Abstract
The technical advances of genomic medicine have been well described in recent years, in the medical as well as public media. The social aspects of these advances have significant implications for primary care. GPs have previously ‘done genomics’ simply by the act of taking a family history from a patient and interpreting that history as part of ordinary care. Even at the level of a family history, genomic practice inevitably involves people other than that patient, and from that fact all the social and moral complexities arise. The scientific progress in current genomic research is creating a sphere of knowledge and information that GPs will need to be increasingly familiar with now and in the future. These advances offer opportunities and challenges for the health of communities and the learning needs of all GPs [see Box 1].
Clinical case scenario 1.
E has a screening test at work for cholesterol, as it was on offer to employees. He turns out to have a fasting lipid profile as follows: Total cholesterol 7.5 mmol/l LDL 11 mmol/l. He presents to his GP with a printout of his results, who suspects familial hypercholesterolaemia. A repeat lipid profile is similar. E reports that father died of cardiovascular disease in his 40s. The GP refers E to the local lipid clinic, then wonders about E’s sister who is also his patient.
General genomic issues
Confidentiality
GPs have previously considered genomics through ‘family history’. By exploring family history, we seek to identify risk factors in our patients that may have hereditary factors, and then reduce risks to health and lifespan as a result. This reduction in risk might be through behaviour modification (e.g. quitting smoking), medication (such as prescribing statins) or even surgery (e.g. mastectomy and oophorectomy). However, even in the taking of a family history, information about people other than the presenting patient is being sought and gained. It is being recorded in the medical records of presenting patients. This is an ethical issue that is accepted tacitly as an inevitable by-product of patient care. Patients do not usually seek consent from family members before answering questions about family history. However, as technology in information sharing advances, the retention of their information in the records of index patients is likely to become an overt issue (Royal College of Physicians, Royal College of Pathologists and British Society for Human Genetics, 2011). We suggest that a grounding about confidentiality in the primary care context is essential in managing genetic and genomic information regardless of whether this takes the form of information about family members or the results of genetic tests (Knight and Papanikitas, 2018; Slowther, 2010).
In Case 1, the patient presents with evidence of a monogenic disease of known importance to his long-term health, and also, due to the GP’s duty of care to another family member, a dilemma for the GP is created. Should he (she) contact the sister of the patient to reveal the family diagnosis, or should the decision be left to the patient himself? Normal confidentiality regulations would suggest that the GP should simply leave the decision to the patient himself, but there are powerful arguments against this course of action.
Can the patient be relied upon to share the information? Perhaps the two siblings do not get on in some way, and unless the GP intervenes, the sister may never be aware of her family risk. The ethics of this kind of situation are straightforward when families consider their heritable risks to be a ‘shared account’ (Lucassen and Farsides, 2017). They become complicated when persons at genomic risk do not wish their relatives to be informed about such shared risks. We might posit a ‘right to know’ about such risks on behalf the index patient’s relatives for example.
Although recently more helpful (Dyer, 2020) the law in the UK does not always help clinicians to resolve conflict between family members about the sharing of potentially harmful genomic information. Traditionally, the law has maintained the duty of confidentiality with the ‘index’ patient, however, a recent English case has developed the notion that clinicians should balance the harms in sharing or not sharing genomic information between family members where the index patient claims confidentiality (Dyer, 2020). These are not easy situations to manage, and GPs should take expert council if involved in such cases. GPs might for example be happier to override the patient’s confidentiality if there were a risk of breast cancer rather than of a form of hyperlipidaemia with much lower associated risk.
Consent
The principles of consent are well established in UK general practice (Walters and Metcalfe, 2016):
Decisions should be made by anyone with the capacity so to do Decisions should be fully informed Decisions should not be coerced by others Decisions should be allowed to be changed by the decision maker
These aspects are consistent with making a fully autonomous consent to a diagnostic procedure, treatment or any other intervention. We might add that the degree of information needed in any intervention should cover the nature, purpose, benefits and harms attached to it. It is sometimes worth reflecting on what constitutes benefit and what constitutes harm in the context of healthcare. It is also worth reflecting on the situations where the benefits are so small, and the harms are so great, that shared decision-making is not possible (Ives et al., 2018). This, so far, is uncontroversial, but when applied to the genomic field can get a little more complicated. Consent also requires that the person consenting understands the nature (e.g. blood test or cheek swab) and purpose (e.g. to give details about health risks, ancestry, inform research or identify criminals!) of what is being consented to.
Clinical case scenario 2.
F presents to her GP one day with her daughter G, who is 7 years old. Her relationship with G's father has broken down after several years of a ‘rocky' relationship. Partially as a result of this, F is wondering about the paternity of G. She would like to be clear about who G's father is as there were several possibilities…
She asks if the GP can arrange paternity testing on F ‘to sort things out'.
Most of the time seeking and gaining consent is straightforward, given the components described above. If the father consents (otherwise how will we know what his genotype is?) and both are committed to raising the child together and this is in the daughter’s interests, for example to identify a condition that is treatable in childhood, then there may be no ethical conflict. In Case 2 this clearly is not the situation and a question like this should involve legal advice. Conducting a paternity test using the father’s genetic material (e.g. from a toothbrush) without his knowledge and consent is illegal in the UK (Human Tissue Authority, 2016). G is probably not, by virtue of her age, in any position to consent to paternity testing by genomic means. The candidates for paternity may not be willing to submit to testing. Any justification for F to consent on her behalf must rest on an assessment of it being in G’s best interests, at the very least, and it is difficult to imagine any circumstances when that might be so. Generally, genetic testing is held back until children are capable of understanding the nature, purpose etc. of the test and it is clearly in their best interests (British Medical Association, 2019). Paternity testing is not offered on the NHS. It is only appropriate for doctors to signpost patients to a list of approved providers (www.gov.uk/get-a-dna-test) rather than actually organising a test. Similar issues arise when children may be subject to familial illnesses that could affect their future health and longevity. For example, in families where Huntingdon’s Disease exists, this autosomal dominantly inherited trinucleotide repeat gene can be identified in childhood by molecular testing, so decisions often have to be made about the testing of children who are the offspring of Huntingdon’s parents. Consent for such tests should follow the guidance above.
When someone consents to genetic testing we may need to consider whether their relatives may also have a ‘right not to know’. An example is a patient attending after they find out an uncle has a BRCA2 pathogenic variant, but their mother has not been tested. Clinical genetics would always want to test family members sequentially unless the intervening relative is ‘unavailable' to avoid implicit testing of obligate carriers, which then negates the mothers ‘right not to know.’
Across generations: Public health genomics
Historically speaking, much literature has been devoted to the possibility of preventing genomic disease by interrupting its transmission across generations. Broadly speaking this has been termed ‘eugenic’ and has not usually been seen as morally right. Though there have been programmes that seek to reduce genomic disease in future generations that are, at least arguably, ethical. In Cyprus, thalassaemia has been virtually eliminated by a national intervention involving testing of parents, health education and the avoidance of potential ‘risky’ pregnancies (Hoedemakers and ten Have, 1998). Furthermore, this has happened simultaneously in the two communities of the Greek-Cypriot south and Turkish-Cypriot north. This programme involved primary care clinicians among others in successful reduction of the incidence of thalassaemia. Clearly there are ethical arguments against ‘interfering’ in nature in a way that counters ethical arguments that favour health promotion.
Closer to home, GPs are involved in counselling consanguineous couples in some communities, where it is known that the children of these couples have a higher incidence of congenital disease (Rafi and Spicer, 2018). Clearly such counselling would be non-directive, with the aim of providing information about the nature of such risks to future children and family members.
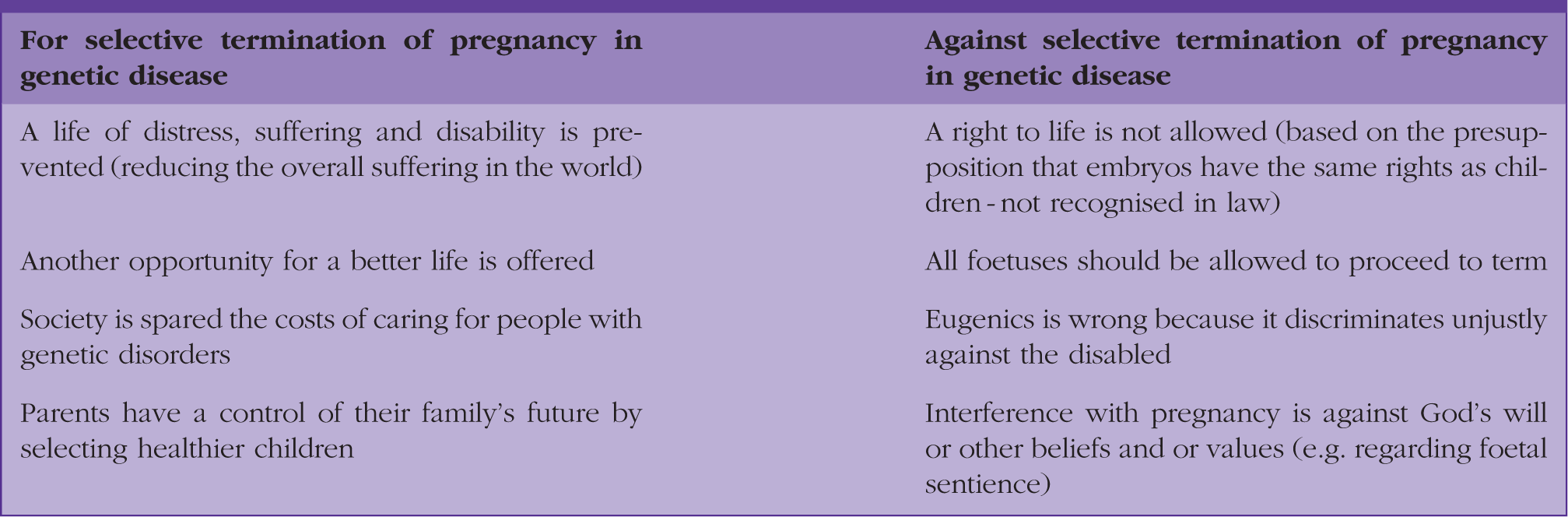
More contested is the ethical justification for preventing the birth of children who may be damaged in utero by a wide variety of genomic abnormalities.
Clinical case scenario case 3.
H and J have been married for 10 years and have had some difficulty conceiving, however, they are now experiencing their first pregnancy. H is known to be a carrier for Alport Syndrome, and she undergoes prenatal diagnosis. The result confirms the foetus is affected. They discuss the matter several times and are confused as to what to do about the pregnancy: they turn to their GP for help.
GPs will, both as clinicians and as ordinary citizens (Papanikitas, 2018), have their own views on abortion. Whatever they may be, they will have a duty of care to patients such as H and J; as such they will want to offer them the support they need as they come to a decision. There is a professional expectation that any advice should be non-directive (Aung and Knight, 2020), and that might be difficult if the decision that H and J eventually make is counter to the GP’s own philosophical position. Contact with the genomic medicine centre will usually be necessary, as will some knowledge of the disease in question and the likely course of events should the foetus go to term and birth.
Summary arguments in selective termination of pregnancy.
Emerging genomic issues
The 100,000 Genomes Project and its successors
Many people are now enrolled in the 100,000 Genomes Project, which has several laudable aims (NHS, 2018):
To increase understanding of genetic variants leading to new treatments and diagnostics To accelerate the uptake of advanced genomic medicine integrated into the NHS To promote greater public understanding of the benefits of genomic medicine To stimulate the UK life sciences industry and commercial activity in genomics
The project aims to expand personalised medicine, where treatments are targeted to individuals rather than populations. GPs are seeing this kind of personalised approach particularly in cancer care, but in years to come it may spread across many domains of healthcare. There will be a need for primary care teams to learn more about the delivery of such a mode of treatment, and for GPs involved in commissioning, deciding how to go about funding such programmes. Successor projects include the Accelerating Detection of Disease programme, currently recruiting 5 000 000 subjects, to examine disease patterns genomically with artificial intelligence methodology (Digital Health, 2019).
By comparison, the National DNA database, operated by the UK Home Office, is a similar large inventory of genomic information. It is used for a very different purpose, in identifying criminals from genetic material recovered at crime scenes. This material is ‘matched’ to the genomes on the database. Some observers have suggested that all our genomes should be recorded in a similar way to enable matching with diseases. Although a utilitarian justification could be advanced for both large scale projects, clinicians will probably be more persuaded by the 100,000 Genome Project than the National DNA database! As an illustration of consent, the nature of collecting genetic material may be similar for both databases but their purposes differ wildly.
Insurance
GPs often have to give information to insurance companies on their patients, where there is a need to assess risk of future illness or death for financial reasons. On one level this is ethically unproblematic: explicit consent is gained from the patient by the company and GPs make available any report that is written to the patient. This consent can absolve the GP of any legal breach of confidentiality inherent in the process. There are several ethical complications, nonetheless. First, family history may be passed on, and as described above, there is no notion of consent by the family members to whom the history refers to such a transfer. Second, if the patient has had some form of adverse genetic testing result, it might give the insurance company a reason to refuse a policy, and thus create a ‘genetic underclass’ that is uninsurable as it represents a poor investment risk. The UK has devised a solution to this problem, known as the Code on Genetic Testing and Insurance (Association of British Insurers, 2019) and under this guidance GPs do not have to disclose information on their patients predictive genetic testing for life policies under £500 000 (with variations for other policies). Huntingdon’s Disease is excluded and does require declaration. In essence this is an example of an ethically driven practical arrangement to protect patients at a special health risk from the social effects of that risk. It is representative of observation of the principle of solidarity, over mutuality.
Incidental or secondary findings
The growth of genomic testing in recent years has led to the discovery of unexpected findings in investigations. This might be similar to (for example) discovery of non-paternity (not the parent expected) in the investigation of a couple’s genetic symptoms. Another kind of unexpected finding is where one kind of genetic abnormality is being looked for but another is found as in Case 4 below.
Clinical case scenario 4.
L is six-year-old girl who has a complex set of physical issues. She is referred for genomic testing by her paediatrician, and turns out to have, among other things, an altered BRCA2 gene.
This is imparted to her parents at an outpatient appointment. In a letter to the GP, this summary is reported. The GP sees L and her parents and considers what she should do next
Adapted from Lucassen and Farsides (2017)
L’s biological parents inevitably are the source of the BRCA2 gene and thus far were unaware of that fact, which will clearly have implications particularly for her mother, and her wider family in terms of cancer risk. Counselling of the risks of bearing the BRCA2 gene may not yet have implications for L herself, but will need to include L’s mother. Thus the GP should refer her to clinical genetics for counselling. If the parent refuses this referral or indicates they are unwilling to share the information with others who could be affected, the GP should seek advice.
Findings may also be generated by people who have their genome tested outside the NHS, by commercial bodies. As well as giving ancestry information, such widely available procedures will only test a small proportion of the genome (looking for single nucleotide polymorphisms) and can report increased risks to many diseases. It is as yet unclear as to the extent that the determination of risk is realistic, and the GP is left trying to decide what further investigation via the NHS might be needed to asses such a risk. Arguably, this is a process not consistent with the principle of equity, where genomic tests which are not evidence-based play into the future healthcare choices of individual patients
Education, resource commitment and workload relating to genomics
A packed debate at the RCGP annual conference in 2018 exposed a need for GP education and disquiet about the resource and workforce implications for primary care presented by genomic medicine. Concerns included the idea that GPs were already at maximum capacity without the introduction of a new technology of unproven efficacy (Dickenson et al., 2019).
According to Samuel and Farsides (2018), staff working at or with Genomics England raised organisational tensions about implementation: whether the ‘cash strapped busy’ NHS and its ‘stressed and busy’ staff not trained in genomics would deliver the project. In an ethnographic study of personalised medicine at a London cancer centre, Day and colleagues found that as experienced clinicians were directed to back-office and laboratory activities, the patient-facing aspects were delegated to clinicians without expertise, who had to follow protocols (Day et al., 2017). GPs and GP trainees, accordingly, need to be aware of how different services might operate (such as personalised treatment for cancer, or identification of additional cardiovascular risk requiring early treatment with a statin) and when and how to engage with each new, additional service.
Five key questions to ask someone contemplating a genomic test and 5 key points bear in mind about direct to consumer genomic testing.

Notwithstanding these sensible caveats, as genomic research is translated from the laboratory to the consulting room, primary care teams will inevitably find themselves with learning needs as a result of emerging science. One good example of this is in cardiovascular care where traditionally GPs have assessed risk by means of scoring systems such as QRISK2 ([soon to be QRISK3) (Hippisley-Cox et al., 2019). Such risks are shared with patients with the aim of reducing personal risk of cardiac events. QRISK2 includes a family history factor as it stands, but in years to come personal genetic risks based on formal testing will be included in the risk assessment. Genomic testing, family history and conventional cardiovascular parameters (lipids, etc.) when combined will provide assessment of personalised risk much greater and more accurate than is possible from the individual component parts (Middlemass et al., 2014). The hope is that patients’ access to better, more comprehensive information about personalised risk, with guidance from informed GPs, will enhance patients’ decision-making when they consider their futures and some life choices.
Summary
Further reading.
KEY POINTS
Genomic medicine can involve the health and confidentiality of people in families who are not the presenting patient There are many people with a possible interest in a patient’s genomic data, including family members, researchers, insurance companies and even the police! Clinicians now have a legal duty to weigh the interests of the patient’s known relatives, when the patient does not which to share a significant finding that could affect those relatives; the normal rules on consent and confidentiality apply, mediated by the needs and interests of family members Any question regarding genomic testing that involves conflict between family members may require medicolegal advice; if in any doubt advice can be sought from medical indemnity bodies or clinical genetics departments GPs will need to maintain their continuing education in genomics as the 21st century proceeds, to maintain their duties of care to their patients GPs need to know when and where to refer for specialist advice on the variety of issues arising from more genomic knowledge and more widespread use of testing The difference between genetics and genomics.