
Abstract
As cancer treatment improves and survival rates continue to increase, clinicians are seeing increasing numbers of patients with metastatic bone disease (MBD). This term describes cancer that has originated in another organ and subsequently spread to the bone. It is a condition that can severely impact the quality of life for an individual and the treatment is often not curative. This article aims to cover the management of MBD, from early recognition to secondary care interventions. The care of individuals with MBD is evolving in the UK, with the development of specialist regional referral pathways to facilitate prompt and timely management.
Clinical case scenario.
John, a 73-year-old gentleman, attends a routine GP consultation complaining of left-sided groin pain. The pain has worsened over the last 2 weeks and has not improved with basic analgesia. The pain is dull and aching in nature with some radiation down his left thigh. He denies any history of trauma and is able to mobilise independently. John's prostate cancer was diagnosed 3 years ago and he is on hormonal treatment. The pain is now impacting his everyday life and John is eager to understand what is causing his symptoms.
Background
Over the last decade, the incidence of all cancers has risen in the UK. Bone is the third most common site of tumour spread, following the lungs and liver (Coleman, 2001). The incidence of bony metastasis in all cancers is approximately 3–5%, which rises significantly to 19% in cancers affecting the prostate, lung and breast (Challapalli et al., 2020). Skeletal metastases are a possibility in any cancer, but are more commonly associated with malignancies of:
Prostate Breast Lung Thyroid Kidney Myeloma
Pathophysiology
Metastatic bone disease (MBD) is usually osteolytic or osteoblastic in nature depending on the radiological appearance and originating tumour. Metastases from the lung, thyroid and kidney are lytic (Fig. 1(a)); whereas in contrast, prostate metastases typically develop into sclerotic lesions (Fig. 1(b)). Breast cancer metastases often behave in a mixed osteoblastic and osteolytic nature. Osteolytic and osteoblastic lesions occur in response to the factors secreted by the various cancer cells. These factors promote either bone formation, destruction or both.
(a) Osteolytic X-ray of a humerus secondary to renal cell cancer. (b) Osteosclerotic X-ray of a femur secondary to prostate cancer. (c) Osteolytic X-ray of a femur secondary to breast cancer.
Signs and symptoms
The most common symptom patients present with is pain. This is normally experienced around the site of the metastases, although sometimes can be referred to other areas from the affected structure. This pain is caused by the release of cytokines and neuropeptides acting on the endosteum and subsequently the periosteum, as the tumour affects cortical bone. Particular attention must be given to any patient presenting with musculoskeletal pain and a background of cancer. Commonly, patients report functional pain, describing pain that comes on when completing everyday activities or experience difficulty weight bearing. Importantly, simple analgesia normally has no effect on relieving this pain, which can help differentiate it from other musculoskeletal problems. Functional pain is also a more accurate predictor of MBD, compared with those who experience pain at rest.
Other symptoms of MBD are predominantly associated with complications of the disease and include hypercalcaemia, myelosuppression, metastatic spinal cord compression (MSCC) or pathological fractures. Common sites for bony metastasis include:
Spine Pelvis Ribs Skull Long bones
In the case study, John presents with atraumatic left hip pain that does not improve with simple analgesia. In view of his background of prostate cancer these features are highly concerning, and further assessment is urgently required.
Pathological fractures
Evidence suggests that up to 30% of patients with MBD will sustain a fracture, and approximately 15% will go on to develop MSCC, highlighting the importance of early recognition (Agarwal and Nayak, 2015; Loblaw et al., 2003). Pathological fractures from MBD usually arise from innocuous injuries, or simple everyday activities, acting on pathological bone to cause an atraumatic fracture. If considered early enough, weakened areas of bone that have been altered by the metastatic lesion can be identified using X-ray, computer tomography (CT) or magnetic resonance imaging (MRI). These areas are identified as an impending pathological fracture and treatment can be sought.
Metastatic spinal cord compression
MSCC is an oncological emergency whereby the tumour has spread to the spine causing compression of the spinal cord. This will require immediate secondary care assessment, with the referral to either, medical, spinal or oncology specialties depending on the services in your local area. The condition may present without previous diagnosis of MBD; therefore, it is important for clinicians to be vigilant in any patients presenting with possible symptoms of MSCC who have a known cancer. Common symptoms include bowel and bladder dysfunction along with altered lower limb neurology. The complications of MSCC can be permanent and irreversible if not diagnosed and treated early. Particular consideration must be given to all patients with prostate cancer presenting with lower back pain, as the rich venous plexus surrounding this organ allows local spread into the spine and subsequent MBD.
Hypercalcaemia
Hypercalcaemia in malignancy presents with symptoms such as nausea, vomiting, lethargy, constipation, abdominal bloating, reduced appetite and confusion. The raised calcium levels are caused by increased bone reabsorption, which occurs in osteoclastic activity. Although hypercalcaemia can occur without MBD, its presence increases the chances of this being seen.
Myeloma
Up to between 70 and 95% of patients with Multiple Myeloma (MM) will go on to develop MBD (D'Oronzo et al., 2019). MM tends to appear as a lytic bone lesion on X-ray and CT images, with its MRI findings classified into normal, focal, diffuse, and typical salt and pepper pattern (Park et al., 2018).
Bone sarcoma
Bone sarcomas are primary tumours arising from mesenchymal bone cells. Most sarcomas arise in the appendicular extremities and occur in children and young adults, with the most common symptoms being either pain, or a newly identified mass (Mavrogenis and Ruggieri, 2013). Despite this, as bone sarcoma can present as an isolated lesion, a singly solitary bone lesion should not be presumed to be a metastasis.
Examination
When examining a patient with MBD there are a few key things to assess. Initially during general inspection, examine for any soft tissue swellings, lumps or masses, particularly around the site of pain. Confirming the exact site of pain is important, as pain experienced in the middle of a limb away from the joint capsule is highly suspicious for a metastatic lesion. Particular attention should be given as to whether the examination findings of tenderness are disproportionate to what you would expect from the proposed mechanism of injury. Comparison with the contralateral joint can be helpful in assisting with this comparison.
Reviewing the case study, assessing John’s ability to stand on one leg would be a useful functional test to evaluate the situation, as the inability to weight bear on the affected limb is a concerning feature of an impending pathological fracture. Groin pain is a common presentation of referred spinal pathology. In view of his recent history of prostate cancer, it would be important to fully examine John’s neurological status and spine to ensure there is no evidence of MSCC.
Diagnosis
Although skeletal metastases are a common cause of morbidity in cancer patients, advances in both surgical and medical management, along with improvements in the multi-disciplinary approach have led to increased survival rates (Taylor and Kumar, 2017). Many of these patients present late, with vague symptoms, therefore identifying MBD can be difficult. Often the diagnosis of MBD is only made following a hospital admission where a fracture is identified to be pathological in nature, or in an acute emergency situation with sudden symptoms of MSCC. Other patients are referred as outpatients to an orthopaedic clinic, where following further imaging, the discovery of bony metastasis may be the first manifestation of widespread malignancy.
Making an early diagnosis is paramount in order to improve patient outcomes from this condition. As clinicians, having a high index of suspicion for anyone with known malignancy presenting with musculoskeletal pain is key. Routine blood tests can be performed in the community; they include a full blood count, liver function tests, renal function, bone profile, C-reactive protein, erythrocyte sedimentation rate, tumour makers and a myeloma screen. Derangements in these results may help point to this diagnosis; however, imaging modalities can be used to support diagnosis. Although MRI remains the gold standard radiological test for identifying and assessing these lesions, the use of X-ray and CT imaging are often more readily available in the community, and can be used to support your diagnosis (Issac et al., 2020; Messiou et al., 2009).
In John’s case, urgent blood tests including a prostate-specific antigen (PSA) may help to diagnose disease recurrence. Urgent X-ray imaging of the affected femur, hip and pelvis should be performed to assess for sclerotic lesions commonly seen from prostate malignancy (Fig. 1(b)).
Secondary care referral
Urgent referral to specialist services will vary depending on your practice’s location; however, an urgent referral should be made to the appropriate specialist to ensure prompt assessment. Although the pathway for a 2-week wait referral direct to a metastatic bone cancer specialist does not currently exist, an urgent referral should be made to either the local MBD team or orthopaedic unit or back to the oncology team, depending on your local area. Of note, according to recommendations from the British Orthopaedic Oncology Society (BOOS) and British Orthopaedic Association, each Trust should have a nominated lead clinician for the management of patients with MBD (BOOS, 2015).
Assessment in secondary care
Following specialist intervention, further imaging can be used to assess more widely for disease progression, in the form of a CT thorax, abdomen and pelvis and an isotope bone scan. These allow a more detailed assessment of the primary tumour, while allowing identification and the distribution of further metastatic spread. This also enables differentiation between new primary lesions and metastatic deposits. A multi-disciplinary team (MDT) discussion will then review these images, alongside further results such as blood tests and histology to formulate a treatment plan. This includes determining the diagnosis, staging the disease and discussing the likely prognosis. The team will then consider the patients functional status before deciding whether conservative, medical or surgical management is appropriate. Patient choice remains fundamental in the decision-making process and early involvement following the MDT discussion remains paramount.
Pathological fracture risk assessment
Mirel’s scoring system used for prediction of pathological fracture.

Size is defined by fraction of cortical thickness,
Source: Mirels (1989).
Role of bone biopsy
In many cases, where the primary site is known and there is widespread disseminated disease, it is not necessary to perform a bone biopsy. However, in cases where there is any doubt regarding the origin of the lesion a biopsy is indicated. This allows the MDT to distinguish whether the lesion is a new primary or instead a secondary lesion, which significantly alters the management.
Management
The high risk of fracture in MBD means that management decisions should be made quickly, and where possible, early in the disease. The role of the primary care physician is to identify at risk patients early, perform suitable initial investigations and ensure prompt referral onwards to secondary care. The key aim is to prevent pathological fractures. The psychological effects of the diagnosis can be vast, and so continued support in the community is important. Management decisions are complex and depend on a number of variables including extent of disease (localised or widespread), cancer type, patient’s prognosis, previous treatment, general health and most important, the patient’s preference.
Conservative management
In some cases, conservative treatment may be the best management option for the patient. This may be based on patient preference, or unsuitability to progress to either medical or surgical options. Conservative treatment options include the use of physiotherapy to increase strength and mobility. Assistance devices such as walking aids or spinal braces can be used to help the patient cope. The low-energy mechanisms that are associated with pathological fractures mean that soft tissue damage is often minimal; therefore, effective immobilisation can make the patient much more comfortable.
Medical management
There are many different medical treatment options for people with MBD depending on the patient’s symptoms, extent of the disease, overall physical health and their own personal preference. Pain is the predominant symptom, with cancer-induced bone pain considered particularly difficult to treat. Initial treatment should ensure that analgesia is provided based on the World Health Organisation’s analgesic ladder, with studies highlighting that 73% of patients achieve adequate pain relief utilising these principles (Kane et al., 2015). Non-opioid analgesics such as paracetamol and non-steroidal anti-inflammatory medications have limited effect, although should be trialed first. Weak opioids such as codeine and tramadol provide minimal benefit, so where clinically appropriate this step is often omitted (National Institute for Health and Care Excellence, 2020). Strong opioids form the mainstay of treatment; therefore, primary care clinicians should have a low threshold to initiate oral preparations such as morphine or oxycodone, or transdermal opioids such as fentanyl or buprenorphine (Bennett et al., 2012). Early specialist involvement of the palliative care team should be sought in those patients whose pain remains poorly controlled.
Increasingly, medications commonly used in osteoporosis management such as bisphosphonates and denosumab have been used in patients with MBD (Coleman and McCloskey, 2011; Fizazi et al., 2009). Although the specific action of these medications may differ, they both aim to inhibit osteoclast destruction and increase bone resorption. Evidence has shown that these medications, if used early in the course of the disease, can reduce pain and delay the time until fracture, subsequently improving a patient’s overall quality of life (Jehn et al., 2016). Chemotherapy may be suggested for patients where the disease is more widespread, while hormone-specific treatments are used for specific types of cancer, including breast and prostate.
Radiotherapy can be an effective treatment intervention for MBD and can be used on its own, or alongside surgery. The main aim of radiotherapy is to reduce pain and improve a patient’s quality of life. High-dose ionising radiation is used to reduce osteoclast activity and kill tumour cells, which reduces tumour volume and the effect on local nerve fibres that cause pain (De Felice et al., 2017). Response to radiotherapy depends on the origin of the lesion, with different cancers having different sensitivities. The analgesic benefits can start to take effect from short days to weeks following therapy but may take up to several months for full effect.
Surgical management
Indications for surgical intervention fall broadly into three categories, to:
Improve survival Alleviate symptoms and improve quality of life Prevent fracture
Prior to surgery a multi-disciplinary discussion should take place to review the appropriateness of surgery and the best time for this to be undertaken. Surgical options must be appropriate for the stage of the disease, the patient’s overall health, and be communicated clearly with the patient to allow an autonomous decision to be made. It has been recommended that surgery should only be undertaken in patients whose life expectancy is at least 1 month for a weight-bearing bone and 3 months for a non-weight-bearing bone (Healey and Brown, 2000).
When surgery is not curative, its role is to restore mobility, improve function, provide pain relief and improve quality of life. The surgical fixation should allow for weight bearing of the affected limb and aim to last throughout the remainder of the patient’s life. Surgical fixation can include open reduction and internal fixation, where the lesion is internally stabilised (Fig. 2(a)), or excision arthroplasty, where the lesion is excised and replaced with a metal prosthesis (Fig. 2(b)). Surgery may be undertaken prophylactically in patients who are deemed to have a significant risk of impending fracture.
(a) Curettage with cement augmentation and fixation for renal cell cancer metastases. (b) Hip hemiarthroplasty for prostate cancer metastases.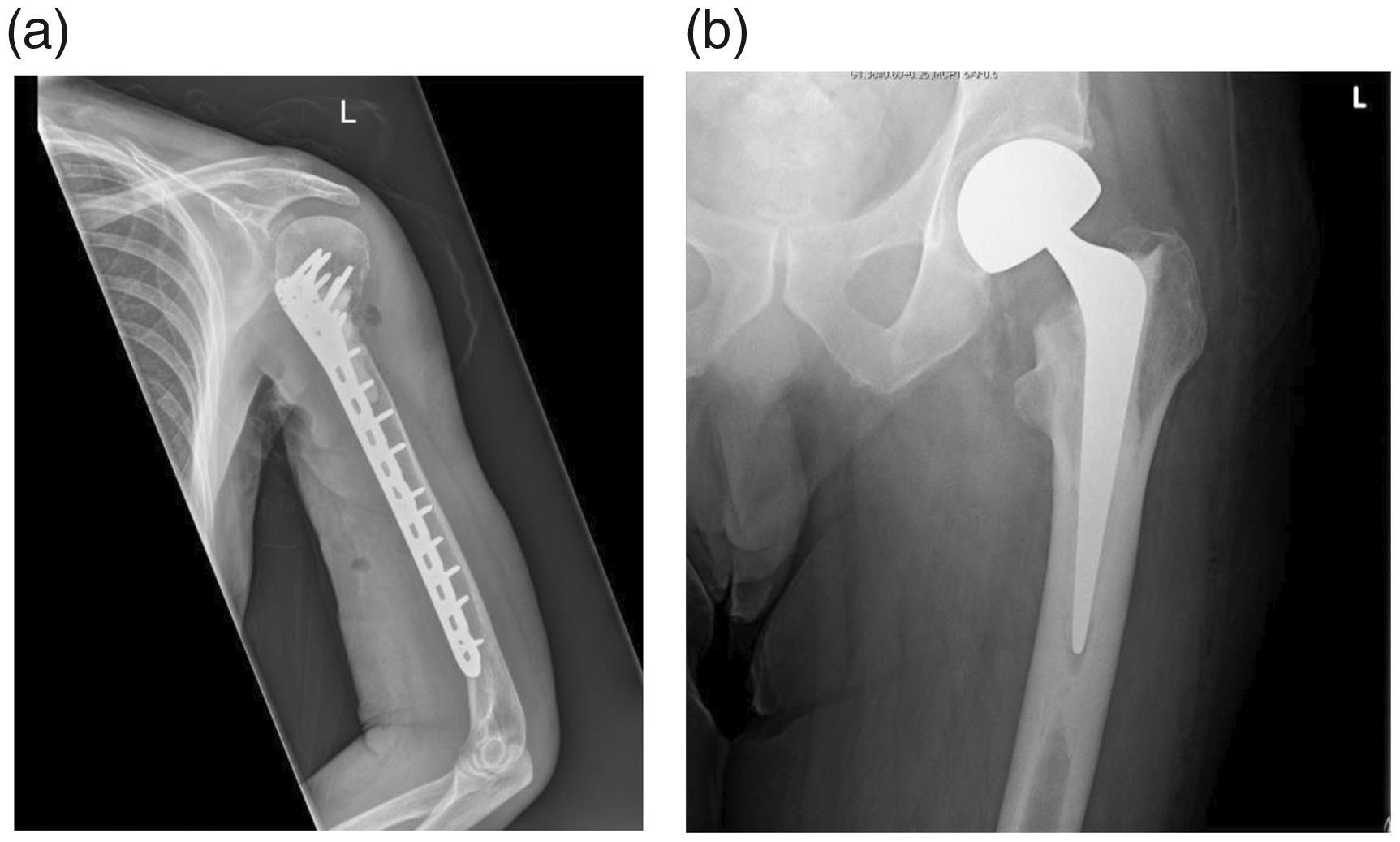
Clinical case scenario (continued).
Further investigation showed this to be disease recurrence from John’s prostate cancer with an isolated metastatic lesion at the left femoral neck. John was otherwise fit and well and 2 weeks later was able to mobilise independently with an exercise tolerance of 3-4 miles and to complete all activities of daily living without support. His case was discussed with the MDT and a decision made for surgical intervention. An excision arthroplasty was performed (Fig. 2(b)).
Care and rehabilitation in the community
Individualised rehabilitation programmes should be considered for all patients including advice on nutrition and physical exercise. Regular physical activity has been shown to improve functional health with benefits to mental health, physical health and quality of life been observed (Cormie et al., 2014). The general advice is to avoid stress on high-risk areas, or those with a known pathological fracture and target the unaffected limbs. The use of community physiotherapists, occupational therapists and dieticians can help aid recovery. It is important to consider the significant impact on patients’ mental health. Using the support from services provided by specialist cancer or palliative nurses can be invaluable for the patient.
In this case study, John had the lesion excised and a hemi-arthroplasty inserted. The rehabilitation plan from the orthopaedic team was that he could fully weight bear on this affected hip straight away. In cases where the weight bearing or exercising status of an affected limb is in question it is important to liaise with the specialist team for further clarification.
Summary
Although patients with skeletal metastases are commonly encountered, improved awareness of the disease in both primary and secondary care is needed for earlier diagnosis. Early identification of MBD improves patient outcomes. It is important to consider this diagnosis in any patient presenting with musculoskeletal pain with a previous history of malignancy. Pain is the predominant symptom, with areas such as the spine, pelvis, ribs and long bones commonly affected. Functional pain is a particular red flag and must be investigated urgently. Although MRI remains the gold standard imaging modality, other more accessible tests such as bloods and X-rays should be used to aid diagnosis.
Management should include early MDT involvement to give patients the best outcomes possible. Conservative, medical or surgical treatment options may be used depending on a number of factors, including the patient’s age, comorbidities, prognosis, cancer type and previous treatment history. Patient involvement in decision making is important when deciding on a suitable treatment plan.
Although outcomes from MBD are gradually improving, the increasing incidence of cases observed in recent years highlights the importance of improving service provision. It is likely that the creation of an MBD 2-week wait referral pathway would help with this, by improving access to specialist services and allowing earlier MDT discussions.
KEY POINTS
Early recognition of MBD improves patient outcomes Pain is the predominant symptom, with functional pain being a poor prognostic indicator Maintain a high index of clinical suspicion for patients with previous malignancy presenting with musculoskeletal pain and a low threshold for referral of patients with possible MBD on a 2-week wait referral to local secondary care services Management is individualised and requires an MDT approach Pain management is crucial to aid quality of life Planned prophylactic surgery is preferable to emergency fixation
Footnotes
ORCID iDs
Natalie Cheyne https://orcid.org/0000-0003-0436-5739 Amit Kumar ![]()