
Abstract
Myeloma is a rare, life-limiting blood cancer arising from plasma cells. Early diagnosis is imperative to improve clinical outcomes for patients, by both improving overall survival and reducing the morbidity associated with myeloma-related end-organ damage. This can be challenging in primary care, as myeloma can be difficult to diagnose. It may present in a number of non-specific ways that overlap with a multitude of other conditions. Tests that indicate myeloma are readily available in primary care. This article will describe the pathology of myeloma, the range and timing of diagnostic tests, guide interpretation of results, and outline the diagnostic subcategories of plasma cell disorders. Two cases looking at different aspects and complications of myeloma diagnosis are discussed with the aim of raising awareness and potential pitfalls in diagnosis. Useful resources to aid clinicians are signposted.
Clinical case scenario 1
A 61-year-old woman presented to her GP with a 3-month history of mid-thoracic back pain radiating to the left chest wall. It developed over a period of weeks without an obvious precipitant. It was persistent and disturbed her sleep despite regular over-the-counter analgesia. She felt unsteady mobilising and was unable to stand from a chair without pushing up with her arms. She denied bowel or bladder dysfunction and had no sensory changes. She had no constitutional symptoms. She had a past medical history of type II diabetes and hypertension. On examination she had a body mass index (BMI) of 37 kg/m2. There was no spinal tenderness and neurological examination was normal.
She had a normal full blood count, renal function and calcium. A myeloma screen was performed, which detected an IgG paraprotein at 3 g/L and normal serum free light chains, alongside low level Bence–Jones proteinuria. A magnetic resonance imaging (MRI) scan of her spine revealed no sinister bony lesions and no clear cause for her pain. A bone marrow biopsy was not performed as the paraprotein was less than 15 g/L and she had no evidence of myeloma-related end-organ damage. She was diagnosed with IgG monoclonal gammopathy of uncertain significance (MGUS) and her GP is monitoring her MGUS parameters on a 6 monthly basis.
Pathophysiology
Myeloma is a clonal proliferation of plasma cells. It constitutes approximately 18% of all haematological malignancies and 2% of all cancers (Cancer Research UK, 2016). Plasma cells are mature B-lymphocytes that produce antibodies to fight infection. Each plasma cell is capable of producing a unique antibody, or immunoglobulin, to a specific foreign antigen as part of the humoral immune response. In health, numerous immunoglobulins are produced to contend with the multiple insults that the immune system faces. In myeloma, however, mutations within a single plasma cell form the basis of a clonal population of abnormal plasma cells that become dominant within the bone marrow. These myelomatous plasma cells produce only one form of immunoglobulin, and due to the abnormalities gained, normal antibody function is frequently lost or reduced. The immunoglobulin secreted by clonal plasma cells can be detected in the blood by serum protein electrophoresis and is referred to as a ‘paraprotein’.
A normal antibody is made up of two heavy chains and two light chains (see Fig. 1). In myeloma, sometimes only part of the immunoglobulin, the light chain, can be detected in the blood and/or urine as in light chain myeloma. In some cases, the excess of light chains produced is excreted into the urine and may be detected as Bence–Jones protein. The amount of paraprotein in the blood does not always correlate with the number of plasma cells in the bone marrow. In some cases, the malignant plasma cells are high secretors, but more rarely they can be non-secretors. In these patients, myeloma can be detected in the bone marrow, but there is no measurable paraprotein or serum free light chain imbalance.
Antibody production by plasma cells.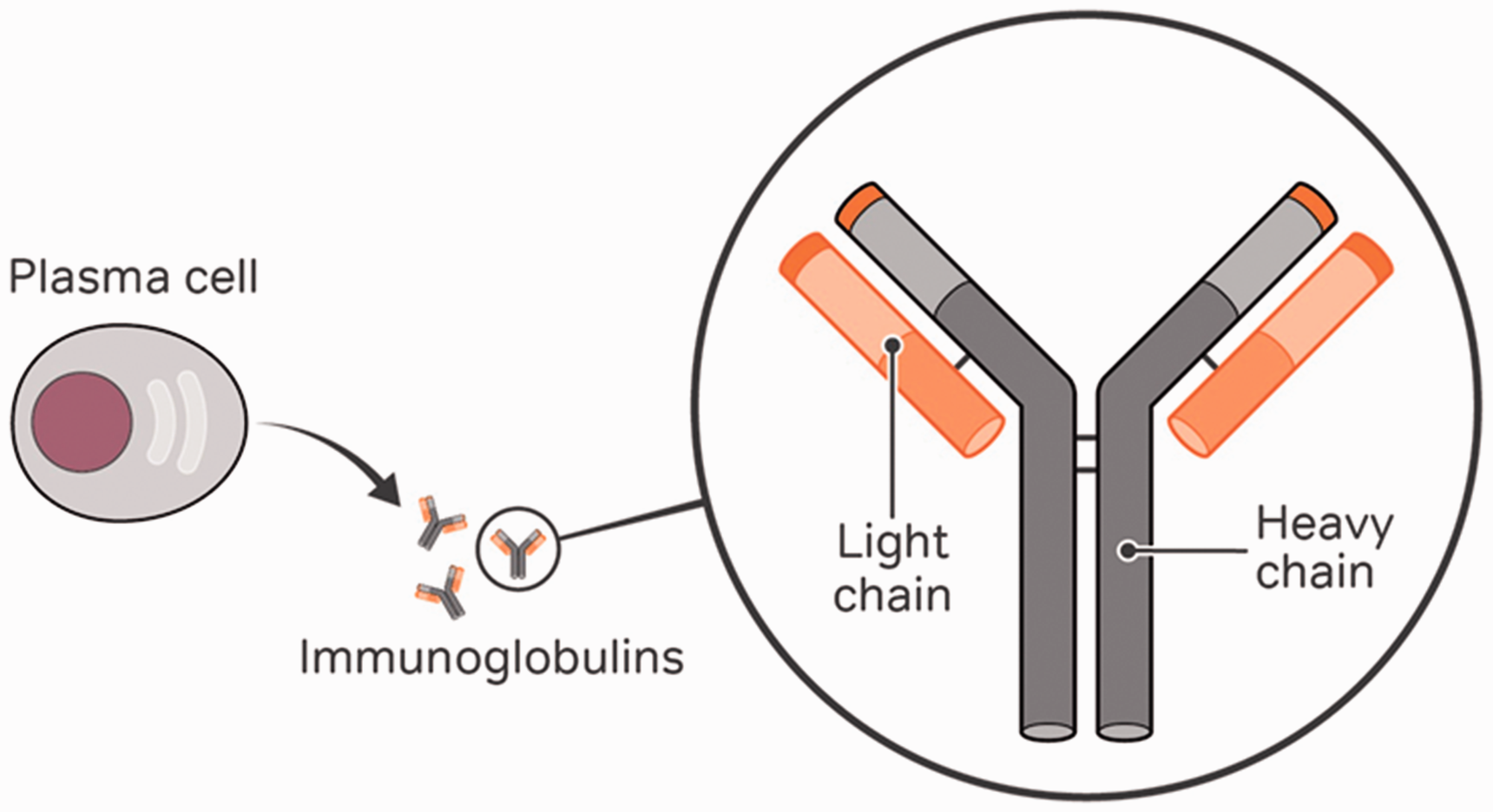
Clonal plasma cells are capable of suppressing normal bone marrow function, impairing bone homeostasis and through a number of mechanisms impacting on kidney function. This leads to the cardinal symptoms and signs of myeloma as summarised by the acronym CRAB – calcium (hypercalcaemia from bone breakdown), renal impairment, anaemia and bone pain (Rajkumar et al., 2014).
Early diagnosis is key
A diagnosis of myeloma can be difficult and is often delayed because the symptoms can be vague and non-specific with a low predictive value. For many patients, it can take months from their first presentation before a diagnosis is established (Howell et al., 2017; Koo et al., 2018). Early diagnosis is critical, in order to allow the timely institution of treatment to reduce the risk of potentially life-threatening and debilitating complications developing. These complications may include spinal cord compression, renal failure requiring dialysis and fractures. Given the majority of patients with myeloma are older than 65-years they may have less physiological reserve to withstand such events. Recent data shows that 33% of patients are diagnosed by the emergency route. The 1-year survival for patients diagnosed in the emergency setting is 62% versus 88% for patients diagnosed by primary care referral (National Cancer Registration and Analysis Service (NCRAS), 2018). Although treatment can correct some complications, not all are reversible and can be life-limiting in themselves, even when the underlying myeloma is managed.
Clinical case scenario 1 (continued)
Key points relevant to early diagnosis of myeloma in the clinical case scenario:
Myeloma should be considered in the differential of persistent back pain, as for many patients pain is the presenting symptom despite the fact that back pain is common and frequently occurs independently of a paraprotein Red flag symptoms relevant in this case include (National Institute for Health and Clinical Excellence (NICE), 2018) age greater than 50 years, gradual onset of symptoms unremitting pain, including aching night pain that disturbs sleep and thoracic pain and no symptomatic improvement after 4 to 6 weeks of conservative management NICE recommends a full blood count, calcium and either plasma viscosity or erythrocyte sedimentation rate (ESR) be performed to assess for myeloma in people over 60 years with persistent bone pain, especially back pain (NICE, 2017). Urgent serum protein electrophoresis and a serum free light chain assay should be requested. A low level of paraprotein does not always exclude myeloma as a cause of symptoms, as some patients can be oligosecretory
Who to test?
Most frequently, a paraprotein is detected incidentally during investigation of other problems. For this group, the majority of patients are found to have MGUS (Bird, 2012). Patients with MGUS have a risk of progression to myeloma of approximately 1% per year. They should therefore be routinely monitored in primary or secondary care, depending on local arrangements. One of the biggest difficulties in the diagnosis of myeloma is that symptoms can be non-specific, overlap with a number of different conditions and can seem unconnected (see Fig. 2).
Common presenting features of myeloma.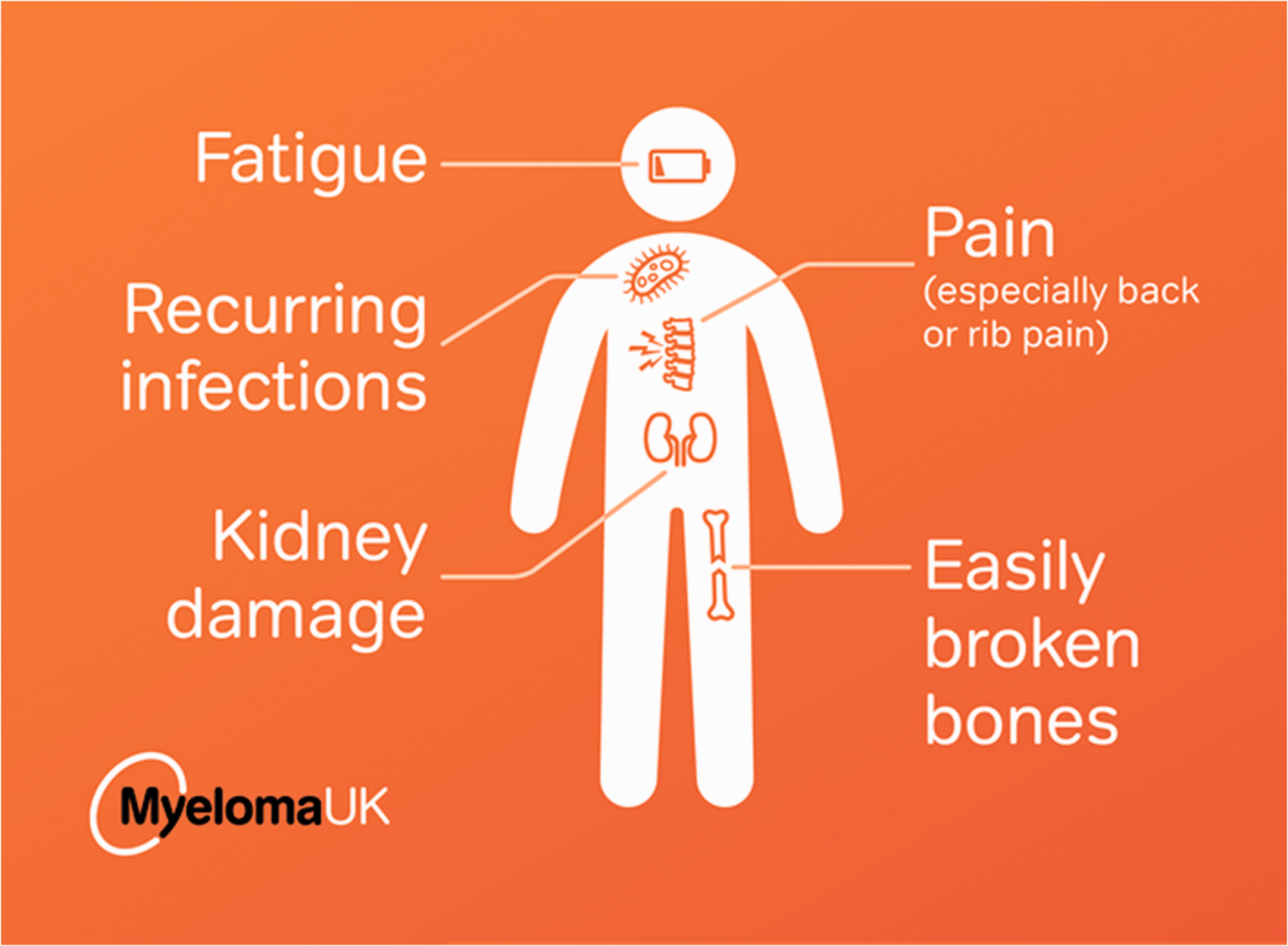
The majority of patients (60–70%) present with pain, particularly back or other bone pain, or unexplained fractures (Yong et al., 2016). Myeloma bone disease is caused by malignant plasma cells disrupting the usual balance between osteoclasts and osteoblasts by promoting osteoclast activation and bone turnover and inhibiting osteoblast function. This imbalance may be seen as lytic lesions on imaging (although these may only be visible on plain X-rays when 30–50% of trabecular bone is lost) or as diffuse osteoporosis (Barwick et al., 2019). This process can lead to hypercalcaemia and the associated symptoms of thirst, abdominal pain and confusion.
When to test for possible myeloma.

Adapted from Myeloma UK (2020)
In addition to these CRAB features, other signs and symptoms can be identified, many of which can be detected earlier than these signs of end-organ damage. Myeloma impacts on the function of the immune system in a number of ways, not all of which are fully understood. This leaves patients susceptible to recurrent infections, particularly from encapsulated bacteria such as pneumococcus. Patients may also complain of bleeding and bruising. This is due to a combination of factors including thrombocytopenia and the interaction of paraprotein with elements of the clotting pathway. A number of common co-morbidities can overlap with the signs and symptoms seen in myeloma, and teasing them apart is one of the diagnostic difficulties. For example, patients may have anaemia related to a chronic inflammatory condition, pain due to osteoarthritis and/or chronic kidney disease related to diabetes or hypertension. It can help to review if these symptoms are stable and chronic and clearly related to another cause when considering them in the context of a newly detected paraprotein. However, thought should be given to testing for myeloma in any patient with persistent, unexplained symptoms of concern, particularly back pain, as summarised in Table 1.
Which investigations should be performed in primary care?
Recommended investigations for a patient with suspected myeloma.
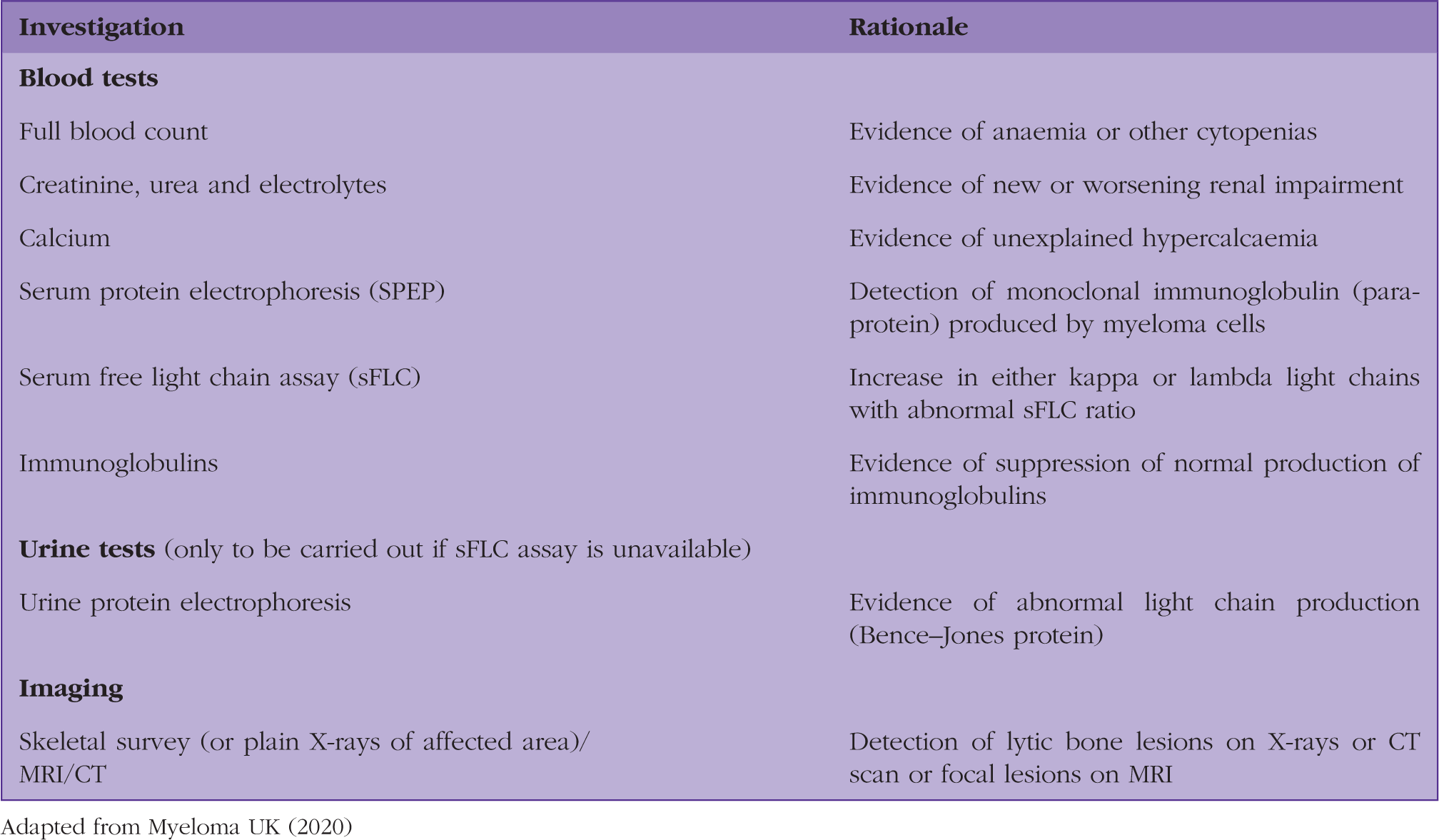
Adapted from Myeloma UK (2020)
More specialised tests such as serum protein electrophoresis and serum free light chain assay identify the presence of a paraprotein and/or clonal light chains suggestive of an underlying plasma cell disorder. These tests also allow characterisation of the type of immunoglobulin being produced and allow for quantification of paraprotein. The paraprotein result will be reported as showing an immunoglobulin type, most commonly IgG followed by IgA, and the amount present. Serum free light chains (sFLC) are present in either a kappa or lambda form, and in myeloma the balance will be skewed to one or the other, due to the monoclonal production. The results will quantify the amount of light chain present and the ratio of kappa: lambda light chains. The ratio is important, as an abnormal ratio suggests an imbalance in production, suggesting the presence of a clonal plasma cell population. It is important to note that sFLC are renally excreted. This means that when there is impaired renal function, of any cause, there can be an elevation in sFLC; however, the ratio may remain close to the normal reference range. Many laboratories have a reference range for those with concurrent renal impairment. Immunoglobulin levels are useful in determining whether normal immunoglobulin production has been preserved or whether it has been suppressed by the abnormal clone.
The choice of initial imaging will depend on the patient’s presentation and the differential diagnosis at the time of assessment. An X-ray can detect lytic lesions, but whole MRI scanning is much more sensitive (Barwick et al., 2019) and is currently recommended as the first-line imaging choice in NICE guidance (NICE, 2016).
How are the results interpreted?
The results obtained from the above investigations can help to stratify patients into different diagnostic groups, each group with its own care pathway, for example, MGUS versus suspected myeloma. Some patients can be monitored safely in the community. Others will require referral to secondary care for further review. Secondary care investigations may include bone marrow biopsy and more detailed imaging, to confirm diagnosis and guide management.
All tests need to be interpreted in the light of known patient co-morbidities. For example, stable anaemia related to another known cause alongside the finding of a new paraprotein does not necessarily indicate a myeloma-related complication; the same may apply to stable chronic renal impairment in a patient with diabetes, for example. These signs are most relevant when they are unexplained or there is a new deterioration from a stable baseline.
Interpretation of results.

Adapted from Myeloma UK (2020).
Summary of possible diagnoses of newly detected paraprotein based on the diagnostic criteria of the International Myeloma Working Group (Rajkumar et al., 2014).

Clinical case scenario 2
Clinical case scenario 2: Summary of blood results.

On further enquiry he reported a recent history of reduced appetite and intermittent abdominal pain. He had no change in his bowel habit. He was referred to haematology urgently in view of the paraprotein and new anaemia. A CT scan of his abdomen and pelvis was also arranged and he was prescribed oral iron supplementation. When seen in the haematology clinic, the anaemia had improved with 10 days oral iron replacement from 103 g/L to 116 g/L. He went on to have a bone marrow biopsy, as he had a borderline high-risk paraprotein, which demonstrated plasma cells at a level of 8% (not diagnostic for myeloma). He was subsequently diagnosed with a gastric malignancy, but will remain under monitoring for MGUS. This case highlights the incidental finding of MGUS in the context of a new anaemia due to another malignancy.
Supporting myeloma patients in the community
Patients face the emotional burden of living with a chronic, life-limiting illness with no definitive cure. They may endure relapses and are vulnerable to the side effects of the medication prescribed. They will also be recommended to have an annual influenza vaccination and a pneumococcal vaccination every 5 years. For those with MGUS, there may be anxiety related to the uncertainty of progression to myeloma.
Consultants and clinical nurse specialists are available to offer advice, support and guidance for GPs and patients alike. Myeloma UK has a multitude of resources and can provide a wealth of support, accessed via myeloma.org.uk (patients) or academy.myeloma.org.uk (for healthcare professionals). This includes a GP diagnostic tool (https://academy.myeloma.org.uk/resources/gp-myeloma-investigation-tool/) produced in partnership with experts from the Myeloma UK Early Diagnosis Steering Committee. Any queries or follow-up guidance for GPs should be directed to earlydiagnosis@myeloma.org.uk.
KEY POINTS
Early diagnosis is important in preventing myeloma-associated morbidity and prolonging survival The key signs and symptoms are summarised by the acronym CRAB – hypercalcaemia, renal failure, anaemia and bone pain (particularly back pain) Fatigue, recurrent infections and bleeding and bruising can also be features that should raise suspicion Consider performing a myeloma screen in any patient with persistent, unexplained symptoms as outlined above Refer to the Myeloma UK GP diagnostic tool if myeloma is suspected to ensure relevant investigations are ordered If IgG paraprotein greater than 15 g/L, IgA or IgM greater than 10 g/L or less than 15 g/l with otherwise unexplained symptoms in keeping with myeloma or abnormal sFLC ratio refer for urgent haematology review