
Abstract
Clinical decision support systems relating to prescribing are available on general practice information technology systems, with warnings relating to drug–drug interactions and allergies. These tools can help us anticipate and avoid known side effects of drugs, but only after we have selected the drug. Combining these with renal function, liver function, other biophysical markers and pharmacogenomics information, can improve medicines optimisation and reduce adverse effects. Managing all these variables at the same time as conforming to disease guidelines is a challenge. The challenge is even greater when managing multi-morbidity and the associated polypharmacy.
Clinical case scenario: Tamoxifen and interactions
Mrs M is a 65-year-old woman who underwent a lumpectomy for breast cancer 4 years ago. Six months ago she was diagnosed with ischaemic heart disease, presenting with a myocardial infarction. She attends with low mood, struggling with the psychological effects of her diagnoses and the limitation to her daily activities through osteoarthritis of her right knee. Her repeat prescriptions include tamoxifen, simvastatin, aspirin, clopidogrel, candesartan, bisoprolol and lansoprazole. She also takes co-codamol 30/500 when she cannot manage with her knee pain. The consultation involves a discussion of management options for her low mood, including prescription of a selective serotonin receptor inhibitor. She is open to this suggestion, but feels she already takes too many medications that do not offer any immediate benefit to her daily life.
Background: Polypharmacy, multi-morbidity and adverse drug reactions
Mrs M and this complex consultation will be familiar to us all within primary care, illustrating the common challenges of multi-morbidity, polypharmacy, concordance, co-ordination of care and management of the psychosocial dimension.
The vast majority of activity and prescription of medications in the NHS occurs within primary care; every year 1.1 billion prescription items are issued within primary care at a cost of £9.2 billion. However, 50% medications are not taken as prescribed, any medication may only be effective in 30–50% patients, and adverse drug reactions (ADRs) are common, being responsible for 1 in 16 hospital admissions and a significant proportion of A + E attendances (Pirmohamed et al., 2004). Although an ageing population has increased the prevalence of multi-morbidity (MM) and polypharmacy, there are more people with MM between 40 and 60 years of age than people over age 60 with MM.
‘Appropriate’ polypharmacy is beneficial and results in medicines optimisation, medicines use that is evidence-based and optimised. ‘Problematic’ polypharmacy may lead to increased risk of drug interactions and adverse drug reactions, together with impaired adherence to medication and quality of life for patients. (Kings Fund, 2013). MM, defined as two or more chronic conditions, and associated polypharmacy (defined as individuals taking four or more individual drugs) are key challenges facing the NHS including general practice (Barnett et al., 2012; Salisbury, 2013). The recent published National Institute for Health and Care Excellence (NICE) guidance on MM is an attempt to highlight management issues relating to treatment burden (Farmer et al., 2016).
Co-morbidities that are linked together have been defined through a large-scale epidemiology study looking at 1 751 841 patient records from 314 general practices (Barnet et al., 2012). Linked co-morbidities include diabetes, cancer, coronary heart disease, atrial fibrillation, depression and pain conditions. A meta-analysis has shown that 46% of patients on statins, 41% on antihypertensive medications and 30% on aspirin fail to adhere to their medication, including due to side effects (Chowdhury et al., 2013). The key factors that predicted adherence rates in these studies were age, gender, co-morbidity, and polypharmacy.
The decision to prescribe drugs is dependent on many factors, including clinical and biomedical parameters, such as kidney function and liver function. For example, a raised lipid level in diabetes relies on near normal hepatic function before prescribing lipid-lowering therapy. In primary care, clinical decision support systems (CDSSs) already exist and are integrated into information technology (IT) systems, incorporating information such as renal function, co-morbidities and other medications to guide clinicians in safe prescribing decisions at the point of prescription. Additional mechanisms to ensure safe prescribing are regular structured medication reviews (SMRs) and pharmacist expertise. Figure 1 illustrates a decision ‘flow’ for incorporating pharmacogenomics into prescribing decisions regarding medications for multiple co-morbidities.
Drug selection algorithm including the use of pharmacogenomics information.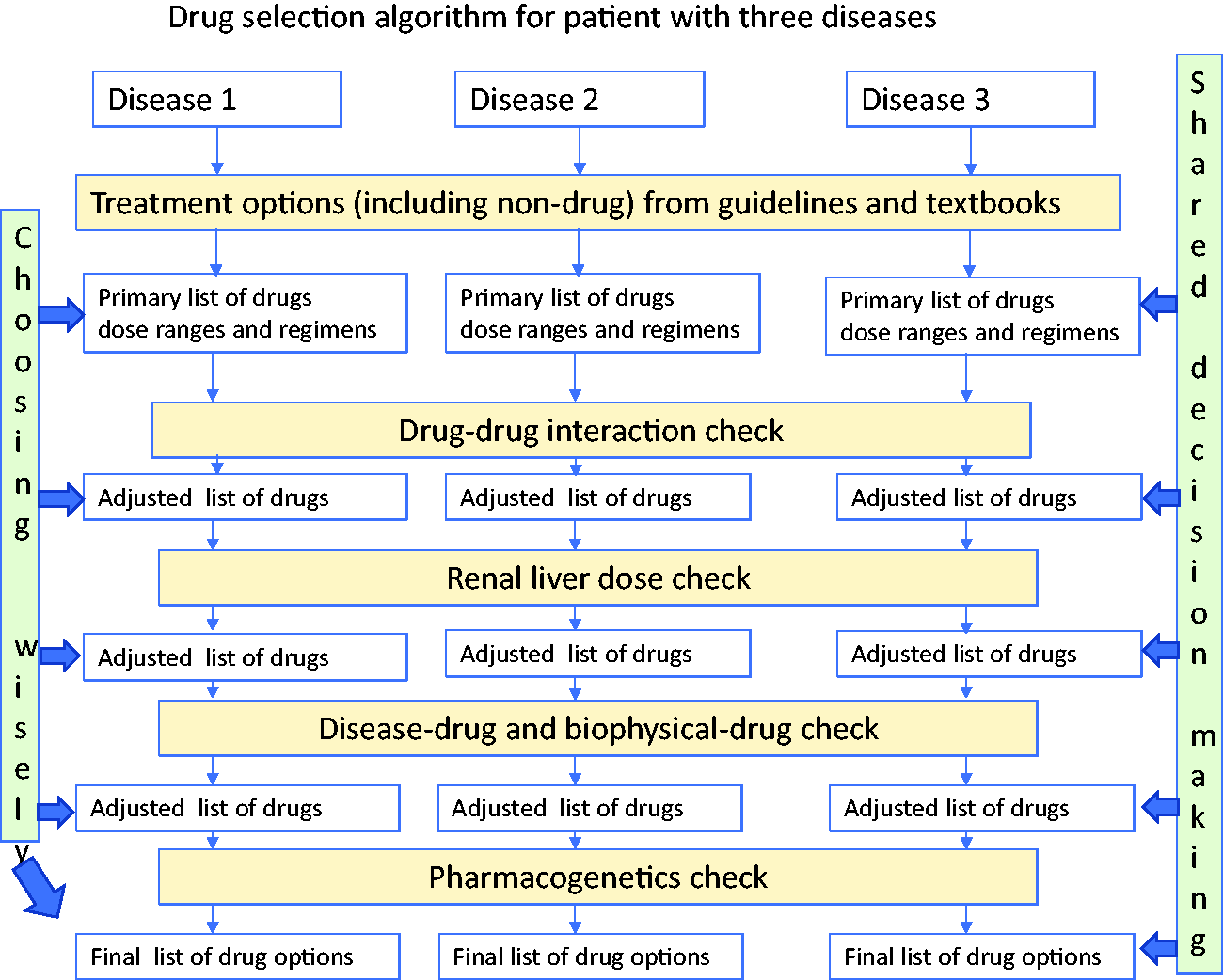
Mrs M has several commonly linked co-morbidities, is at risk of ‘problematic’ polypharmacy and has a high risk of non-concordance. For example, a selective serotonin receptor inhibitor (SSRI) might increase the risk of bleeding if combined with aspirin and clopidogrel, or the liver impairment might reduce excretion of the SSRI and indicate a lower dose. In this way, complex patient information is integrated into the decision process. The same can be done using pharmacogenetics.
Pharmacogenomics and personalised medicine
Pharmacogenomics is the study of genetic variation on drug prescribing. Genetic variation can affect drug metabolism through pharmacokinetic and pharmacodynamic processes. Pharmacokinetics involves the bioavailability (oral administration), drug absorption, distribution, metabolism and elimination (including renal and enterohepatic clearing) of drugs. That last phrase is so important. Pharmacogenetic variants can be used in the same way we use a low estimated globular filtration rate or knowledge about liver fibrosis to alter drug doses. Pharmacodynamics involves the end organ effects of the drug dependent on its receptor binding. Pharmacovigilance is the pharmacological science relating to the collection, detection, assessment, monitoring, and prevention of adverse effects with pharmaceutical products. The Medicines Health Regulatory Agency has a fundamental role in pharmacovigiliance through its regulation of medicines within the UK, co-ordinating activities including the Yellow Card scheme, drug safety alerts, and patient information and Summary of Product Characteristics.
Tangible benefits to the NHS in the use of pharmacogenomics.
Where genetic variation may affect drug pharmacokinetics or pharmacodynamics.

What is meant by stratified medicine and precision medicine?
Stratified medicine is otherwise known or described as personalised, precision, or P4 (predictive, preventive, personalised and participatory) medicine. The UK Pharmacogenetics and Stratified Medicine Network define stratified medicine as the use of genomic testing to ‘prescribe the drug that is most likely to have a positive therapeutic effect, at the optimum dose and in the right combination with other medication, to patients at the start of their treatment’. The majority of prescribing is currently based on the signs or symptoms of the patients disease, however, ‘prescribing patients their treatment based on their genetic profile, molecular basis of their disease, risk of disease, and response to a particular drug therapy improves healthcare outcomes’ (UK Pharmacogenomics and Stratified Medicine Network, 2020).
Improving drug dosing, preventing adverse effects
There have been significant successes already in routine clinical practice around the use of genomic information in prescribing. To date, successes in germ-line pharmacogenomic testing involve testing of single ‘drug/gene pairs’; single combinations of drugs whose metabolism is significantly affected by variation or a polymorphism within a single gene.
The use of Abacavir HLA-B*5701 testing in patients with HIV to reduce severe hypersensitivity reactions is now well-established, and the summary of product characteristics recommends mandatory pharmacogenomic testing prior to prescription. Another example is the prescription of azathioprine in inflammatory bowel disease and other autoimmune disorders. Thiopurine methyltransferase (TPMT) activity is crucial in the metabolism of azathioprine; around 10% of the population carries a genomic polymorphism resulting in TPMT deficiency, giving them a high risk of a myelotoxic effect if azathioprine is prescribed. The Summary of Product Characteristics states that TPMT testing is ‘desirable’ prior to prescription.
There are numerous examples of pharmacogenomic testing to stratify treatment in the field of oncology. Genomic testing of cancer samples is generally performed to detect somatic variants: these are defined variants that are not present in gametes but occur any time during or after foetal development and are present only in some cells in the body. One example is the use of oestrogen (ER), Progesterone (Pr) and Herceptin (Trastuzumab) (Her-2) receptor status, this provides a stratification for treatments that include aromatase inhibitors and the use of immune-targeted therapy in the case of herceptin.
What about medications prescribed within primary care?
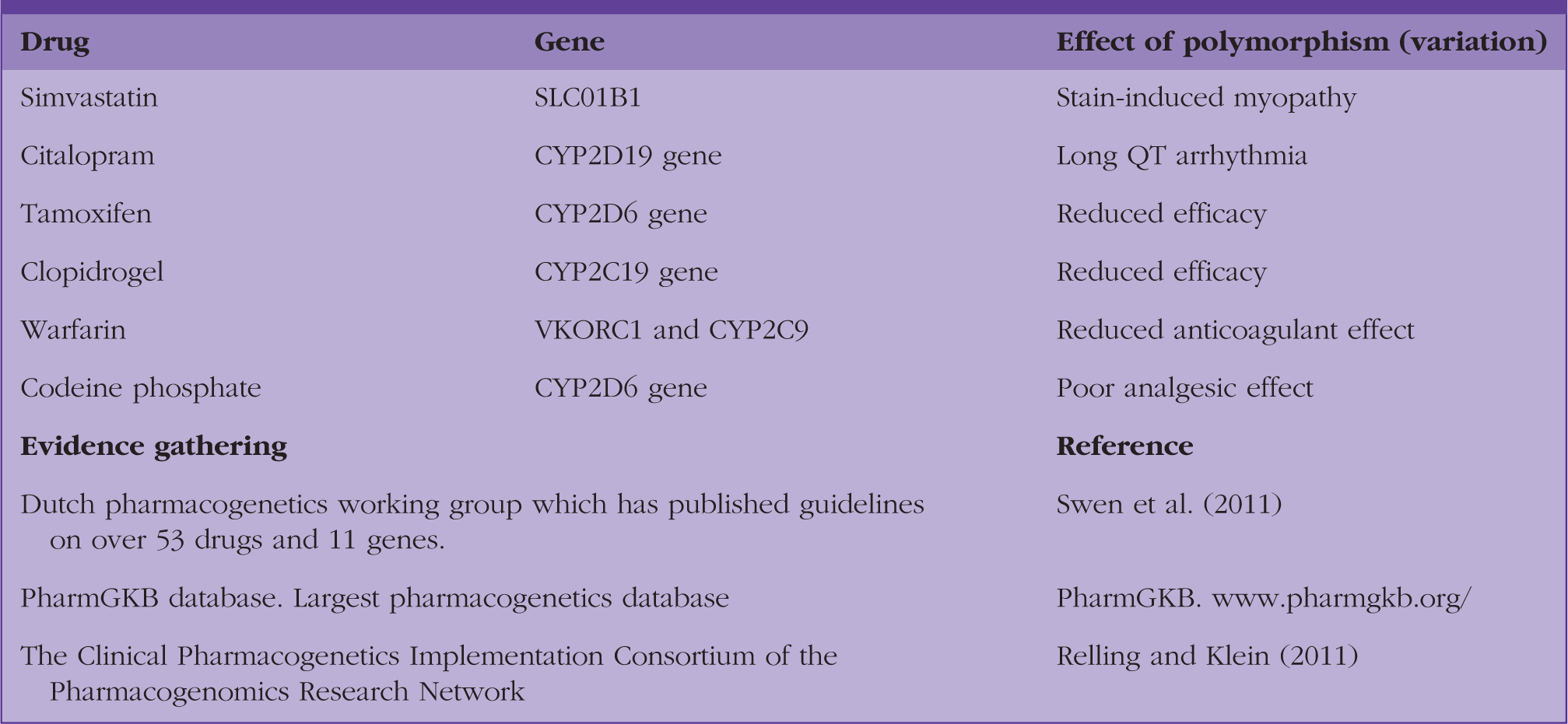
Common drugs, associated genes and effect of variation underpinned by evidence.
Simvastatin
Variants in the SLCO1B1 gene predispose to statin-induced myopathy in patients taking simvastatin. SLCO1B1 gene testing could guide the need for reduced dosing to prevent simvastatin-induced myopathies, or the need to consider an alternative statin (Ramsay et al., 2014).
SSRIs and tamoxifen
Polymorphisms in the CYP2D19 gene result in patients being CYP2C19 poor metabolisers; if citalopram is prescribed, there is an increased risk of arrythmia through long QT interval (Hicks et al., 2015). QTc interval monitoring in these patients is part of the personalised approach to medication management. CYP2D6 polymorphisms can affect the efficacy of SSRIs, for instance a patient may gain therapeutic benefit from low-dose citalopram 10 mg.
Tamoxifen is prescribed as an anti-ER drug, inhibiting the action of estradiol on ER-positive breast cancer cells. Tamoxifen is a pro-drug and is metabolised by CYP2D6 and others to active metabolites 4OH-Tamoxifen, and then by CYP3A4/5 to endoxifen. CYPD6 inhibitors such as SSRIs, for example, can alter the metaboliser status of a patient to poor metaboliser, which means the efficacy of tamoxifen may be affected. The International Tamoxifen Pharmacogenomics Consortium is monitoring what the effects of polymorphisms may have in these cytochrome systems (Province et al., 2013).
Clopidogrel
Hepatic biotransformation of clopidogrel leads to an active metabolite that inhibits the purinergic P2RY12 receptor leading to inhibition of platelet aggregation. This requires involvement through many enzymes and genes within the cytochrome system: CYP 1A2, 2B6, 2C9, 2C19 and 3 A 4/5 (Scott et al., 2013). In patients who are poor CYP2C19 metabolisers, clopidogrel at recommended doses forms less of the active metabolite of clopidogrel and has a smaller effect on platelet function and therefore, efficacy. Clinical trials have demonstrated that polymorphisms in the cytochrome system are associated with increased stent thrombosis (Mega et al., 2008) and Food and Drug Administration (FDA) labelling and the Summary of Product Characteristics state ‘tests are available to identify a patient's CYP2C19 genotype’. Ethnic variations exist, with 30% of Caucasians and African Americans and 60% of Asians having deficient CYP2C19 activity, and therefore, Clopidogrel will have reduced efficacy in these groups. Until recently it was thought that the use of a proton pump inhibitor may affect clopidrogel response, as CYP2C19 is an important pathway for metabolising omeprazole.
Warfarin
Polymorphisms in VKORC1 and CYP2C9(*3) have recently been found to act as important determinants of clinical initial international normalized ratio (INR) response to warfarin dosing (Johnson et al., 2011) . This is an example of both pharmacokinetic and pharmacodynamic genetic effects. Genotype-guided warfarin dosing has been shown in some studies to be superior to standard dosing with respect to the time in the therapeutic INR range.
Codeine phosphate
Codeine is a pro-drug and is activated to morphine through the P450 2D6 hepatic cytochrome. Variation within CYP2D6 gene affects the speed at which an individual metabolises codeine to morphine and are categorised into poor metabolisers (5–10% of the population), normal metabolisers or ultra-rapid metabolisers (1–2% of the population). Poor metabolisers will experience a poor analgesic effect from codeine, individuals who are ultra-metabolisers to morphine experience effects of overdose and even respiratory depression at low doses. For this reason, codeine is contra-indicated in children and in breast-feeding mothers. Codeine metaboliser status may be affected by CYP2D6 inhibitors such as fluoxetine, terbinafine and amitriptyline.
Following recommendations for prescription from single disease clinical guidelines may result in several potentially serious drug interactions (Dumbreck et al., 2015). Returning to Mrs M; she is currently taking tamoxifen, simvastatin, aspirin, clopidogrel, candesartan, bisoprolol and lansoprazole, and co-codamol. Pharmacogenomic testing for Mrs M may reveal genomic polymorphisms that could reduce the efficacy of clopidogrel, predispose her to an adverse drug reaction from simvastatin or co-codamol, thereby affecting concordance, and also influence choice and dosage of an SSRI.
Pharmacogenomic testing
Examples of pre-emptive genotyping that allows informed prescribing as part of practice-based decision support within the electronic health record using pharmacogenomics is exemplified by the Vanderbilt Predict programme (Schildcrout et al., 2012); this has been shown to reduce adverse drug effects.
Pharmacogenomic testing within the NHS currently is limited to testing of single drug/gene pairs with proven cost-effectiveness, usually due to severe or life-threatening ADRs, and are done on a reactive basis. Reactive pharmacogenomic testing refers to testing in anticipation of prescription of a medication with a high-risk ADR, or in response to an unexplained ADR. Pre-emptive testing aims to optimise medication by pharmacogenomic testing for variants within multiple genes (gene panel). There is now demonstrated cost-effectiveness of pre-emptive pharmacogenetics gene panel tests over a patient's lifetime (Alagoz et al., 2015). Results from such testing could be incorporated into CDSSs with other information affecting prescribing, and combined with current guidance to provide information to the primary care practitioner at the point of prescribing (Swen and Guchelaar, 2012).
In primary care, a mouth swab, from which DNA can be extracted for analysis, could then provide pharmacogenomics results. Rather than looking at a panel of gene tests, it might be that we see testing comprising a custom panel of drug–gene pair testing for medications within particular specialties, for example, psychiatry or cardiovascular. In primary care, feasibility studies using pharmacogenetics testing with clinical decision support have been conducted (Dawes et al., 2016). Patients were identified and stratified into the most common presenting in primary care with actionable pharmacogenetics tests as exemplified by Table 1. Dawes et al. (2016) moved away from alerts of what not to give, and instead focused on producing a list of drugs for each condition being experienced by the patient. This list, see Figure 1, adjusts doses and dose regimen that takes into account all the variables discussed above.
Participants within the 100 000 genome project will receive results for some pharmacogenomic testing, the scope of which is under development. Over time, pharmacogenomic testing is anticipated to become more widely available within NHS clinical care via the Genomic Testing Directory, which comprises nationally agreed testing eligibility criteria.
Individuals may access pharmacogenomic testing through commercial routes, ‘direct-to-consumer’ testing. However, limitations of testing may mean that qualified laboratories are not involved or that the variant testing done for those that are not available through the NHS. This could have workload implications for General Practice if consumers then seek medical advice. A RCGP position statement aims to offer advice on this situation (www.rcgp.org.uk/policy/rcgp-policy-areas/genomic-position-statement.aspx).
Other pharmacogenomic examples
Genomics and new drug targets
Loss of function in the PCSK9 gene leads to lower levels of LDL cholesterol, whereas alterations in the genes could cause gain-of-function alterations leading to high levels of LDL and potentially cardiovascular disease. Clinical trials are ongoing.
Repurposing existing drugs
The COVID-19 pandemic has highlighted the potential use of repurposing existing drugs for new diseases. Drugs include azithromycin and dexamethasone. Here genetic variation may positively impact on drug efficacy.
Drug development based on specific mutations
The use of targeted therapy for cancers includes breast cancer (e.g. trastuzamab), lung cancer (e.g. erlotinib), melanoma (e.g. vemurafenib) and leukaemia (e.g. dasatinib ) (Patel et al., 2014). Others include prescribed aromatase inhibitors based on tumour biomarkers (e.g. estrogen status). Ongoing work is necessary to determine how outcomes could be improved. This is particularly relevant in the management of cystic fibrosis where thousands of mutations in the CFTR gene cause differences in function of the cystic fibrosis transregulator. Ongoing drug development work linked to functional improvement (e.g. in forced expiratory volume) could lead to new treatments for this debilitating condition.
Multi-morbidity and stratified medicine
Linked with this is the identification of new biomarkers through genotyping. Biomarkers could be prognostic (e.g. MSI-H for stage II colorectal cancer patients), predictive for efficacy and toxicity. The potential is an increase in the understanding of targets and common biochemical pathways. However, less than one-sixth of FDA drug labels provide convincing evidence of clinical utility of biomarker testing.
Stratification, guiding treatments in General Practice, includes the use of CHA2DS2-VASc risk scoring for stroke with atrial fibrillation and the predicted need for anticoagulation or the QRisk (Hippsley- Cox et al., 2010) score for cardiovascular disease, which provides a population risk for the need for statins. To aid decision making, high-risk drug interactions, such as between simvastatin and a macrolide antibiotic clarithromycin, are highlighted on current GP IT systems.
Stratification in terms of pharmacogenetics is relevant when predicting for efficacy and toxicity across multiple diseases. The presence of genetic polymorphisms or variations within the same gene-affecting drug metabolism can affect not only the drug under study, but also drug interactions based on common (and interacting) biochemical pathways.
Looking for causation and associations such as diabetes-related heart disease may over time be possible and bring in the use of genomic information. For example, in prevention we currently use HBA1c as a marker of glycaemic control over the previous 6–8 weeks and it is also used in screening to identify those at risk of diabetes. Genome wide association studies have already revealed susceptibility loci which may indicate predisposition to diabetes, such as the fat and obesity gene (FTO) and the glucokinase GCK gene. Other areas, such as different microenvironments in the body such as the retina, may offer new genomic biomarkers that could be used to predict for disease. The use of miRNA may in the future be used to be predictive for diabetes.
Future work and implementation
Diabetes, as an exemplar of a long-term condition, may require longitudinal studies to determine the utility of potential markers that take in information from other genomic technologies such as proteomics, the study of proteins expressed by their genes. Whole genome and exome sequencing offer the potential for new marker identification. However, this will require validation, gene annotation, biochemical pathway analyses, possible in vitro and then in vivo studies leading onto clinical trials that validate the use of a biomarker in clinical care.
Implementation: There are barriers to the implementation of pharmacogenetics testing in primary care, including lack of direct commissioning of such tests in primary care or clinical referral pathways, lack of evidence of clinical utility and cost-effectiveness, lack of genomic knowledge, uncertainty in the interpretation of the tests, lack of decision support and also lack of patient understanding. For example, dosing algorithms based on CYP2C9 and VKORC1 polymorphisms do exist, but in clinical practice is limited in uptake as a result of many of the barriers mentioned.
How can we improve drug–drug interactions in the future?
It is likely that NHS England will invest in new technologies for application in clinical practice using genomic information in prescribing. There is hope that it will play a role in single disease and drug prescribing, as well as MM and medicines optimisation which present significant management issues for primary care.
With initial steps being taken towards widespread availability and direct access of pharmacogenomics testing via the NHS Genomic Test Directory, it is important that practitioners and commissioning bodies maintain an awareness of the impact of pharmacogenomics. It is also crucial that other issues concerning implementation are considered: development of supporting IT infrastructure, inter-operability of IT between primary and secondary care, and development of integrated CDSSs with information for primary care at the point of prescription.
Underpinning this will be the necessary pharmacovigilance to enable accurate reporting of common harmful interactions to ensure patient safety and confidence. Access to databases that record this information could then be utilised into clinical decision support, particularly when evaluating multidrug interactions (Finklestein et al., 2016).
KEY POINTS
Pharmacogenomics, the use of genomic profiling to aid prescribing, has enormous potential in management of the primary care-relevant issues of MM, polypharmacy, ADRs and concordance There are already many examples of pharmacogenomic tests guiding decisions when prescribing in secondary care; testing within the NHS is anticipated to increase within the national Genomic Testing Directory and nationally-agreed testing criteria Key questions remain around cost-effectiveness, whether testing should be reactive or pre-emptive, which variants should be included in pharmacogenomic testing panels, and who should be eligible Interventions to manage patients have been hampered by vertical integration between primary and secondary care based on single disease pathways; to date interventions relating to patients with MM have led to mixed effects (Muth et al., 2014; Smith et al., 2012) Pharmacogenomic test results should be considered alongside many other pieces of data for each patient, including renal and liver function, when considering potential medications and doses of medication CDSSs already exist and have been shown to be capable of assimilating all data affecting prescribing and guiding primary care practitioners at the point of care