
Abstract
Fragile X syndrome is one of the most common genetic causes of learning disability. Patients with this and other neurodevelopmental disorders will often present to primary care before a diagnosis is made, and this can be challenging and worrying for patients and other carers. These patients may face a number of barriers in accessing healthcare services including communication, behavioural and sensory difficulties. It may be difficult to understand whether symptoms are part of their condition or because of a comorbidity that needs to be addressed. Input from families and carers can be vital in helping with diagnosis. This article aims to outline the key clinical features, diagnosis and management of this syndrome.
Clinical case scenario 1.
You are in afternoon surgery and a 19-month-old child called Jimmy attends with his mother. His mother is concerned that he is not yet walking and is only using single words to communicate. She is especially concerned as this is quite different from her two previous children. He is confidently bum shuffling around the consultation and is generally interacting well with you. He does have a large head and ears. His head circumference is over the 75% centile.
You refer him to community paediatrics; they make a diagnosis of Fragile X syndrome after a period of assessment and genetic testing. His mother is distraught and returns to the surgery. She is terrified of how she will manage Jimmy’s ongoing medical needs. She works as a receptionist in a busy hospital clinic and finds it difficult to take time off work to attend his various medical appointments. She is a single mum with two older children and an elderly mother living in the same house.
Background
Fragile X syndrome is the most common cause of learning disability due to a genetic defect. It is an X-linked dominant disorder and can occur in all major ethnic groups and races. It is caused by the repeat expansion of a trinucleotide sequence. The number of repeat sequences found will determine the severity of the clinical syndrome. The UK prevalence of the condition is currently around 2.3 in every 1000 people, but there is also a pre-mutation which is significantly more common (Song et al., 2003). This is thought to exist in around 1 in 130–260 females and 1 in 250–810 males (Chonchaiya et al., 2009).
Pathophysiology
Fragile X syndrome is associated with aberrant mutation of the CGG nucleotide sequence (where the C is cytosine and the G is guanine) on the fragile X mental retardation (FMR1) gene. FMR1 is located on the X chromosome and inheritance is X-linked dominant. Consequently, individuals only need to have one defective X chromosome in order to be affected by the disorder. This CGG sequence would normally repeat between 6 and 54 times, but if there are greater than 200 repeat sequences, this blocks the production of fragile X mental retardation protein. This protein is responsible for the production of other proteins and is also important for synapse development. Anybody with over 200 repeat sequences will have Fragile X syndrome. If there are only between 55 and 200 repeats, these patients may have a pre-mutation. The pre-mutations are unmethylated, but if they expand to a full mutation, methylation will occur (Finucane et al., 2012). Methylation is where a methyl group is added to DNA and is a normal process. In Fragile X, it means that the FMR1 gene is not functioning to produce the fragile X mental retardation protein. The greatest importance of the pre-mutation is for future generations, but other clinical implications of the pre-mutation are discussed below.
Genetics
The genetic implications of Fragile X syndrome (and the pre-mutation) will depend on the gender of the affected parent, as the defective expansion sequence is found on the X chromosome. In X-linked conditions, often the females can only be carriers and only the males can have the condition. In Fragile X, both males and females can be carriers and have the condition, due to the existence of the pre-mutation state which occurs because of differences in the number of CGG repeats.
Probability of offspring being affected by Fragile X syndrome.

Females with a pre-mutation of the FMR1 gene have a high risk of having children with Fragile X syndrome, as the number of CGG repeats can increase through the generations. The greater the number of CGG repeats possessed by a female who has the pre-mutation, the more likely it is that her children develop Fragile X syndrome. These females have unstable CGG repeats, which can increase during oogenesis.
Males with a pre-mutation and Fragile X syndrome will not pass this on to their sons, as they will pass on only a Y chromosome, and thus their sons will not inherit the defective gene (Table 1). Females will always inherit the pre-mutation from their father, as they will receive the father’s X chromosome with the defective gene. Daughters tend not to be affected with Fragile X syndrome, as the pre-mutation is generally quite stable, meaning no increase in CGG repeats when transmitted from father to daughter. However, there is a greater risk for future generations as the pre-mutation can become unstable.
Clinical features
Fragile X syndrome has a broad clinical phenotype with variable manifestations. It is often diagnosed before the age of 3 years with motor and language delays being the most common presenting features. A family history of Fragile X may be evident, but it is not present in around 30% of cases and physical features are also not present in around 30% of cases (Chonchaiya et al., 2009).
The clinical features tend to be more severe in males, although the degree of learning disability can vary from mild to severe. In females, the clinical picture has a greater degree of diversity. Some females are severely affected, but others are largely asymptomatic. This is because females can have random X-inactivation (McKechanie et al., 2019).
Fragile X syndrome has both physical, developmental and behavioural aspects, as well as associated comorbidities of epilepsy, attention deficit hyperactivity (ADHD) and autism. The diagnosis should always be considered in patients presenting with autistic features.
Physical features include a typical facial shape, large heads with long narrow face and a prominent forehead and jaw. They may have facial asymmetry. The head circumference will often be higher than the 50th percentile. They also have long protruding ears with a high arched palate. Young males typically have a hallucal crease (a single crease between the first and second toes), sensitivity to touch, and are unable to touch their tongue to the lips. Sensory difficulties include strabismus, which may reduce visual acuity. Recurrent sinusitis and otitis media may be problematic leading to a degree of conductive hearing loss. This can exacerbate behavioural problems.
Patients may have a number of joint issues including hyper-extensible finger joints, pectus excavatum, scoliosis, flat feet and recurrent joint dislocations especially shoulder and patella. Other important clinical features are mitral valve prolapse and macro-orchidism in males after puberty which can be up to two to three times the normal size.
These patients have increased rates of childhood inguinal hernias and feeding problems including gastro-oesophageal reflux, vomiting and failure to thrive. A small number will experience seizures (14% of males, 6% females), which are often complex partial and typically start around 6–24 months, although they often outgrow these by early childhood (Berry-Kravis et al., 2010).
A small number of patients can also have a Prader–Willi syndrome phenotype with obesity, hyperphagia and hypogonadism; it is also associated with poor linear growth, small hands and feet, and diffuse hyperpigmentation.
Behavioural features
Patients generally have a low IQ (usually under 70) on formal testing with delayed developmental milestones. Low IQ is found in around 85% of males and 25–30% of females (Chonchaiya et al,. 2009). Motor milestones are typically delayed, due to hypotonia and patients may toe walk.
Language delays including echolalia and perseveration (inability to complete a sentence due to repetition of words at the end of a phrase) often occur. The prevalence of these delays increases with age.
They also experience impaired short-term memory, expressive language ability and difficulties with problem solving. Behavioural problems are common. This can include anxiety, self-injurious behaviour and tantrums, dislike of routine change. Hyperactivity similar to ADHD is also common including aggressive behaviour and attention deficits.
A co-existing diagnosis of autism is common and can be found in up to 20–50% of patients. Behaviours include poor eye contact, hand flapping and self-stimulating behaviour (Kaufmann et al., 2017). Other features include delayed toilet training with frequent enuresis, obsessive–compulsive disorder and sleep disturbances. They may have difficulty falling asleep, frequent night waking and loud snoring.
Implications of pre-mutation
The majority of people who have the pre-mutation are intellectually normal. However, it is not an entirely benign condition and there is still a risk they may have some mild physical symptoms such as prominent ears, as well as a degree of learning disability. This may not initially be noticed and there is significant under-diagnosis of patients with the pre-mutation. They can also share some of the behavioural traits including anxiety, depression, autistic-like behaviour and learning disability.
The pre-mutation also has a risk of associated disorders, which include:
Fragile X-associated tremor/ataxia disorder: This is progressive adult onset movement disorder with rhythmic, involuntary movements, which can appear similar to Parkinson’s disease. It more typically affects men Fragile X-associated primary ovarian insufficiency: The risk of this is directly related to the number of CGG repeats. It presents with irregular periods, reduced fertility, premature ovarian failure and elevated follicle stimulating hormone (FSH) levels. There is a risk of around 21% in those patients with the pre-mutation. There is around a 2% chance of women who have premature ovarian insufficiency (POI) of unclear cause being carriers of a pre-mutation in the FMR1 gene (Sherman et al., 2005).
Differential diagnosis
The differential diagnosis for Fragile X syndrome is very broad. It includes:
General learning disability Other chromosomal abnormalities causing learning difficulty, e.g. Down's syndrome Sex chromosome anomalies, e.g. Klinefelter's syndrome Sotos syndrome ADHD Autistic spectrum disorder Marfan's syndrome
Investigations
Diagnosis of Fragile X syndrome can be made on blood sample or chorionic villus biopsy which can be sent for DNA analysis. Most laboratories currently use a combination of Southern blotting, which detects full mutations, and polymerase chain reaction (PCR) testing to identify pre-mutations and smaller CGG repeats. PCR is faster, cheaper and will give a more accurate estimate of CGG triple repeats if a permutation is present. Testing is around 99% sensitive (Finucane et al., 2012).
Karyotyping is also usually performed to look for other chromosomal abnormalities. Other investigations that may be useful include spinal X-rays to look for evidence of scoliosis and echocardiogram to look for mitral valve prolapse. Taking a good family history is also useful, as previous generations may have features of pre-mutation.
Management
There is currently no cure for Fragile X syndrome, but a number of pharmacological, behavioural and cognitive interventions may improve quality of life. Interventions will differ depending on the age of the affected patient. Early years interventions that aim to try and maximise the ability of the affected child include speech therapy, special needs education and behavioural therapy.
It is also important for GPs to be aware of the concept of ‘diagnostic overshadowing’. This is the concept that symptoms are attributed to the underlying condition, i.e. Fragile X syndrome when they actually instead are due to a potentially treatable comorbidity (McKechanie et al., 2019).
Medications
Various different pharmacological treatments have been used, mainly to treat the associated behavioural issues, although there is minimal evidence of the efficacy of any of these options. Stimulants e.g. dextroamphetamine and methylphenidate can be used for hyperactivity behaviours and selective serotonin reuptake inhibitors for symptoms of anxiety, but the latter should be avoided in patients with impulsivity due to the risk of suicide associated with this course of action.
Antipsychotics can be used for mood stabilisation, improving attention and reducing anxiety. Aripiprazole is often the first line agent. Anticonvulsants are used if seizures are present. First line agents often include carbamazepine or sodium valproate.
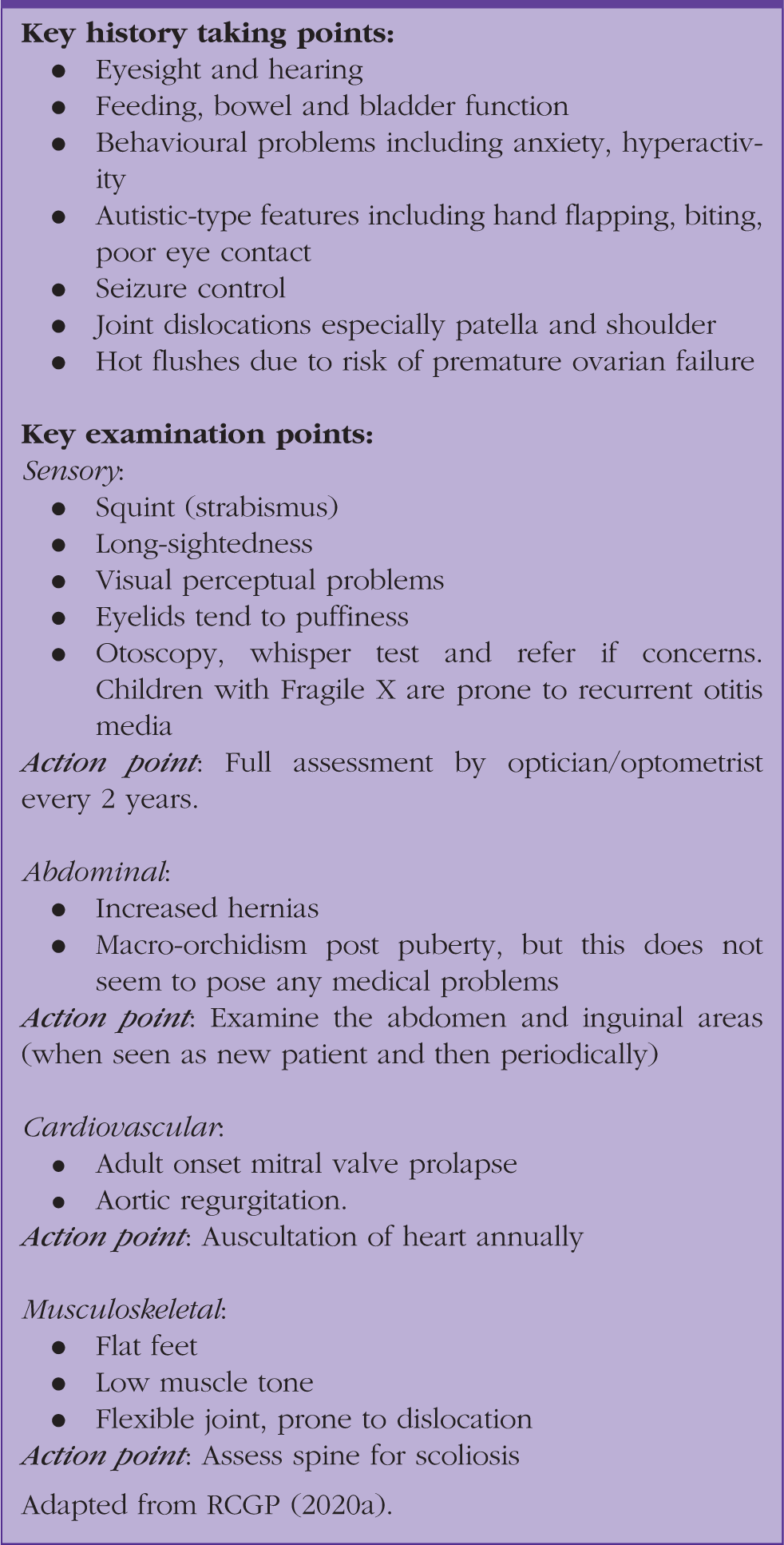
RCGP guidance for Fragile X-specific health check.
It is also important to consider the carer burden for parents and carers of Fragile X patients, especially if they are frequently exhibiting challenging behaviours. There are specific organisations that provide support for families. The UK organisation is the Fragile X society, whose website can be accessed at www.fragilex.org.uk.
Genetic screening and counselling
There is currently no national UK screening programme, and screening is only done for carrier screening in affected families. Foetal testing can be done via amniocentesis or chorionic villus sampling (CVS), but these procedures both carry risk of miscarriage. Prenatal testing should be offered to all women who are known carriers of the pre-mutation or full mutation or those with a family history of Fragile X syndrome. Amniocentesis after 15 weeks is generally preferred, as the methylation status of the FMR1 gene may not yet be established in the chorionic villi at the time of sampling, leading to the need to do a follow up amniocentesis if CVS is performed.
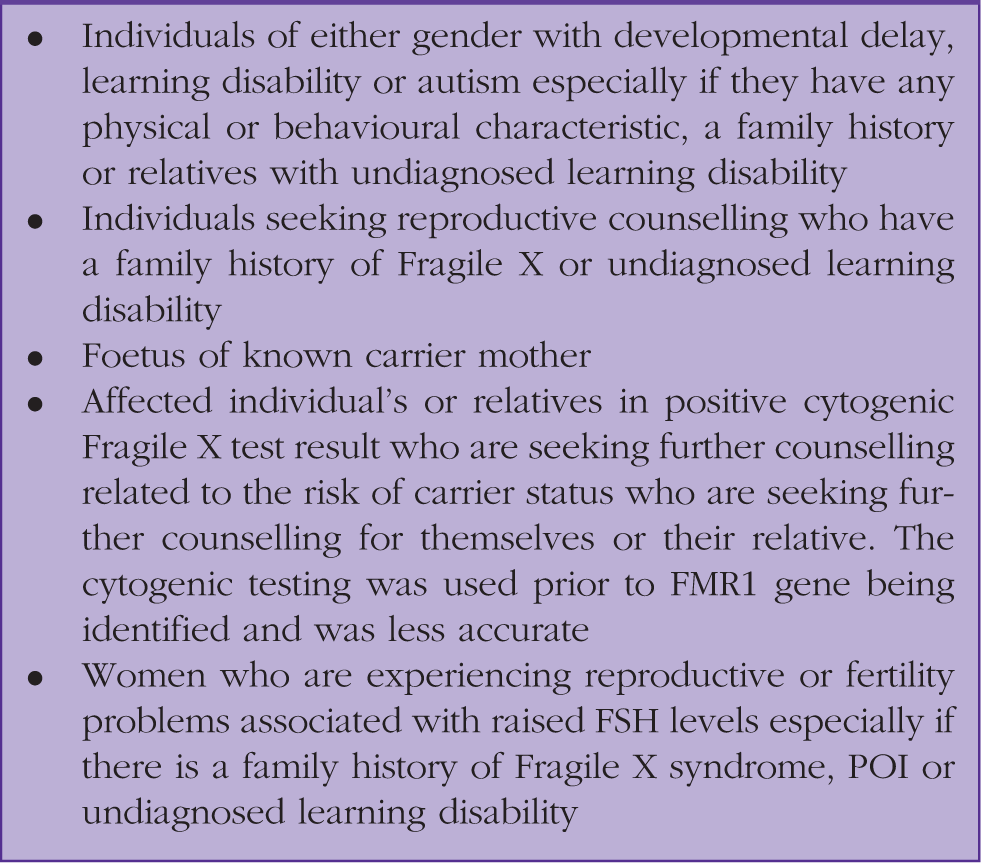
Individuals who should be considered for testing.
Considerations for pre-test genetic counselling.

It is also important to consider that genetic testing is an area of medicine where there have been major advances over the last few decades. It is important to consider that more elderly patients, who may never have been tested or who may have been tested with inferior older tests, may need to be re-tested by either the learning disability team or genetics depending on local protocols (McKechanie et al., 2019).
Clinical case scenario 2.
A 70-year-old man presents to morning surgery accompanied by his daughter. He is attending with a runny nose and productive cough. You notice he appears to have a mild learning disability. He is finding it difficult to process your explanation of his symptoms, which are likely due to viral illness. He does not attend the practice regularly and was last seen 4 years ago. You check the GP records that mention a mild learning disability, but no clear diagnosis is present. You refer him to the local learning disability services and they make a diagnosis of Fragile X syndrome. He has three adult children, all of whom have at least one child already. His daughter is recently pregnant again and is concerned about her likelihood of having a child with Fragile X syndrome. As the daughter is also a patient at your practice, you are able to refer her for genetic counselling. She is offered prenatal testing which she declines due to the risk of miscarriage.
KEY POINTS
Fragile X syndrome is an X-linked dominant disorder that is due to greater than 200 trinucleotide repeat expansions of CGG on the FMR1 gene; having between 54 and 200 repeat expansions may cause a pre-mutation Fragile X syndrome usually presents in early childhood with language and motor delays, but patients may remain undiagnosed until later into adulthood Patients typically have a low IQ (less than 70) and may have behavioural issues such as hyperactivity and autistic-type features Key physical features are large facial features, joint issues and sensory difficulties Patients with a pre-mutation are generally intellectually normal, but are risk of expansion into Fragile X syndrome in future generations Patients with a pre-mutation have a risk of FXTAS and fragile X-associated POI