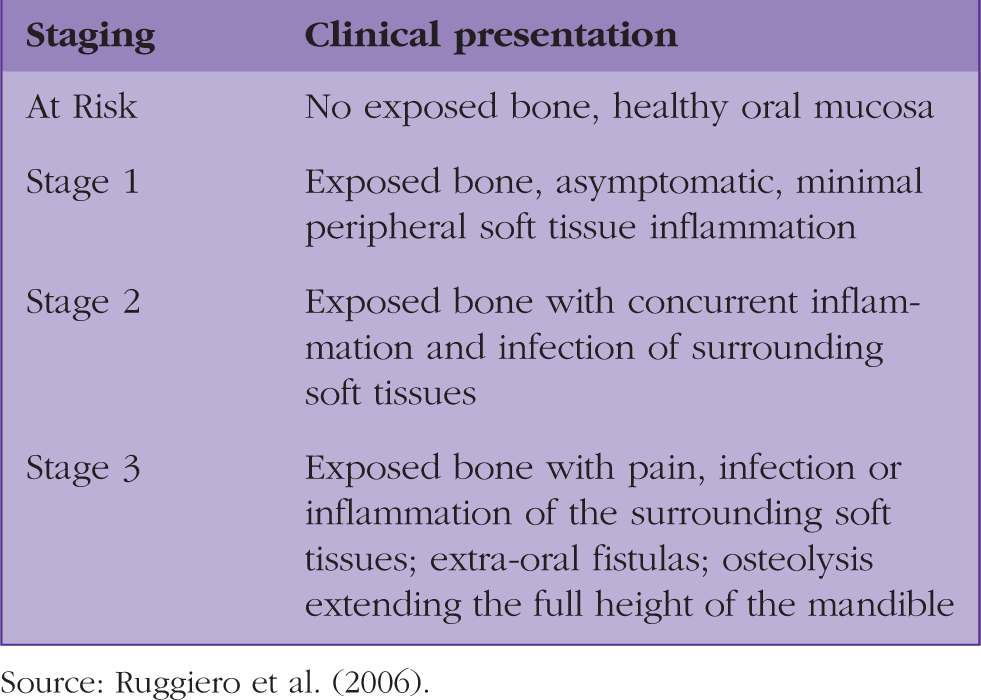
Source: Ruggiero et al. (2006).
The GP’s role in preventing MRONJ
GPs can deliver key information to patients to prevent MRONJ and ensure that those at risk of developing it seek appropriate advice and treatment. GPs should encourage those who are due to start any course of treatment predisposing to MRONJ to seek a dental care assessment. Confirmation of assessment and any outstanding dental treatment can then be provided by the patient’s dentist prior to beginning anti-resorptive or anti-angiogenic drug therapy. Figure 1 provides a flow diagram to help GPs in their efforts to decrease the incidence of MRONJ. Working with colleagues in the best interests of the patient is a General Medical Council (GMC) duty (GMC, 2014).
Flow diagram to aid GPs in reducing patient's risk of developing MRONJ.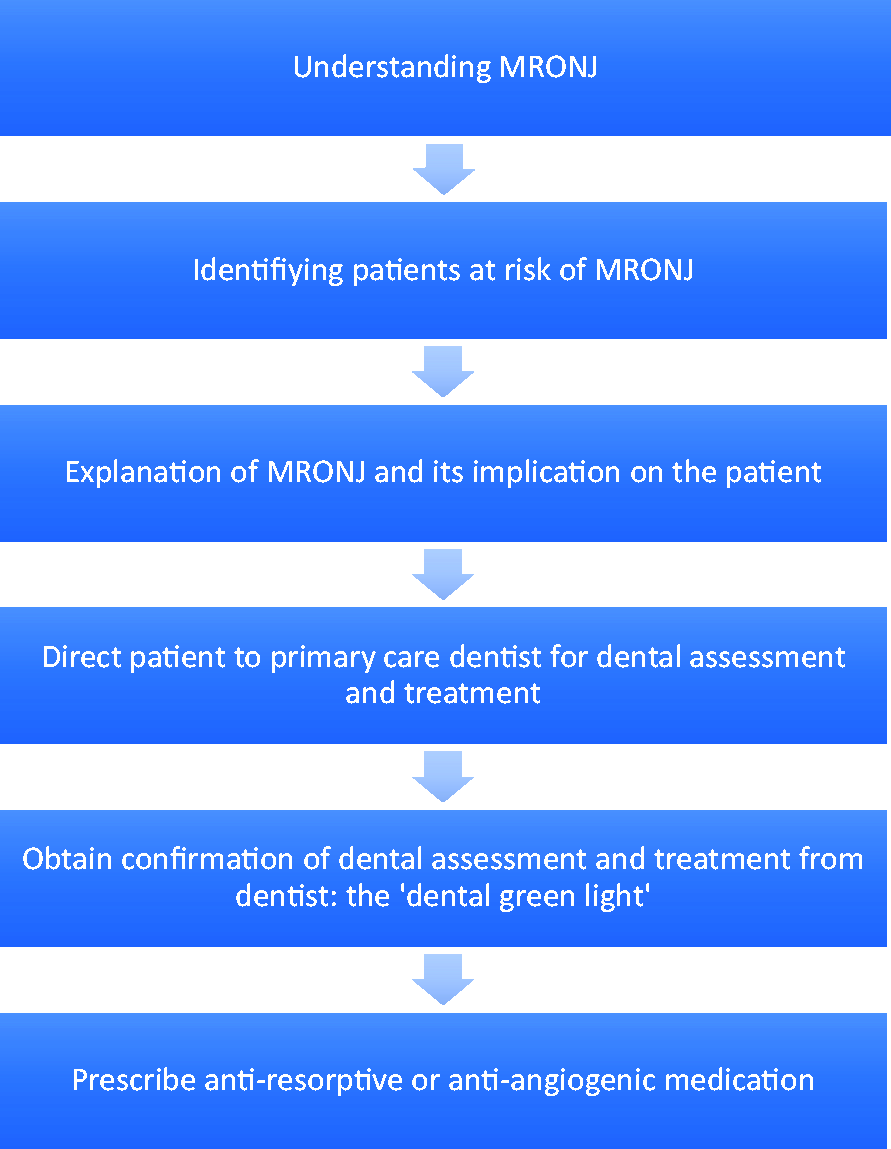
Prevention is at the core of any dental intervention and this includes minimising a patient’s risk of developing MRONJ. There are two main dental diseases requiring dental treatment: gum disease and dental decay. Dental extraction can be a treatment option for these dental pathologies. In a patient on any of the drugs highlighted in Table 1 dental extraction can result in MRONJ.
Dental preventative advice that can be delivered by GPs.

Management of patients presenting with MRONJ
The management of patients presenting with MRONJ depends on the severity and classification of MRONJ. Table 2 indicates the staging of MRONJ. Currently, there is no definitive treatment protocol for patients presenting with MRONJ. Treatment options range from conservative management with observation, to surgical intervention.
A patient presenting with signs and symptoms of MRONJ should be referred to specialist oral and maxillofacial services (OMFS) for assessment and subsequent treatment. A clear and comprehensive patient history should be undertaken to exclude a working diagnosis of metastatic disease or ORN. For asymptomatic MRONJ (Stage 1), the GP can advise the use of anti-bacterial mouthwash (for example chlorhexidine) and give oral hygiene instruction. This will hopefully aid soft-tissue healing. Stages 2 and 3 MRONJ can be managed by the GP in a similar manner, but with the addition of systemic anti-microbial therapy, for example with co-amoxiclav or amoxicillin. In all cases, a referral to specialist services via local pathways should be made. Furthermore, GPs should aim to report any suspected case of MRONJ to the Medicines and Healthcare products Regulatory Agency.
Associated acute or spreading oro-facial infection or suspected pathological fracture will require contact with the local OMFS team and may require urgent referral. In such circumstances, patients should be informed of the rationale for their urgent referral to the hospital and be kept nil-by-mouth until (if) their medical history permits. Patients should be given a comprehensive list of their current medication and formal medical diagnoses for the OMFS team to inform the admission process. A flow diagram that summarises modalities of appropriate referral based on patient presentation can be seen in Fig. 2.
Referral flow diagram.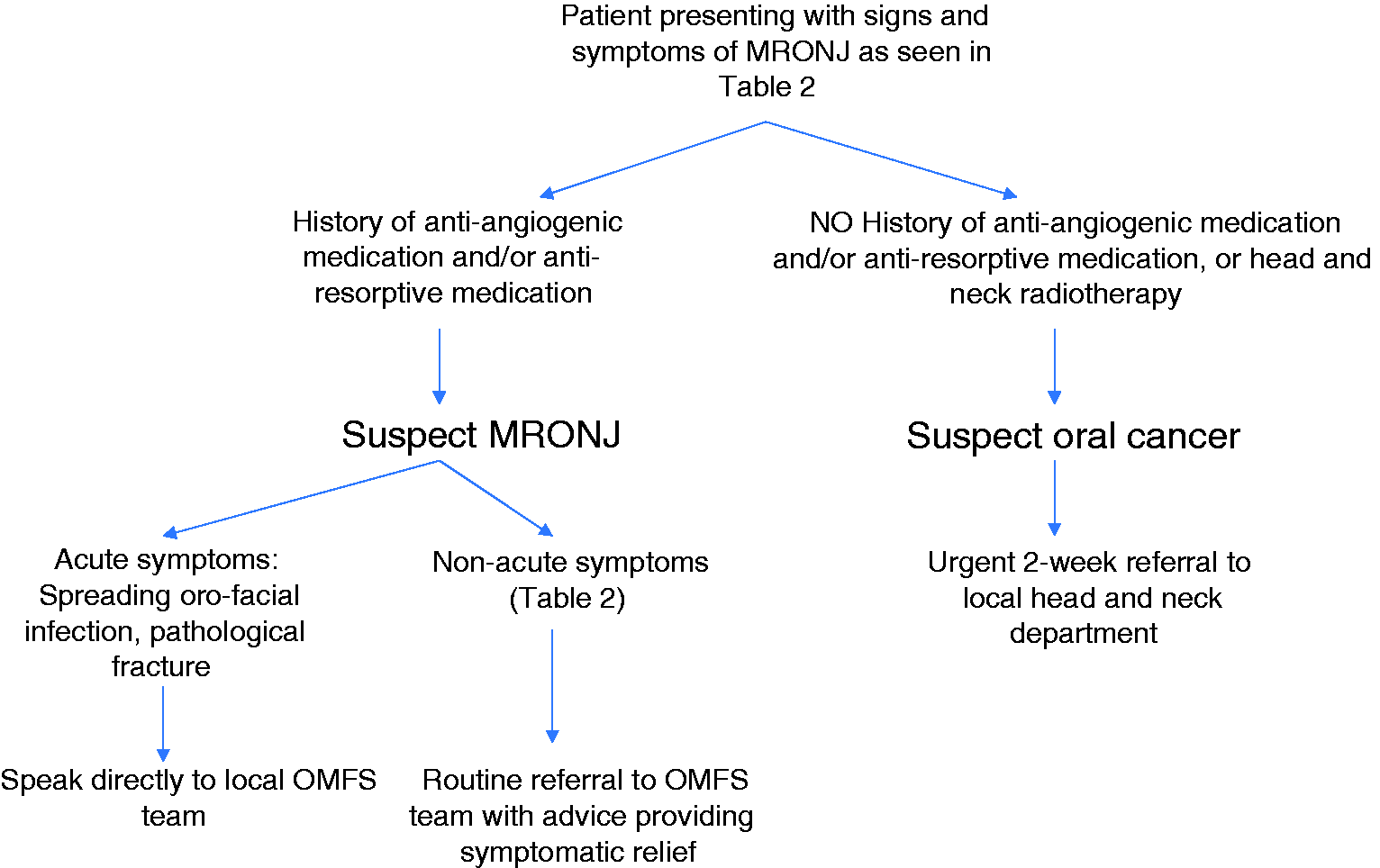
Treatment of MRONJ
Treatment of MRONJ will typically be undertaken by the OMFS team. Some units have dedicated multi-disciplinary team MRONJ clinics that may include an oral surgeon, oral and maxillofacial surgeon, special care dentist and a restorative dentist. Treatment of acute symptoms is of primary importance. The majority of cases are treated conservatively. This may not resolve the lesions entirely, but may provide long-term symptomatic relief for the patient (Saad, 2012). Additional medication, such as pentoxyphylline and tocopherol can be added to antibiotic therapy to manage such lesions (Epstein et al., 2010). Conservative management should be continued as long as there is no progression of signs or symptoms of MRONJ.
If symptoms are worsening on a conservative management regime, surgical intervention may be indicated. This may include resection of necrotic bone, with adequate margins extending onto normal bone. Careful osteoplasty needs to be undertaken to ensure the bony contour is smooth, minimising any subsequent wound breakdown. Tension-free primary closure should be achieved. In some cases, microvascular surgery may need to be undertaken to optimise success of surgical intervention.
Conclusion
The reasons for prescribing anti-resorptive medication by GPs are well documented, and guidelines have been published to standardise its administration (National Institute for Health and Clinical Excellence (NICE), 2012; 2017). The benefits of prescribing bisphosphonates are significant, but they do come with well-documented oral risks. Patients who have been diagnosed with MRONJ will have long-term follow-up with the unit managing their MRONJ. It is vital for GPs to be vigilant and refer to onwards services appropriately while continuing to reinforce preventative advice and to ensure symptoms of MRONJ, if already diagnosed, do not worsen.
GPs should be aware of MRONJ as a potential side-effect of prescribing anti-resorptive and anti-angiogenic drugs, and should appropriately risk assess patients prior to their prescription.
KEY POINTS
A variety of medications pre-dispose patients to MRONJ GPs should deliver appropriate advice to minimise the incidence of MRONJ in patients on anti-resorptive or anti-angiogenic drugs GPs should seek a ‘green light’ from the dentist prior to prescribing anti-resorptive or anti-angiogenic drugs GPs should refer cases of MRONJ to their local OMFS unit for further assessment and treatment