
Abstract
It is well-known that people with an intellectual disability often face a host of health inequalities and co-morbidities. These include childhood obesity, mental health problems, and challenging behaviour. People with an intellectual disability also have reduced life expectancy. GPs are uniquely placed to advocate for and signpost these patients, ensuring they have access to appropriate support. However, it is often unclear what resources are, in reality, both available and beneficial. Here we aim to summarise some of the common inequalities and complexities when working with patients with an intellectual disability and provide an overview of some potentially helpful services.
The RCGP curriculum and services for people with an intellectual disability
The role of the GP in the neurodevelopmental disorders, intellectual and social disability clinical topic guide is to:
Identify, monitor and review all patients who have difficulties with communication, social relationships and managing their own affairs; this may require additional skills in diagnosis, examination and consultation, and an understanding of legislation and guidance on mental capacity Carry out annual health checks for people with intellectual disability Signpost patients and their families or carers to appropriate resources, knowing when and where to seek specialist help Advocate for people with intellectual and social disabilities; promote fairness and equity in the community, including equal access to healthcare Diagnostic features and genetic causes of intellectual disability Common associated physical health disorders and mental health problems Annual health checks Secondary care and specialist services
The RCGP curriculum outlines knowledge and skills topics that may be relevant for GPs working with patients with intellectual disabilities. This paper will address the topics listed below:
Terminology
Since the inception of psychiatric nosology, various terms have been used to describe conditions affecting cognitive and adaptive functioning. Some of these are now considered at best outdated and at worst stigmatising. Throughout this article, we will use the initialism (ID) to refer to an ‘intellectual disability’, reflecting the language used in the RCGP curriculum. In the UK, and elsewhere, many specialist services and indeed patients and families use the term ‘learning disability’. Despite sounding similar, there is a firm distinction between ‘learning disabilities’ and ‘learning difficulties’, the latter being an umbrella term used to describe the broad spectrum of conditions which impact a specific area of learning such as literacy (dyslexia) rather than cognitive development or ‘intellect’ and adaptive functioning as a whole. Understanding this distinction may be a challenge for patients, families, and professionals alike. Therefore, it is important that GPs have a strong grasp of each group when making referral decisions.
Definition, aetiology and prevalence of ID
An ID is a neurodevelopmental condition that begins in the developmental period and is characterised by atypical cognitive development and differences in conceptual, social or practical adaptive functioning that are two or more standard deviations below the population mean (World Health Organisation, 2019). In the UK, the legal definition of disability comes from the Equality Act (2010), wherein differences in adaptive functioning are considered a core feature of disability. For ID specifically, the General Medical Services contract Quality and Outcomes Framework (NHS, 2019a) describes ID by three criteria: an intelligence quotient of less than 70, impairments in social or adaptive functioning, and onset in childhood. However, it is important to note that the range and severity of cognitive and functional differences are diverse. In an attempt to describe this diversity, psychiatric nosologies use terms such as ‘mild’, ‘moderate’, ‘severe’ and ‘profound’. Most people (approx. 85%) with an ID fall under the categories of mild to moderate (Boat and Wu, 2015). Many of these patients are able to live independently though may require some additional support (e.g. when making health or legal decisions). People with a severe ID, in contrast, may require greater support with tending to care needs and may need a flexible approach to communication. People in the ‘profound’ category often require assistance with all aspects of care and might also have difficulties with symbolic communication and reasoning. However, it is essential that all decisions regarding support be made on an individual basis rather than on the category of functioning, using appropriate approaches to allow the patient and their family to indicate preferences and make choices.
The aetiology is diverse, ranging from birth complications, prenatal substance exposure, brain injury and severe neglect, to genetic syndromes. It is estimated that in 60% of people with an ID, the genetic aetiology can now be established (Vissers et al., 2017). Such genetic aetiologies include Trisomy 21 (Down’s syndrome), paternal 15q11-q13 deletion (Prader–Willi syndrome), XXY (Kinefelter syndrome) and many others. Parents and patients might also benefit from support groups such as hwww.rarechromo.org. Some syndromes associated with ID have specific patterns of cognitive and general abilities associated with them although show considerable individual variation among individuals (Mulder et al., 2017).
In England, it has been estimated that there are 1 087 100 people with ID (Public Health England, 2015). This figure stands in stark contrast with the number of people with an ID on GP registers, which is approximately 252 446 (Public Health England, 2015). This equates to 4.4 people with ID per 1000 people registered with a GP (Public Health England, 2015). Speculating on the causes for these discrepancies, Public Health England (2015) suggests that one factor may be that people tend to use GP services sporadically. However, this is cause for concern considering that free annual health checks are recommended for everyone over the age of 14 years with an ID (Public Health England, 2016). Another explanation offered by Public Health England (2015) is that the majority of adults with an ID are not known to ID services. In support of this claim, Public Health England cites national prevalence figures that show a marked difference between the numbers of children with an ID in the education system (2.5%) and the number of people in their twenties known to services (around 0.6%). Such a distinct drop-off, it is reasoned by the national body, might be due to increased thresholds for entry to adult specialist health and social care services, or less obvious impairments in non-educational settings. Nevertheless, there are signs that things are moving in a positive direction. That is, the numbers of people with an ID on GP registers has been growing at a rate of around 5% per year. This is likely the result of non-aetiological factors such as more accurate record-keeping. Still, it is consequential that many patients with an established ID may not have this marked in their health records or making use of potentially important or beneficial services.
Health inequalities/multi-morbidity
Overview
Previous work has established that people with an ID and associated conditions often face a number of health inequalities across the lifespan relative to typically developing peers. Such disparities might include greater risk of respiratory problems (Chang et al., 2017) and a reduced life expectancy (Thornton, 2019). In an analysis of 1 424 378 primary healthcare records, Cooper et al. (2015) identified a number of physical health co-morbidities which were more prevalent in people with an ID relative to people without an ID. These included epilepsy (odds ratio = 31.03), constipation (odds ratio = 11.19), and visual impairment (odds ratio = 7.81). However, it is important to note that the extent to which these outcomes will be expressed may be more or less linked to genetic aetiologies. That is, certain conditions (e.g. Prader–Willi syndrome or Down’s syndrome) might confer a particular risk of said co-morbidity (e.g. obesity).
Regarding mortality, in a review of the deaths of 247 people with IDs, Heslop et al. (2014) reported that the median age of death for men and woman with an ID is, respectively, 13 years and 20 years lower than that in the general population. Moreover, 37% of these deaths were classified as ‘avoidable’ through good quality healthcare. The percentage of avoidable deaths in the general population is approximately 13% (Heslop et al., 2014). Such alarming findings underscore the importance of annual health checks in this population. These checks are recommended for anyone aged 14 years or older who has an established ID (Public Health England, 2016). However, in 2017–18 only just over half of patients with an ID received their annual health check (Thornton, 2019). The RCGP offers a step-by-step guide to conducting these checks (RCGP, n.d.). This guidance covers a range of topics relevant to both physical and mental health. Helpfully, this guide also offers a number of practical communication tips, which have been developed in conjunction with a patient with an ID. In a systematic review, Robertson et al. (2011) concluded that health checks are an effective method of recognising previously unidentified health problems in this population. Health checks are thus an evidence-based and effective service that GPs can offer their patients with an ID.
Mental health problems
Like anyone else, people with an ID can experience psychiatric illness, such as depression or anxiety disorders. Common symptoms of these conditions include feelings of low mood, isolation, or anxiety. In contrast, conditions such as autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), and indeed ID are lifelong developmental differences. Grasping this distinction is important for a number of reasons, not least because it helps practitioners understand the configuration of service pathways and decision-making in prescribing.
Due to methodological variation between studies, there is a range of reports of the co-morbidity of ID and mental health problems. Nevertheless, the available research strongly indicates that children with an ID experience rates of mental health problems that are comparable to, or higher than, neurotypical peers (Einfeld et al., 2011). Similar findings also extend to adults and adolescents with an ID, with recent meta-analytic evidence estimating 33% co-morbidity (Mazza et al., 2019). Cooper et al. (2015) also describe specific co-occurring mental health conditions that people with an ID experienced relative to people without an ID. These include schizophrenia (odds ratio = 7.16), anxiety or other stress disorders (odds ratio = 2.62), dementia (odds ratio = 2.22), and depression (odds ratio = 1.88). Best practice guidelines thus recommend that a mental health review be completed as part of the patient’s annual health check (National Institute for Health and Care Excellence (NICE), 2016). The markers of a potential psychiatric disorder in people with an ID are very varied, and include loss of skills, social isolation, avoidance, challenging behaviour, or loss of interest in activities the individual previously enjoyed (NICE, 2016). It is important to note that autism and ADHD, without ID, are themselves associated with increased psychiatric co-morbidity.
Challenging behaviour
Challenging behaviour is also more common in people with an ID (Emerson and Baines, 2010). Challenging behaviour is typically defined as: culturally abnormal behaviour(s) of such intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit the use of, or result in them being denied access to ordinary community facilities (Emerson, 1995, p. 4).
In response, and as part of a wider national agenda to improve care for persons with an ID, the ‘stopping over medication of people with a learning disability, autism or both with psychotropic medicines (STOMP)’ project was established (NHS England, n.d.). At the heart of this project is a collaboration between NHS England and other professional organisations including the RCGP, The Royal College of Psychiatrists and The Royal Pharmaceutical Society. The core aims are as follows:
Promote regular check-ups about medication Ensure professionals involve patients and families in decision-making about medications Inform all key stakeholders about alternative modes of intervention and responding to challenging behaviour (e.g. Positive Behavioural Support)
It is, therefore, important that practitioners are aware of the various functions of challenging behaviours. That is, these behaviours very often serve a communicative or sensory function (NICE, 2015). Moreover, the behaviours may be contextual or environmentally specific. NICE (2015, p.15) thus recommends that antipsychotic medication should only be offered if:
Psychological or behavioural interventions have not been effective Treatment of any co-morbid condition (psychiatric or otherwise) has not reduced the behaviour There is significant risk to the safety of the individual or others
The guidance goes on to state that these medications should only be offered in conjunction with psychological or other interventions. Further guidance and information on prescribing in primary care can be found in the RCGP annual health checks guide.
Diagnostic overshadowing
The now-popular clinical phrase ‘diagnostic overshadowing’ has its provenance in early ID research. It is used to refer to situations where a symptom is misattributed to the patients' ID. This occurs throughout medicine, but is particularly relevant in patients with an ID when there is a well-documented and dangerous tendency for co-morbidities, such as constipation, epilepsy, and infection, are not sought as reasons for changes in behaviour. This can be fatal. Healthcare professionals thus have a moral ethical and professional responsibility to ensure that a patient’s diagnosis of ID does not mean that they miss symptoms of underlying medical conditions. For instance, challenging behaviour in the form of head-banging might be how the individual expresses that they have a toothache, constipation, seizures, depression, sepsis, or brain tumour. This is a significant contributor to avoidable death in people with an ID (see Learning Disability Mortality Review (NHS, 2019b)).
This can occur in the other direction, with ID not being sought due to other issues such as ASD or epilepsy. Therefore, GPs and other healthcare professionals also need to keep in mind that some patients with an ID may reach adulthood without a diagnosis. Given the nature of general practice, GPs are often well-placed to offer colleagues in other services a holistic view of the patient’s physical and mental health. This level of insight can be used in practice to safeguard against possible diagnostic overshadowing in both primary care and specialist services.
Service provision
Context
In the 1970s, several clinical initiatives were established with the goal of replacing institution-based services for persons with mental health difficulties and or ID with community-based options (Killaspy, 2007). Consequently, much of the responsibility for meeting the social and healthcare needs of such patients was gradually transferred to community-based teams. Often, however, community services were under-resourced and unable to respond to some of the specialist needs of this population. This resulted in many of these patients experiencing long stays in inpatient settings. In 2011, this issue came to the fore following the airing of the BBC Panorama documentary featuring Winterbourne View Hospital. This programme highlighted significant emotional and physical abuse committed by some staff against patients who had an ID. Although the abuse was obviously abhorrent, it was also of great concern that patients with an ID were spending long periods in inpatient units, rather than in the community. In response, the Department of Health (2012) developed the ‘Transforming care’ plan wherein it pledged: all current placements will be reviewed by 1 June 2013, and everyone inappropriately in a hospital will move to community-based support as quickly as possible, and no later than 1 June 2014 (p. 9).
Unfortunately, however, this target was missed (Bubb, 2014).
Ultimately and despite the abuse uncovered at Winterbourne View Hospital, public outrage and subsequent policies and programmes, the numbers of patients with an ID in inpatients units in the UK has remained at a similar level. Health and social care services for people with an ID are still not delivering appropriate and timely support to enable people to lead flourishing lives in their local communities. It is the responsibility of all stakeholders, including GPs to ensure that whenever possible the needs of these patients are met in community-based settings that promote opportunities for inclusion, choice, and autonomy in a supportive environment. Moreover, frontline healthcare professionals, such as GPs, may be able to advise patients and families about the services available locally. GPs are also uniquely placed, given professional expertise and authority, to advocate for these patients both individually and at policy level.
‘Reasonable adjustments’
Independent groups.
Recently, the organisation Dimensions conducted a survey of 252 GPs about their experiences caring for people with an ID (Dimensions, 2018). The results indicated that 48% of GPs were unclear when to make a ‘reasonable adjustment’ and 74% suggest that they would benefit from further training. This suggests some training on ‘reasonable adjustments’ may be beneficial. The survey also showed that 64% of GPs surveyed had less than 1 day’s face-to-face training focused on responding to the needs of patients with an ID. Also around 98% indicated that they would like more training. Such training is available through charities and advocacy groups such as Dimensions or British Institute of Learning Disability (BILD). For a useful and accessible report on making reasonable adjustments see Turner and Robinson (2011).
Services for people with an ID across the lifespan
When deciding which services may be beneficial for patients with an ID, it is important to consider the nature of the ID (i.e. mild, moderate, serve, or profound) and the age of the patient.
Early intervention can be beneficial for some children with an ID, particularly in supporting carers and schools to understand and manage communication via behaviour, and in early identification and treatment of co-morbidities. However, there is some geographical variation in the services that are available locally. Organisations such as the Early Intervention Foundation offer information regarding such services (see Table 1 for details). Nevertheless, it is crucial that GPs understand the configuration of local ID services. For instance, some do not have a lower age limit, but may only work with children up to the age of 18 years with a moderate-to-profound learning disability. Other community teams may work with any child with an ID (i.e. mild to profound) up to the age of 18 or 19 years. Some adult services may accept referrals from people 17 years and older with a learning disability or autism. Ensuring there is a continuity of service between child and adult services, is vital, not only for patients with moderate-to-profound ID, but also for patients with mild ID who may require support in activities of daily living as well as financial or legal decision-making.
Like anyone else, it is crucial that patients with an ID have their wishes respected when it comes to their care, including end-of-life care. Groups such as the Marie Curie Foundation offer accessible guidance for professionals on a range of topics including communication of issues regarding end-of-life, supportive decision-making, and identifying distress. For further information see www.mariecurie.org.uk/professionals/palliative-care-knowledge-zone/equality-diversity/learning-disability.
Working with carers and people with an ID who attend independently
It is important to consider that some patients with an ID will attend appointments with carers, whereas others will attend independently. As described in the RCGP toolkit (RGCP, n.d.), carers can be valuable sources of information and can help practitioners restructure questions in a way that will be best understood by the patient. In addition, they can also help to confirm whether the information has been understood by the patient and suggest alternative modes of communication which the patient might prefer. Nevertheless, it is crucial that the patient is given the space and modes of communication to express their needs. Also the carer should not answer for the patient when the patient is capable of expressing themselves. For patients with an ID who attend appointments without a carer, it is important that frontline professionals are mindful of when they had their last annual health check and allocate increased time to ensure that they are being understood and the patients have access to information in an accessible form. In this circumstance, it is particularly important that practitioners are proactive in offering and making reasonable adjustments.
Relatedly, issues around parenting and birth control might come to the fore when working with patients with an ID. This raises a number of complicated moral and interdisciplinary issues regarding consent, patient autonomy, confidentiality, and attending to needs for support for both the parents as well as their children who may or may not also have an ID. Such issues have been discussed elsewhere (Schuengel et al., 2017).
Despite being able to parent successfully, some mothers with an ID report discrimination and not having their communication needs met during maternity consultations (Malouf et al., 2017). In addition to the material presented above, the Working Together with Parents Network also offers helpful resources that might be helpful when considering some of these issues - www.bristol.ac.uk/sps/wtpn/forparents.
Independent groups
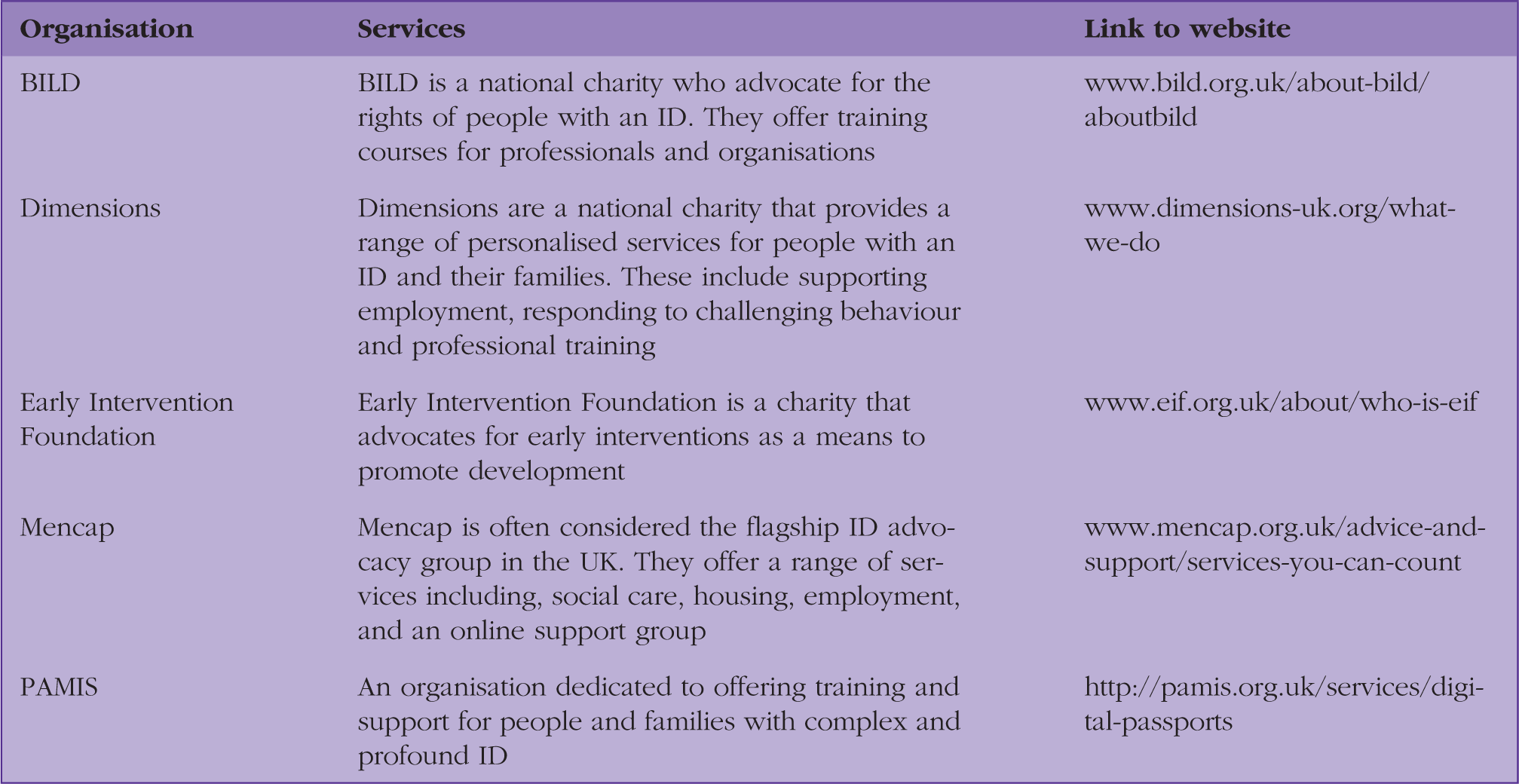
Independent charities and advocacy groups have done remarkable work pushing forward the disability rights agenda while offering specialist and important services to people with an ID. Such services include health and social care, housing, legal advice, employment, online chat forums, support groups, social activities and sports. Some of these groups are described in Table 1. This list is not exhaustive. Moreover, it is crucial to remember that, like anyone else, patients with an ID can benefit from involvement in the suite of community activities, groups, and sports teams with people across the cognitive and behavioural spectrum.
Conclusion
Responding to the health inequalities faced by patients with an ID is a complex task that requires a co-ordinated and multi-pronged approach involving policy-makers, healthcare professionals and clinically focused researchers. It is most important that patients and families are at the centre of decision-making about the services that are indeed ‘beneficial’. GPs have a key role in reducing some of these health inequalities and can offer important services such as the annual health checks. Furthermore, it is crucial that healthcare professionals across the care pathway are mindful and aware of potential abuses and overmedication of patients in this vulnerable population. At an individual level, staff training may prove a useful supplement to wider policy changes and clinical initiatives.
KEY POINTS
It is important that patients with an ID have this recorded in their health record People with an ID often face a host of health inequalities and co-morbidity is common The annual health check is an important and effective services that GPs can offer their patients with an ID Challenging behaviour is a complex multidimensional phenomenon that often serves a communicative or sensory function People with an ID will benefit from person-centred support offered through community-based teams whenever possible Diagnostic overshadowing can be fatal
Footnotes
Funding
The authors wish to thank NIHR School for Primary Care Research [RG94577] and Wellcome Trust [Grant WT103343MA] for their support for work on this paper. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.