
Abstract
The temporomandibular joint (TMJ) is prone to a number of disease states involving any one of its anatomical components. The current favoured term for problems associated with the TMJ is ‘temporomandibular disorder’ (TMD). TMD is one of the most common orofacial pain conditions. Patients will present to GPs and general dental practitioners as well as directly to accident and emergency, typically for referral to Oral and maxillofacial surgery, due to either significant acute pain or chronic pain that can no longer be tolerated. Common features of TMD include pain in the face and preauricular area, restricted jaw movement, and noise from the TMJs during jaw movements. TMD can coincide with poor general health, psychological co-morbidities such as depression and often affects quality of life.
Clinical case scenario
Susan, a 34-year-old woman, attends your practice. She is usually fit and well, but on reviewing her records, her past medical history includes anxiety and depression for which she takes duloxetine 20 mg daily, and irritable bowel syndrome (IBS).
She has booked this appointment as she is experiencing increasing pain from especially the left side of her ear/jaw joint. She is also getting headaches and neck pain. This is troubling her, as it does not seem to be getting any better and eating is becoming more uncomfortable. In addition, she cannot open her mouth fully due to discomfort.
She has experienced similar symptoms before, but the pain seems to be more severe and longer lasting this time round. She thinks it may relate to an ear infection, but wanted to check if there could be any other cause.
Temporomandibular joint anatomy
The temporomandibular joint (TMJ) is a synovial joint between the temporal and mandibular bone, hence its name. The main structural components of the TMJ are the joint capsule, articular disc, mandibular condyles, temporomandibular articular surface of the temporal bone, temporomandibular ligament, stylomandibular ligament, sphenomandibular ligament, and the lateral pterygoid muscle (Fig. 1).
TMJ anatomy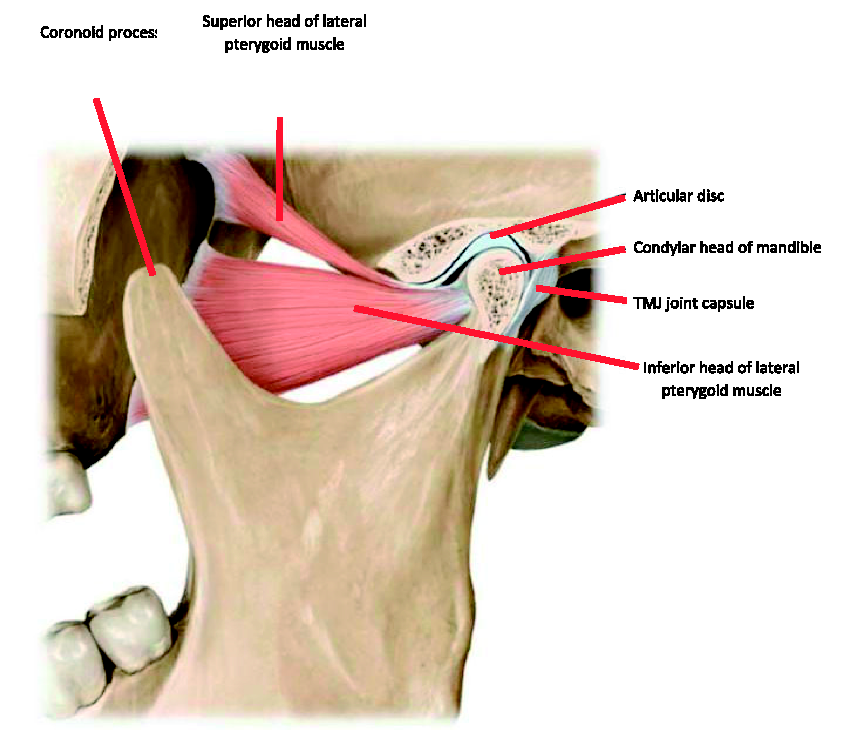
The TMJ is ginglymoarthrodial, capable of both a rotational movement (involving the lower joint space, beneath the articular disc) and a sliding movement (involving the upper joint space, above the articular disc).
The mandible is moved by the muscles of mastication bilaterally: the masseter, temporalis, medial pterygoid and lateral pterygoid. The lateral paterygoid is different in the way that it inserts onto the condylar head of the mandible (the other three inserting onto the coronoid process).
Temporomandibular disorders
‘Temporomandibular disorder’ (TMD) is an umbrella term encompassing a group of related musculoskeletal conditions affecting the TMJ, masticatory muscles and any of the associated structures. TMD has been a hot topic within Oral and maxillofacial surgery (OMFS) and oral medicine. As a result there have been a number of developments affecting the classification of TMDs.
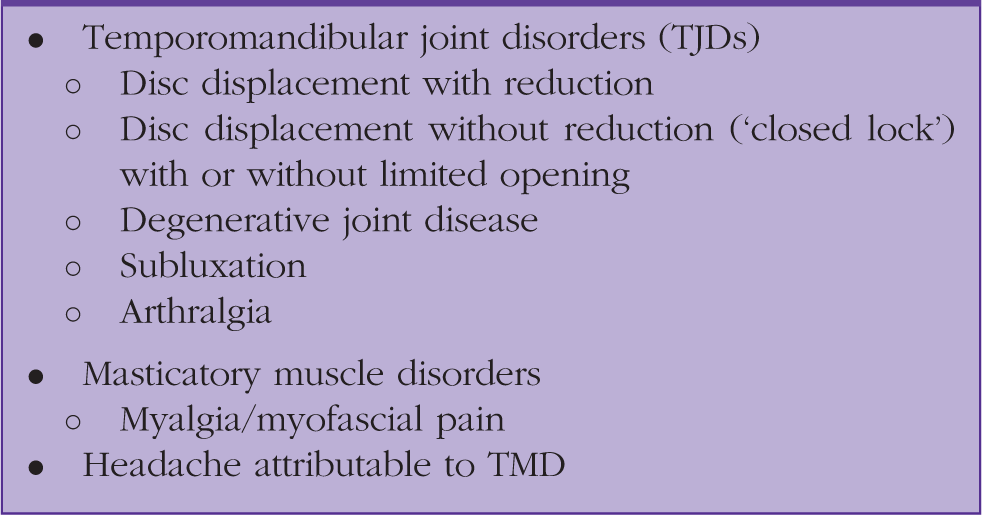
Classification of TMD (DC/TMD).

Principal groups of TMDs.
Notably, the formerly favoured terms ‘TMJD’ and ‘TMJPDS’ (temporomandibular joint dysfunction or temporomandibular joint pain dysfunction syndrome) are no longer recommended, however, they are still widely used. Other examples of the multiple terms that have been used to describe the spectrum of TMD include ‘facial arthralgia’, ‘masticatory myalgia’ and ‘persistent orofacial muscle pain’. These are now of historical note. TMD used to be thought of as a single syndrome, whereas the modern view is that it represents a group of individual but related conditions, and this shift has brought about the change in nomenclature.
Aetiology
Epidemiological data for TMD may vary but certain features remain consistent. There are a number of mutually exclusive aetiological factors, but part of the difficulty in managing TMD is its multifactorial nature. These include anatomical factors, such as internal derangement of the TMJ due to disc displacement. Trauma following a dental procedure or a general anaesthetic (GA) procedure where the mouth has been propped open, a fall onto the chin (transmitting force to the TMJ) or parafunctional habits such as bruxism (grinding or clenching of the teeth) may contribute. These examples may overload the TMJ, leading to cartilage breakdown and/or alterations in the synovial fluid. In addition, psychosocial factors such as stress, anxiety, and depression are significant predictors for the development of TMDs. These factors also predispose patients to developing parafunctional habits, compounding the risk of TMD. Co-morbidities such as chronic fatigue syndrome, fibromyalgia, migraine, irritable bowel syndrome and widespread chronic pain have been implicated. People with these conditions may exhibit generalised pain sensitivity (so-called ‘central sensitisation'). There may also be genetic factors in relation to mood regulation and neurotransmission
Prognosis
There are relatively few large studies available referring to the long-term outcome of TMD. Symptoms resolve spontaneously in up to 40% of people, and in long-term follow-up studies 50–90% of people's symptoms improve with conservative treatment alone (Gauer and Semidey, 2015).
A large US prospective cohort study of 2737 adults (Slade et al, 2013) found that TMD pain occurred as a:
Single episode in 12% of cases Recurrent episode in 65% of cases Persistent episode in 19% of cases
Factors associated with the development of chronic TMD pain and worse prognosis include:
Female age Increasing age at initial presentation Higher subjective pain severity More widespread non-specific symptoms accompanying TMD Co-morbid psychosocial factors (e.g.- anxiety or depression)
Complications
The main complications of TMD include:
Chronic pain Psychosocial distress including anxiety and depression Tooth wear and or fracture, predisposing to dental infection and dental pain Speech problems Swallowing and/or chewing difficulties, which may lead to malnutrition and weight loss
TMD and facial pain
Referred pain describes the phenomenon of pain perceived in an area other than the true source of noxious stimulus. This is especially frequent in the orofacial region, due to overlapping/shared innervation and proximity of structures. Pain referred to the ear and TMJ region is common, and so clinicians must be aware of a range of differential diagnoses that could be responsible for the presenting complaint of pain in this location.
Conditions that may cause facial pain.
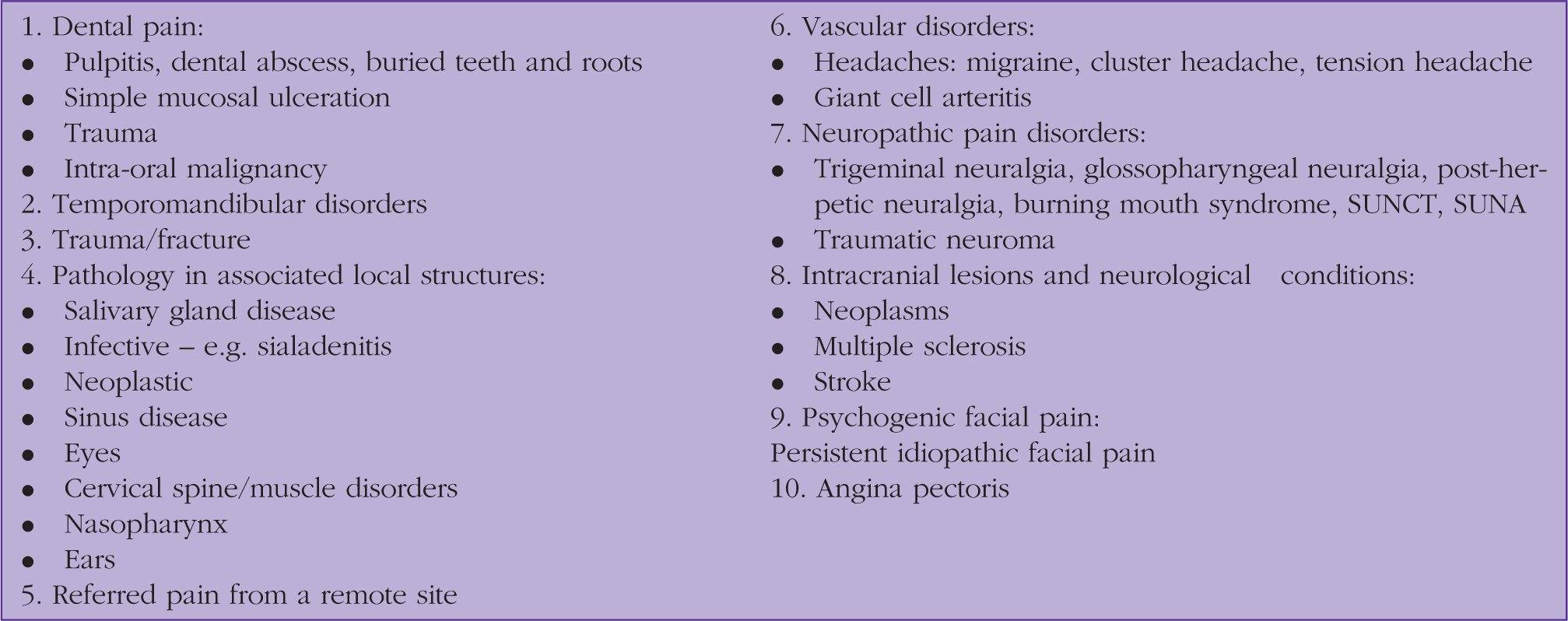
Other important conditions that are beyond the scope of this article include trigeminal neuralgia, the most common example of neuropathic facial pain presenting in primary care, and persistent idiopathic facial pain, frequently associated with psychogenic features such as anxiety and depression.
Features of TMD
There are typical features associated with TMD. First, pain in and around the TMJ and/or the muscles used in mastication is common. Pain usually affects the pre-auricular region, and may radiate to the ear, temple, upper or lower back teeth, cheek, or angle of the lower jaw. Pain may be provoked by palpation of the masseter and/or temporalis muscles or the TMJ, and may be provoked or modified by jaw movement, such as opening or closing the mouth, chewing or grinding
There is commonly a reproducible joint noise of the TMJ (clicking, popping, or crepitus), with or without restricted movement or locking of the TMJ. Painless clicking may indicate disc displacement with reduction. Reduced mouth opening may indicate disc displacement with reduction and persistent closed lock may indicate disc displacement without reduction. There may also be a history of repeated dislocation of the TMJ. It is worth noting that TMJ noises may be sporadic, and may occur in up to 50% of asymptomatic people who do not have a TMD.
Pain may be limited to the temporal region due to the involvement of the temporalis muscles, which inserts into the TMJ. Often this occurs in addition to, rather than instead of, pain around the TMJ. Pain may also be in the form of otalgia and/or tinnitus in the absence of ear disease.
Assessment of facial pain in the context of TMD
History
Pain history.
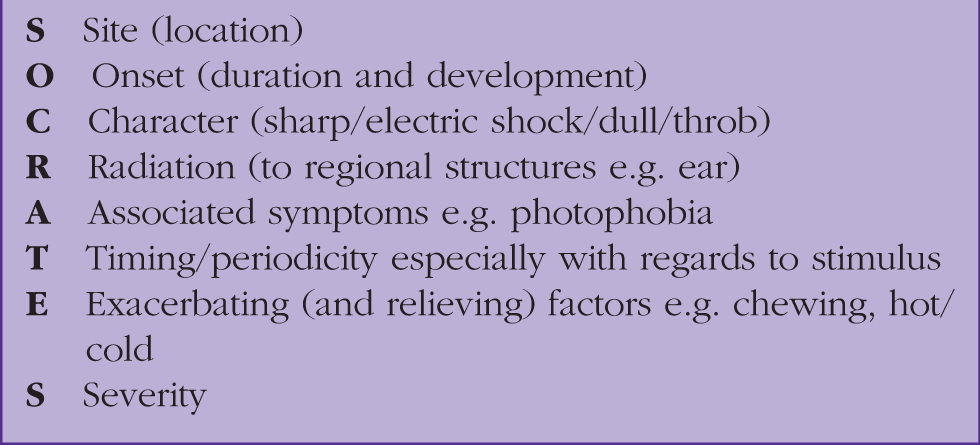
Previous or current dental treatment, as well as any history of previous trauma to the face, should be explored, along with any history of ENT problems. This will include procedures/ diagnoses concerning the ears, nose and paranasal sinuses, all of which could potentially cause referred pain to the TMJ region as previously discussed.
Examination
Systematic examination of orofacial structures and neck is essential and needs to include both TMJs along with associated musculature (muscles of mastication), and salivary glands.
TMJ examination can be broken down (as any joint exam) into look, feel, move:
Look for obvious facial (extra-oral) swelling, which may indicate pathology associated with the submandibular or parotid glands. Obvious swelling around TMJ may indicate a TMJ effusion or mass. Scars could be present due to previous trauma or surgery Feel for tenderness of TMJ, restriction of movement, joint noises (clicking/crepitus), and tenderness of muscles of mastication - temporalis, masseter (and pterygoids, palpable intra-orally) Move in terms of interincisal opening (i.e. assess for trismus), tenderness against resistance and deviation of mandible on opening Intra-oral examination is useful (although this will be more in the remit of GDPs and colleagues in Oral Medicine/ OMFS). This may reveal wear faceting of tooth cusps or macerated mucosa, especially in buccal regions, both indicative of a grinding or clenching habit. It will also provide information as to the extent of restoration of the dentition, state of general oral health and any obvious occlusal discrepancy.
It is worth asking the patient if they are aware of grinding/clenching, however, it may well be the case that patients are unaware as such habits are typically nocturnal and unconscious. For this reason, it can also prove useful to enquire as to whether their partner has noticed any typically associated sounds (depending on the civil status of the patient).
Odontogenic pain has been noted already as the most common cause of orofacial pain. A dental source of pain is confirmed by clinical and radiographic assessment. Common diagnoses including pulpitis, dental abscess, pericorinitis and retained teeth/roots (typically fractured). The dental pulp is notoriously poorly represented by the somatosensory cortex and so patients may well have difficulty in locating the precise location of toothache even if only one causative tooth is identified. Other scenarios may complicate the localisation of dental pain such as referred pain to the ipsilateral maxilla/mandible and a heavily restored dentition (whereby any number of teeth may be implicated).
Identifying and treating dental pain is of course the concern for dental specialties. However, heavily restored teeth or obvious inflammation of surrounding soft tissues, including presence of an abscess/draining sinus, could be fairly readily identified by GPs when patients present with these issues. Figure 2 includes fairly classic examples of how dentitions may look when odontogenic causes are reasonable to consider in a differential.
Top left – multiple fractured teeth with decay still evident. Bottom left – inflamed, swollen gums indicating gingivitis or periodontal (gum) disease. Right – heavily restored dentition with amalgam fillings.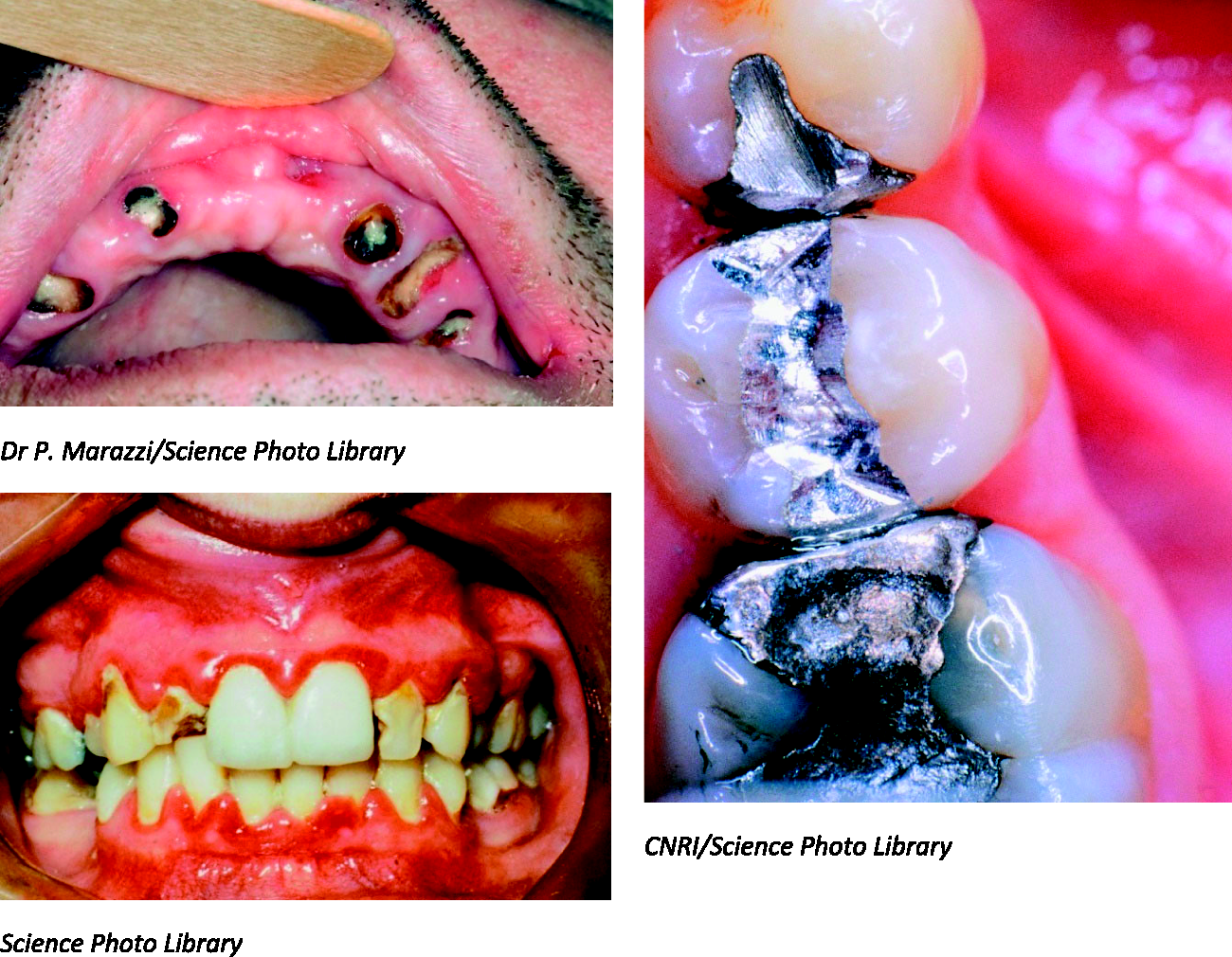
Management of TMD
Figure 3 shows a basic algorithm for the management of TMD in a GP setting. Management of TMD begins with a good history and examination. Symptoms and signs of TMD are usually readily identifiable; however, other important diagnoses may mimic presentation or occur concurrently. There are certain red flag symptoms and signs which must be considered and if any are identified this should prompt urgent referral (Box 5).
A suggested algorithm for GPs in the management of TMD. Major red flags in relation to TMD.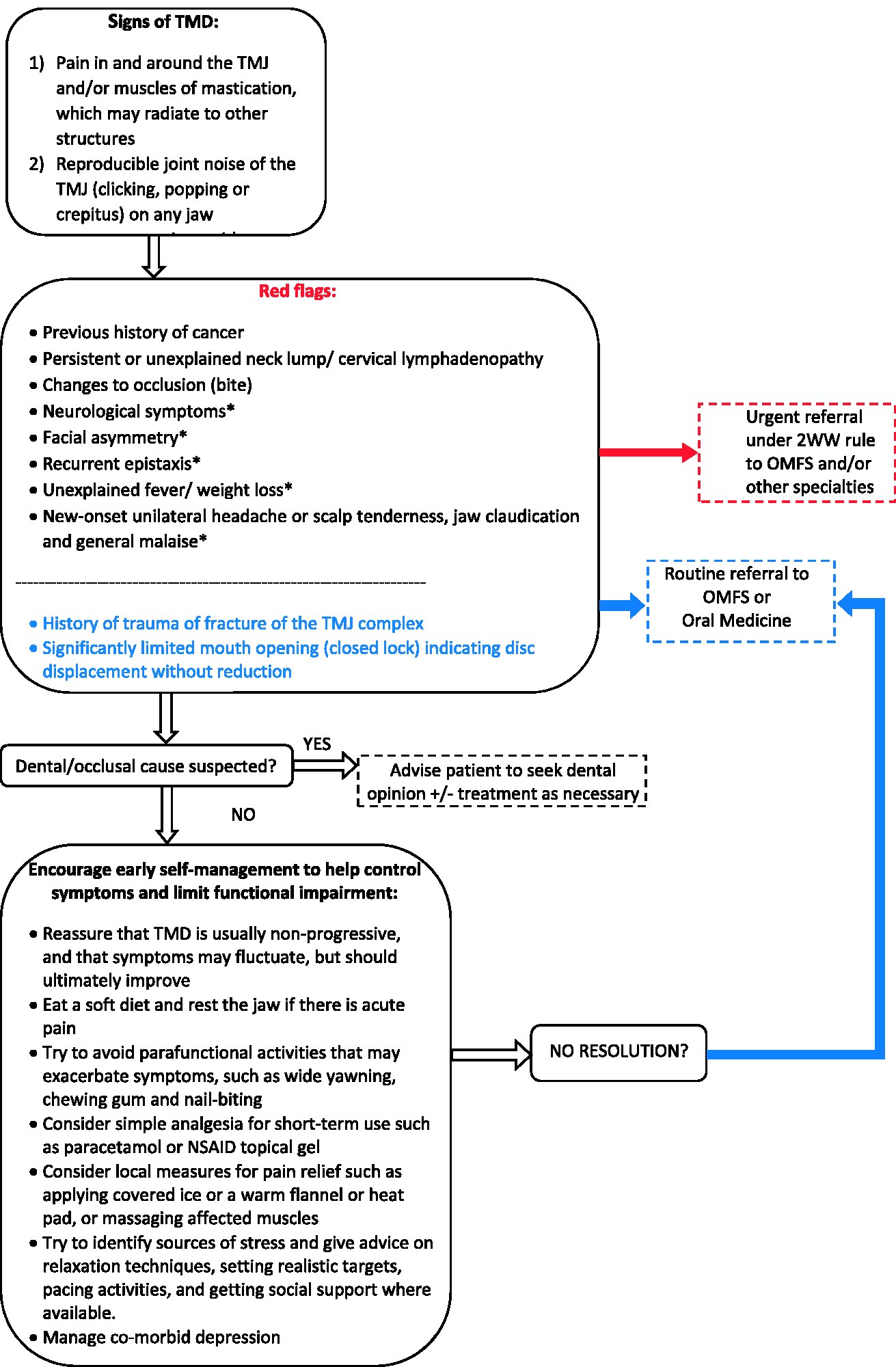
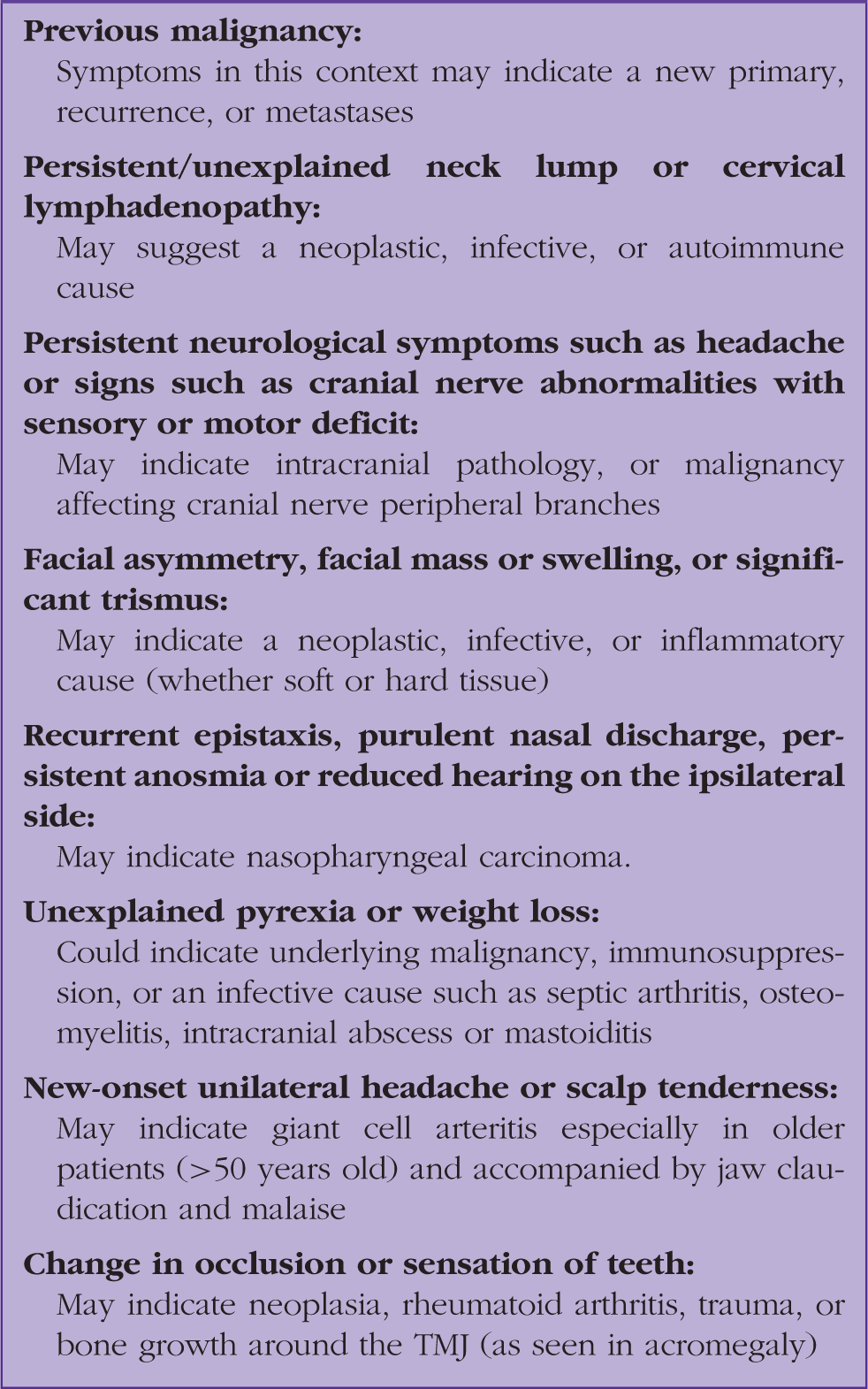
It must be noted that these red flag symptoms in isolation should prompt their own line of enquiry and management. For example unilateral headache should carry a high suspicion of giant cell arteritis, recurrent epistaxis should be referred to ENT and facial asymmetry or neurological symptoms may indicate acute stroke and neurology referral. However, in the context of accompanying TMJ pain, this should prompt urgent OMFS referral.
When red flags have been considered and confidently excluded, the mainstay of treatment for the majority of people is conservative. The importance of reassurance in this approach cannot be over emphasised because anxiety can be the result, as well as a cause, of TMD. Acknowledging and reducing this provides a significant therapeutic effect in most cases. This will further educate and empower patients when it comes to recognising that potential flare-ups of an underlying predisposition to TMD do not represent a sinister development. Explaining that the condition is usually non-progressive and that symptoms may fluctuate, but ultimately improve, is paramount. Extensive evidence shows that the natural history of TMD is of self-limitation.
Management of TMDs by GPs.
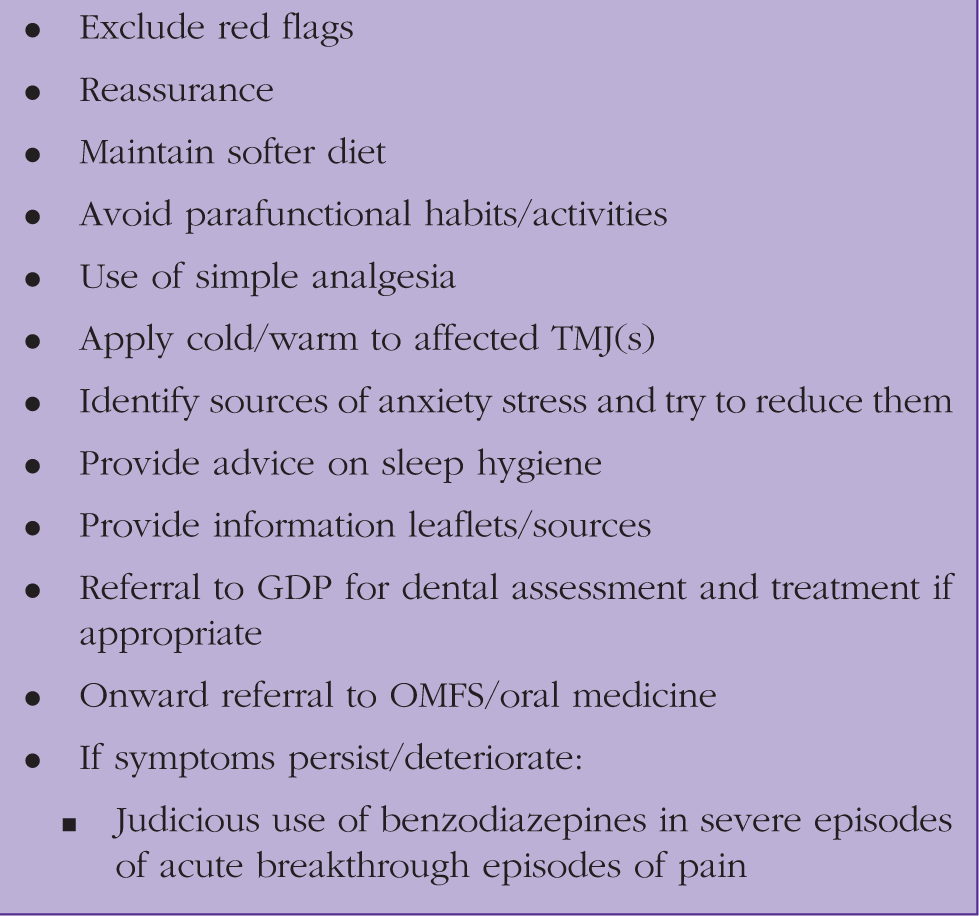
Conservative
In the interest of empowerment, there are a number of self-management strategies that patients are encouraged to adopt early in the case of suspected TMD. These include maintaining a softer diet and resting the jaw if there is an acute episode of pain. Patients should void parafunctional activities known to exacerbate symptoms e.g. wide yawning, tooth grinding or jaw clenching, chewing gum or pencils, and nail biting. Simple analgesia is appropriate for short-term use, such as paracetamol or a nonsteroidal anti-inflammatory drug), the latter in either topical or systemic form. Local measures can be effective for pain relief, such as applying covered ice or a warm flannel or heat pad, or massaging affected muscles. Patients should be encouraged to identify sources of stress and be given advice on relaxation techniques, setting realistic targets, pacing activities, and seeking social support where available. Manage any co-morbid depression/anxiety accordingly, often with overlapping strategies. Provide advice on sleep hygiene, as this will encourage general relaxation and potentially reduce an anxiety component to symptoms related to TMD
Sources of further information for patient reference
Medical/non-surgical
When patients present with acute and severe paroxysmal outbreaks of pain associated with TMD, consider prescribing a short course of a low-dose benzodiazepine. Diazepam is usually favoured unless contraindications apply - 2 mg up to three times daily, for a maximum of 2 weeks.
If there is chronic pain, consider prescribing a neuropathic analgesic such as amitriptyline or gabapentin. Both of these are off-label, but widely used in secondary healthcare settings.
Referral to additional specialists if appropriate
Colleagues in other specialties should be included in the holistic management of TMDs. These include a dental referral if there is poor oral health, suspected malocclusion or dental pathology, or for consideration of an occlusal splint (typically worn at night and more useful for people who have a parafunctional habit). This can be provided by local dental hospitals/OMFS/oral medicine departments, especially if patients cannot afford this on a private basis. Referral to psychology services for cognitive behavioural therapy is appropriate if there is significant associated psychological distress and/or to help with pain-related anxiety. Physiotherapy can provide advice on passive jaw stretching exercises, posture training, and massage. Acupuncture may help relax muscle spasm, if available. Finally, a referral to pain clinic may be necessary in longstanding or unresponsive cases.
Surgical
Surgical intervention is not appropriate for the vast majority of patients. Invasive procedures are considered only once significant disruption of the joint apparatus is confirmed by further investigation as well as failure to respond to non-surgical therapies. Essentially, referral is reasonable and expected in the case of TMDs where symptoms are severe and have not responded to reasonable attempts at conservative therapy, along with cases demonstrating suspicious features.
Refer to OMFS/oral medicine, ENT, neurology or a multidisciplinary pain clinic for further specialist input in any of these cases:
Chronic TMD symptoms lasting longer than 3 months Persistent or deteriorating symptoms despite primary care treatment Uncertain diagnosis Significant psychological distress associated with symptoms and/or preoccupation with their occlusion (e.g. hyper- awareness of their bite) Unexplained persistent pain or chronic orofacial/widespread pain
Secondary care investigations and management
Specialist management is only considered for people with significant functional impairment of the TMJ and/or an intra-articular disorder such as disc displacement, degenerative joint disease or in refractory cases unresponsive to conservative therapy. Plain X-rays are conducted as a basic assessment of any underlying dental pathology, fractures, dislocations or severe degenerative joint disease. Computerised tomography (CT) imaging will assess for degenerative joint disease or subluxation of the TMJ. CT is also useful for assessment of complicated fractures and bony components of the articular apparatus. Magnetic resonance imaging is favoured for TMJ assessment e.g. in the case of disc displacement, subluxation, arthrosis, or synovial proliferation.
Botulinum toxin (Botox) injection into the masseter and temporalis muscles of mastication is now more commonplace in secondary care settings, and can be very effective. However, the mechanism of action and mode of administration lends itself more to use in muscle-related TMDs - parafunctional habits, myalgia and hypertrophy (more often relating to the masseter muscle). This should only be considered as adjunctive to first line therapies.
Surgical options are considered a last resort. Either arthrocentesis or arthroscopy can be considered for non-myogenous TMDs. Arthroplasty can be performed for more severe TMJ degeneration. Eminectomy or eminoplasty for recurrent TMJ dislocation is considered. Total prosthetic TMJ replacement is reserved for end-stage degenerative disease.
It is notable that some historically favoured treatments are no longer recommended, due to either lack of evidence of benefit or worse, evidence of causing harm. Prominent examples include occlusal adjustment (selective reduction of the tooth enamel to achieve a more harmonious, evenly distributed bite) and orthodontics.
Summary
TMD is common, and a frequent clinically encountered source of facial pain. It typically affects younger individuals and is more frequent in females. It is commonly though not exclusively associated with psychosocial factors. The natural history of TMD is self-limiting, and for this reason reversible strategies are greatly favoured over irreversible/invasive alternatives. Conservative therapies are usually very effective, but referral onto specialist departments may be necessary if these therapies fail to adequately relieve symptoms. It is important, however, to consider alternative diagnoses if the presentation of TMD is atypical or accompanied by red flags.
KEY POINTS
TMDs are common, encompassing a wide range of conditions associated with the TMJ and associated structures Psychosocial factors typically play a role in the causing or exacerbating symptoms TMD is usually ultimately self-limiting TMD usually responds to conservative treatment strategies Onward referral may be necessary for people whose symptoms are severe or who do not respond to first line therapies More significant pathology should be considered in the differential diagnosis
Footnotes
Acknowledgment
We would like to thank Dr Elizabeth Head for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.