Abstract
The incidence of oropharyngeal cancer in the UK has almost trebled in the last few decades and continues to climb. It is expected that its associated symptoms will become increasingly common presenting complaints in primary care, where early recognition is hugely advantageous for patient outcomes. Thorough history and examination, plus a sound knowledge of associated risk factors, is vital in identifying potential cases, and an understanding of the correct referral pathways ensures patients are appropriately referred to head and neck cancer services. A broad overview of benign differential diagnoses, subsequent investigation and management of oropharyngeal cancers is helpful in order to properly inform and support patients in their next steps.
Clinical case scenario
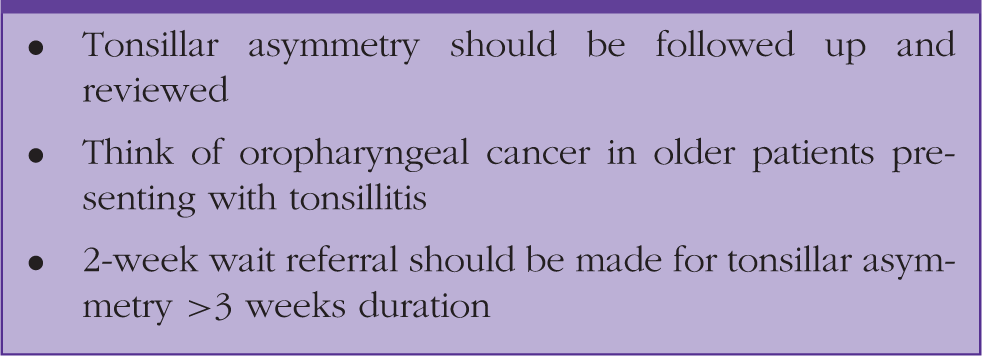
Alan, a 47-year-old man comes to see his GP with a 3-day history of sore throat, with tonsillar exudates and asymmetrical swelling of the left tonsil in comparison with the right. He is a current smoker with a 20-pack-year history. In this case tonsillitis seems to be the most obvious cause of his symptoms and he is treated with a 10-day course of Penicillin V. At this point in time he does not qualify for a 2-week wait referral; however, there is some tonsillar asymmetry which needs to be reviewed once the infection settles.
Alan is reviewed 3 weeks after finishing his course of antibiotics. His infective symptoms have fully subsided, but he has an ongoing left-sided tonsillar swelling as seen in Figure 1 (grade 3 on the left, grade 1 on the right) and some left-sided intermittent otalgia.
Patient photo of left tonsillar mass.
Otoscopy and neck examinations are normal. Alan now qualifies for a 2-week wait referral to rule out a tonsillar malignancy. The tonsillitis may have simply drawn attention to a tonsillar mass that was there beforehand and despite him being relatively young we know that oropharyngeal cancers are becoming more prevalent in the under-50 s. Tonsillitis is uncommon in older age groups and with risk factors such as smoking it is appropriate to suspect a cancer diagnosis and refer accordingly.
Oropharyngeal cancer
The oropharynx is anatomically comprised of the posterior third of the tongue, the soft palate and uvula, tonsils, the pharyngeal arches (which enclose the tonsils) the posterior and lateral oropharyngeal wall and lingual aspect of the epiglottis. The vast majority of malignant tumours are squamous cell carcinomas, the most common site being the tonsil, followed by the base of tongue (Tobias and Hochhauser, 2014).
Incidence of new oropharyngeal cancer diagnosis has nearly trebled within the last 20 years. From 2000 to 2016 there was a 189% increase in new cases in the UK (from 1029 to 2977 cases). The disease occurs approximately three times more commonly in males than females, with male incidence also growing at a slightly faster rate (Office for National Statistics, 2018). With the emergence of Human Papilloma Virus (HPV)-related disease, the age demographic is getting younger with increasing numbers of patients being diagnosed who are under 50 years in age (Elrefaey et al., 2014). Five-year survival rates are about 54% in men, and 61% in women, as shown by age-standardised net survival (Muller et al., 2016). Unfortunately, there have been no significant advances in survival rates, and this may be partly due to a significant proportion of patients presenting late; oropharyngeal malignancies typically remain fairly asymptomatic until they become large enough to spread locally or metastasise to local lymph nodes.
History
Typical symptoms.
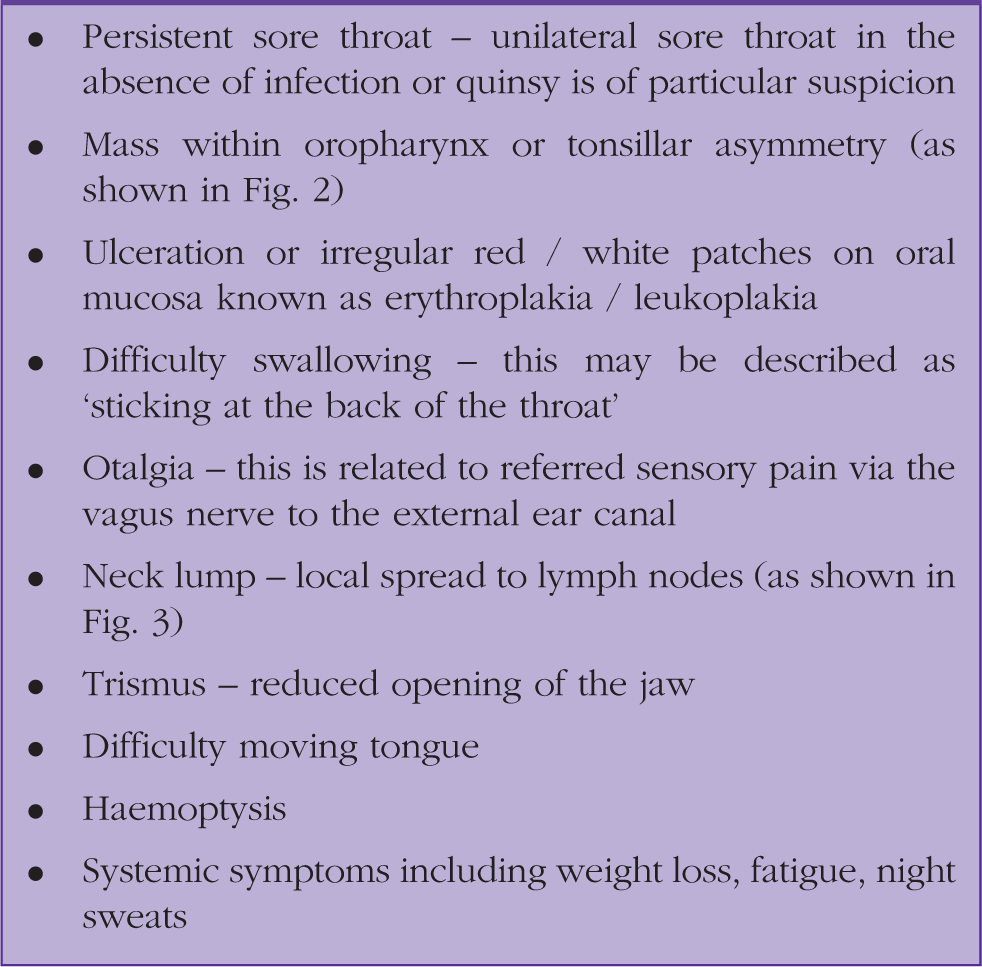
Cases of malignancy can be missed and referral to specialist services (head and neck clinic) is delayed if signs and symptoms are mimicked by infective conditions such as tonsillitis and peri-tonsillar abscesses. It is important to remember that tonsillitis is much less common in older adults, and so a high degree of suspicion should be had, especially if patients present with recurrent or unilateral symptoms and have additional risk factors (Bannister and Ah-See, 2014).
Main risk factors
Tobacco smoking
Around one-in-five people in the UK smoke, and the link to oropharyngeal cancer, in addition to most other cancers, comes as no surprise. Smokers are three times more likely than never-smokers to develop pharyngeal cancer with higher risk profiles seen in the heaviest smokers, both male and female (Gandini et al., 2008; Lubin et al., 2011). Limited research is available as yet on any causal effect of e-cigarettes or ‘vaping’ on head and neck cancer, however, it has been shown that some chemical components are cytotoxic to oropharyngeal tissue and can induce DNA damage. Their link with head and neck cancers cannot be ruled out; therefore, we should be cautious on recommending it as a safe alternative to smoking. It will be interesting to see what research may reveal regarding long term use in the future (Welz et al., 2016).
Smokeless tobacco such as Betel Quid (popular in the Indian subcontinent) and Snuff/Snus (popular in Scandinavia and North America) involve placing dried tobacco inside the oral cavity in direct contact with the mucosa. It is most closely linked to oral cavity cancers, due to direct contact with tissues affected, but is also associated with oropharyngeal malignancies.
Alcohol
Excessive alcohol consumption is associated with around a third of oral and pharyngeal cancer cases. Pure ethanol has never been shown to be carcinogenic, but it is thought that it acts in conjunction with other more carcinogenic substances in the drink. There is also evidence to suggest there is a synergistic effect in those who drink and also smoke (Johnson, 2001; Parkin, 2011). The risk for males is three times as high as that for females, and it is hypothesised that this is related to a higher use of tobacco and consumption of alcohol (Office for National Statistics, 2018).
Human papillomavirus
Over the last 20 years it has become apparent that HPV has a pathogenic role in head and neck cancers in general, most specifically oropharyngeal cancers. HPV subtypes 16 and 18, which are aetiologically related to cervical and anogenital cancers, have been found to be responsible for a subset of oropharyngeal cancers which are referred to as HPV-positive malignancies (Elrefaey et al., 2014). They are mostly transmitted to the mouth via oral sex, and hence, the recent increase in cases may echo changes in sexual behaviour in society (D’Souza et al., 2007). HPV-positive cancers tend to occur in a younger demographic of patient, often with relatively less smoking and alcohol exposure. There is also a higher frequency among Caucasian and male patients groups. The predilection of HPV for the oropharynx is unknown, but it is thought that tonsillar mucosa in particular is a good reservoir for the virus; this mirrors the high proportion of HPV-positive tonsillar tumours specifically. Fortunately, HPV-positive cancers have a more favourable outcome and seem to be more responsive to chemo- radiotherapy, despite any favourable related factors such as age (Elrefaey et al., 2014; Yete et al., 2018). With the introduction of the quadrivalent HPV vaccination, which has now been extended to cover boys in addition to girls (Markowitz et al., 2014), a direct effect on falling numbers of oropharyngeal cancers is anticipated.
Examination
It is vitally important to thoroughly examine the oral cavity and oropharynx in order to fully assess the extent of any abnormalities; there may be lesions that the patient has not noticed or lymphadenopathy that may indicate more advanced disease.
Key elements:
Thorough oral examination with two tongue depressors (as demonstrated in Fig. 4) Take care to fully examine the tonsils looking for asymmetry and the base of tongue (these are most common sites for oropharyngeal malignancy). Palpation of the tonsils, if tolerated by the patient is useful to differentiate between benign and malignant pathology. Neck examination (in all patients) Otoscopy (to rule out other causes of otalgia) Also look at the tongue, palate, floor of the mouth, buccal area and gingivolabial sulcus (gum area above and below teeth) to look for concurrent oral cavity cancers
Referral pathways
The National Institute of Health and Care Excellence (NICE) guidelines focus mainly on potential oral cavity or laryngeal cancers, and so there is some ambiguity about which patients should be referred under the 2-week wait rule. Below is a comprehensive list of when to refer on to Head and Neck Cancer services (London Cancer, 2015)
Consider a 2-week wait suspected cancer pathway referral for patients with persistent or unexplained:
Mass/lump in the oropharynx Mass/lump in the neck Sore throat (particularly if unilateral) Ulceration in the oral cavity >40 years old with unilateral otalgia/dysphagia/odynophagia Erythroplakia/leukoplakia (red/white patches), urgent dental referral within 2 weeks
The key points here are persistent or unexplained. Persistent is generally considered as over 3 weeks of ongoing or progressive symptoms. Most benign disease will be self-limiting or resolve with treatment. Unexplained symptoms may be due to there being no plausible benign cause or a patient who has persistent symptoms where benign disease is becoming is less likely. A watch-and-wait approach does come with the caveat of common sense; if a patient presents late with a highly suspicious lesion, this requires prompt referral and it would be inappropriate to see if this resolves.
Take home messages.
Investigation and management
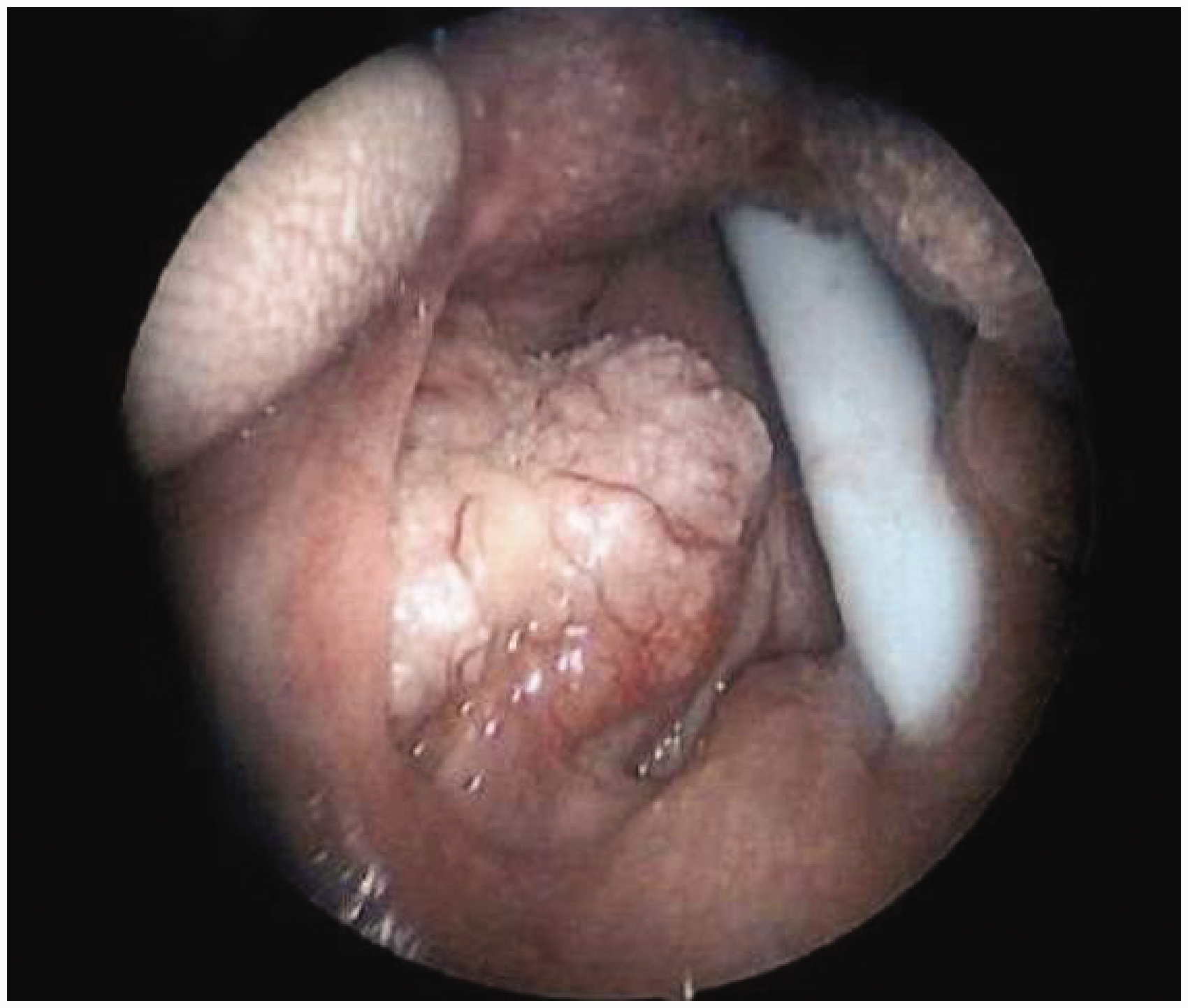
It is imperative that patients are alerted and aware that they are being referred to a cancer service and will be seen within 2 weeks. On the most part they can be reassured that the vast majority of patients seen do not have a cancer (NICE, 2015). During a 2-week wait head and neck clinic, patients should expect to have a thorough history and examination, which will include a flexible nasendoscopy. A biopsy is likely to be arranged in order to gain a histological diagnosis; this may be a fine needle aspiration/biopsy under ultrasound guidance for a neck lump or as a procedure under general anaesthetic, such as a panendoscopy (as shown in Fig. 5), for lesions within the oropharynx. Further imaging, most likely magnetic resonance imaging may be used for diagnosis and to determine extent of disease. Subsequent computed tomography scanning may be required for staging.
Should the diagnosis confirm an oropharyngeal cancer there are multiple treatment options that are available and will be discussed among the multi-disciplinary team. Depending on primary site and staging, usually this is a combination of surgery, radiotherapy and chemotherapy with curative or palliative intent (Cancer Research UK, 2020). Advances in Intensity-modulated radiotherapy allows for local targeting of cancers while minimising doses to surrounding tissue; this therefore reduces long term side effects of radiotherapy such as dry mouth and dysphagia (Setton et al., 2012) In the last 15 years the introduction of transoral robotic surgery (TORS) for suitable patients has also resulted in better outcomes and reduced morbidity versus traditional surgical approaches (Leonhardt et al., 2011; Motz et al., 2017). It has also been suggested that TORS can decrease the intensity of adjuvant treatment, and thus preserve swallowing function. This is currently being investigated in a national Random Controlled Trial with primary results due in 2022 (Nixon, 2014)
It is important to highlight that treatment is tailored specifically for each patient, taking into account staging, performance status and co-morbidities as well as local capabilities. We hope this article has provided readers with an increased awareness of referral pathways and treatment options in order to support patients.
KEY POINTS
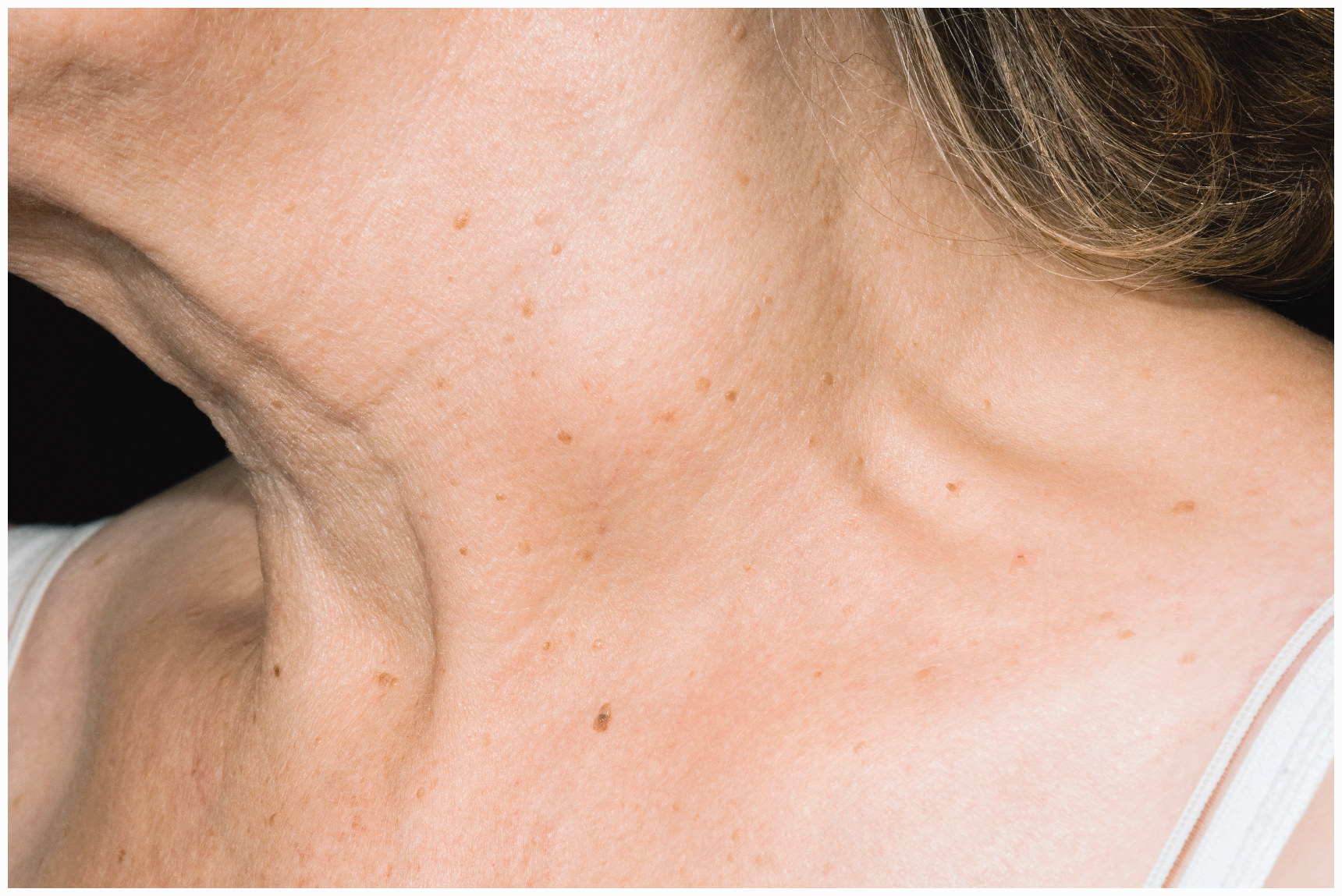
The incidence of oropharyngeal cancer is increasing, in particular HPV-positive malignancies Five-year survival is approximately 50–60% and likely affected by late presentation Risk factors include being male, HPV, smoking, alcohol, and poor diet A thorough history and examination to elucidate symptoms and signs of changes to the oral cavity, oropharynx and neck is vital to determine whether a 2-week wait referral is appropriate Patients will be reviewed by a Head and Neck Specialist who will conduct a range of investigations to confirm diagnosis Treatment of oropharyngeal cancer has advanced in recent years – if eligible, patients will be offered a combination of surgery, radiotherapy or chemotherapy to treat their disease Tonsillar asymmetry. Neck lump. Oropharynx and oral cavity examination with two tongue depressors. Panendoscopy demonstrating tonsillar mass.