
Abstract
Alcohol misuse is a common cause of pancreatitis, both acute and chronic. Alcoholic pancreatitis can present a significant diagnostic challenge for GPs, and a high index of suspicion must be maintained to avoid delayed or missed diagnoses. Management is multi-faceted and an enduring relationship between patient and GP ensures the best patient outcomes. This article will discuss both acute and chronic alcoholic pancreatitis, the diagnosis of alcohol-induced pancreatitis in its different forms and how to create a management plan that addresses symptom control as well as improving long term patient outcomes.
Clinical case scenario
Simon is a 41-year-old man who presents with chronic intermittent epigastric pain radiating to his back, often excruciating in severity. When asked about his bowel habit he describes a 3-month history of pale offensive stools that are difficult to flush away. He has noticed weight loss over the last 6 months. His medical records show that he has been alcohol-dependent for many years, and he tells you he is still drinking heavily. What differential diagnoses would you consider in this man? What would be the next steps in his management?
Acute alcoholic pancreatitis
Scale of problem
Alcohol is the second most common cause of acute pancreatitis after gallstones. Approximately 50% of acute pancreatitis in the UK results from gallstones, 25% from alcohol, and 25% from other causes such as autoimmune inflammation, tumours of the pancreas or post-endoscopic retrograde cholangiopacreaticography (National Institute for Health and Care Excellence (NICE), 2018). In the UK, the incidence of acute alcoholic pancreatitis is approximately 14 per 100 000 per year (NICE, 2018). Up to 3% of heavy drinkers will eventually develop acute pancreatitis versus 1% of non-drinkers (Herreros-Villanueva et al., 2012).
Pathophysiology
Whereas the occurrence of acute pancreatitis due to alcohol has been recognised for over 100 years, the mechanisms by which this occurs are not fully understood. Although commonly associated with pancreatitis, it seems that alcohol in isolation does not cause inflammation, as evidenced by the rather small number of individuals who develop acute pancreatitis after prolonged periods of alcohol abuse. Alcohol appears to predispose the pancreas to damage from other insults, including smoking, high-lipid diets and infectious agents. Genetic factors also play a role (Clemens et al., 2016).
Damage appears to originate in the acinar cells that secrete pancreatic digestive enzymes including trypsin, where metabolism of alcohol generates toxic products that promote intracellular calcium release and thus activation of trypsinogen to trypsin. Activation of stellate cells, which are responsible for maintaining the extracellular matrix, transforms them into myelofibroblasts, which in turn promote inflammation and fibrosis of the gland. Cytokine release may cause a systemic inflammatory response (Clemens et al., 2016).
Signs and symptoms
Acute pancreatitis typically presents with upper abdominal pain, which may be sudden in onset, severe, and radiate to the back. Nausea and vomiting occur in 80% of patients (BMJ Best Practice, 2020).
Signs on examination may include fever, epigastric tenderness and guarding, and uncommonly Grey Turner’s and Cullen’s signs: bruising to the flanks and around the umbilicus respectively. More severe pancreatitis may be associated with a systemic inflammatory response characterised by tachycardia, tachypnoea, reduced oxygen saturations and hypotension. It is important to consider and exclude other causes of an acute abdomen, such as ruptured abdominal aortic aneurysm, perforated or obstructed viscus, cholecystitis or ischaemic bowel.
Investigations in secondary care
Patients with acute severe abdominal pain will often present to the emergency department. Patients presenting to their GP with acute severe abdominal pain should be referred to hospital for same-day assessment.
According to the Revised Atlanta Classification (Banks et al., 2012) diagnosis of acute pancreatitis requires two out of three of the following:
Pain typical of pancreatitis Serum amylase or lipase activity greater than three times the upper limit of normal Characteristic findings of acute pancreatitis on imaging
Serum lipase measurement is preferred over amylase where available, due to its higher sensitivity and specificity (UK Working Party on Acute Pancreatitis, 2005).
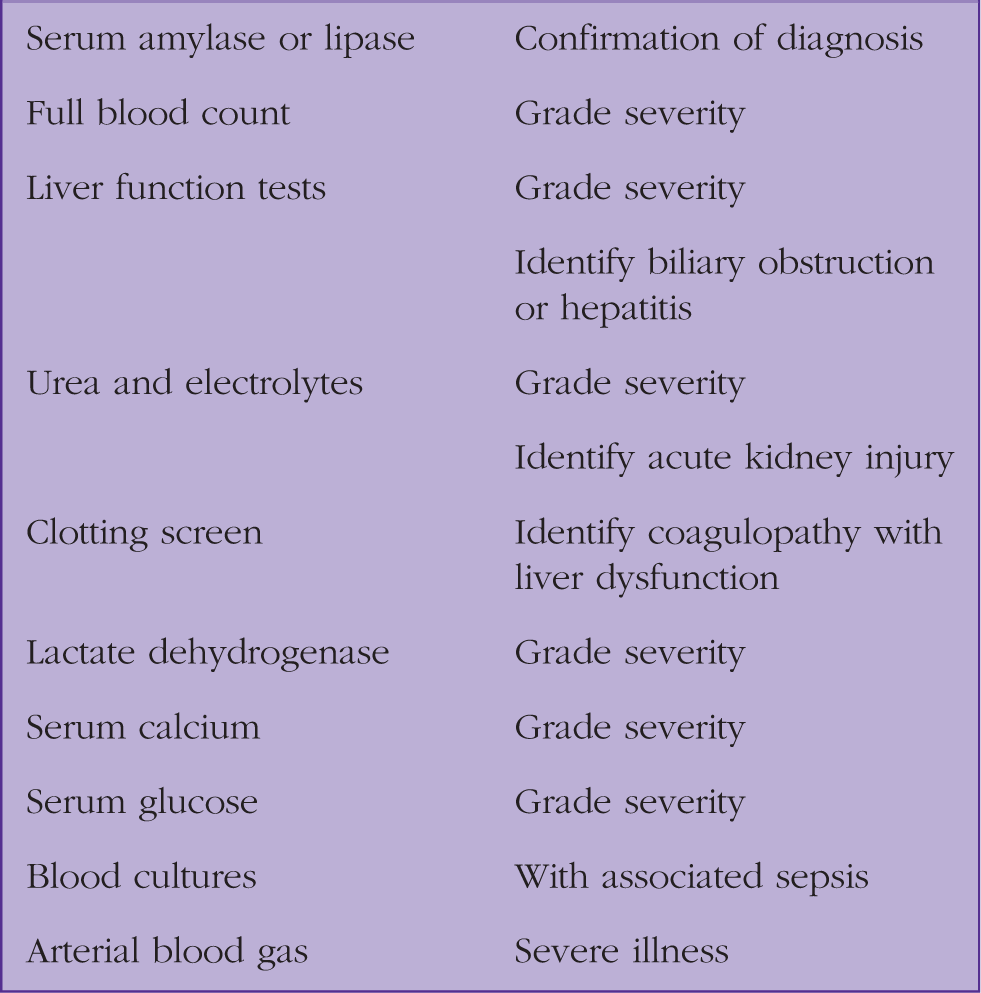
Laboratory investigations in acute pancreatitis in secondary care.
Ultrasound imaging is sensitive for gallstone disease and biliary pathology, and should ideally be performed within 24 hours of admission. Contrast-enhanced computerised tomography (CT) is useful where the diagnosis is not biochemically proven, or there is failure to improve after 48–72 hours of treatment, or complications are suspected.
A number of scoring systems exist and combine clinical, biochemical and radiological findings to grade severity. They include the Glasgow-Imrie, Atlanta and Ranson criteria.
Management
Although no specific therapy exists for acute pancreatitis, patients should be admitted to hospital for supportive treatment. Analgesia, potentially in the form of intravenous patient-controlled opioid infusion, and antiemetics should be prescribed.
Although traditionally this group of patients was kept nil by mouth, it is now understood that enteral nutrition has prognostic benefit and should therefore be re-established as soon as possible. Post-pyloric feeding via nasal tube may be considered in gastric stasis and severe vomiting. Parenteral nutrition should be reserved for failure of the enteral route (Van Dijk et al, 2017).
Patients are likely to be fluid-deplete, due to poor oral intake, vomiting and fluid sequestration in the bowel and around the pancreas, so appropriate intravenous fluid should be prescribed with care, to replace electrolytes such as magnesium and calcium. Prophylactic antibiotics do not prevent infection, so should not be prescribed routinely (Van Dijk et al., 2017).
Patients with alcohol excess are likely to be deficient of thiamine and other B vitamins and should receive appropriate replacement with a high potency parental solution. Alcohol withdrawal should be prevented using benzodiazepines, prescribed according to an assessment score such as the Clinical Institute Withdrawal Assessment for Alcohol – Alcohol, revised (CIWA-Ar) scale. Referral to alcohol treatment services should be made, either as an inpatient or at discharge.
Complications of pancreatitis, such as biliary obstruction, pseudocyst formation, infection and necrosis, may necessitate endoscopic, radiological or surgical intervention, and these patients should be managed in a tertiary centre by a multi-disciplinary team. Secondary organ failure, such as acute respiratory failure or acute kidney injury, may necessitate admission to intensive care and invasive organ support.
Prognosis
Acute alcoholic pancreatitis carries a 3% mortality rate at 60 days (Roberts et al., 2014). Repeated episodes may lead to chronic alcoholic pancreatitis.
Chronic alcoholic pancreatitis
Chronic pancreatitis is defined as ‘a chronic, irreversible, inflammation and/or fibrosis of the pancreas, often characterized by severe pain and progressive endocrine and exocrine insufficiency’ (NICE, 2016). It is difficult to accurately estimate the occurrence of chronic pancreatitis due to alcohol, as patients with alcohol misuse and dependence may avoid healthcare or be lost to follow up, and diagnosis is often challenging in those that do present. A French study estimated an annual incidence of 7.7 cases per 100 000 (Lévy et al., 2006), but there are currently no reliable data on UK incidence and prevalence. Alcohol causes 70–80% of cases of chronic pancreatitis (NICE, 2018).
Pathophysiology
The pathophysiology of chronic alcoholic pancreatitis is poorly understood, but it is thought that the disease process can be divided into three phases that can overlap or occur out of sequence. In the early phase of the disease, there are repeated episodes of acute pancreatitis. In the middle phase, these repeated insults lead to loss of pancreatic parenchyma and morphological changes in the gland including fibrosis and calcifications (Lévy et al., 2014). Disruption of pancreatic ducts and extravasation of pancreatic secretions can lead to formation of pseudocysts adjacent to the pancreas; although pseudocysts may occur with acute pancreatitis or pancreatitis caused by other aetiologies, they are more common in chronic pancreatitis and when pancreatitis is alcohol-induced (Habashi and Draganov, 2009). Eventually, in the late phase, loss of gland function becomes the predominant issue. Exocrine dysfunction, due to damage to acinar and ductal cells, leads to malabsorption. Damage to Islets of Langerhans may lead to reduced insulin secretion and pancreaticogenic diabetes.
Signs and symptoms
Patients typically present with chronic upper abdominal pain, similar in character to that caused by acute pancreatitis, though pain may be absent. Nausea and vomiting are common. Diarrhoea, steatorrhoea and excessive flatus may result from malabsorption, due to reduction of excretion of digestive enzymes. Malabsorption, in turn, can lead to weight loss, which is often compounded by poor diet in patients with alcohol excess. Destruction of the endocrine pancreatitis may result in diabetes mellitus and associated clinical features.
There are often few clinical signs on examination except abdominal tenderness. Doctors should assess the patient for signs of liver disease, as this may be an opportunity in patients with chronic alcohol abuse to detect a concomitant problem.
Investigation in primary care
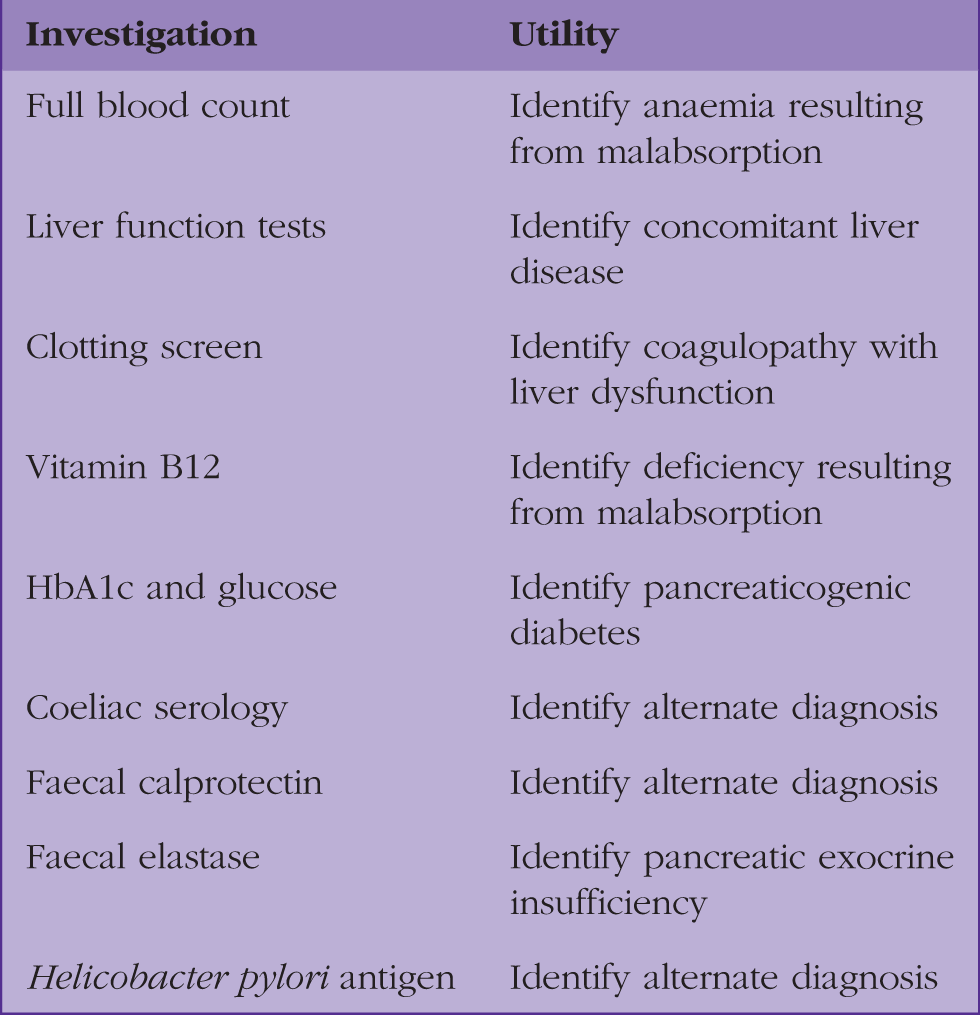
Laboratory investigations in chronic pancreatitis.

Although ultrasound imaging of the abdomen may be useful to identify gallstones and review pancreatic morphology, NICE advises CT ‘as the first-line imaging modality for the diagnosis of chronic alcohol-related pancreatitis in people with a history and symptoms suggestive of chronic alcohol-related pancreatitis’ (NICE, 2017).
Further investigations to facilitate a diagnosis that may be performed in secondary care include:
Secretin enhanced magnetic resonance imaging Magnetic resonance cholangiopancreaticography Endoscopic ultrasound
Management
Complications of chronic pancreatitis.
Since there is potential overlap between the typical presenting symptoms of chronic alcoholic pancreatitis and those of a potential cancer, for example, weight loss with abdominal pain, many patients will also meet the criteria for referral under the suspected cancer pathway. In some cases, patients can meet the criteria for two or more suspected cancer pathways, thus, clinical judgement will be required in deciding how best to manage the patient.
Management often begins in secondary care and is continued in primary care. GPs have a pivotal role in holistic management and long term follow up of patients with chronic pancreatitis. A multi-disciplinary approach is usually required for patients, and guidance from various secondary care teams may be needed depending on the features of the individual’s disease.
Alcohol use should be discussed. Reduction in alcohol intake, ideally abstinence, is an important management step for chronic pancreatitis, as continued excessive use is associated with worse outcomes. Referral to a specialist alcohol treatment unit for assisted withdrawal from alcohol should be considered. Patients should be offered oral thiamine if they are at risk of malabsorption. Smoking is an independent risk factor for chronic pancreatitis (Gupte et al., 2018), and so patients should also be counselled on smoking cessation.
Depression can often co-exist with alcohol dependence. A scoring system such as PHQ-9 can be helpful in diagnosing and assessing the severity of depression in patients.
Analgesia should be titrated based on the World Health Organisation’s ladder. Pain can be difficult to treat, and there is a risk of opioid dependency, so referral to a pain management team may be required. Pain that is worsening or disproportionate can indicate a complication such as bile duct or duodenal obstruction or pseudocyst formation. For intractable pain, techniques such as coeliac plexus blocks or surgery such as pancreaticoduodenectomy may be considered.
Patients with exocrine dysfunction should trial pancreatic enzyme supplementation with pancreatin, which is taken with food. A low fat, high calorie diet with high protein intake can be beneficial. Fat soluble vitamins (A, D, E and K) may need to be supplemented. A referral to a dietician may be helpful. Patients with chronic pancreatitis and malabsorption should be offered an annual dual energy X-ray absorptiometry scan to screen for osteoporosis.
Management of pancreaticogenic diabetes can be challenging. Diabetes in patients with chronic pancreatitis can be especially brittle, due to poor diet and malabsorption. Oral agents are often insufficient to control sugars, and insulin may be needed. A secondary care endocrine opinion may be beneficial for the patient if blood sugar control is poor. Those patients without known diabetes should have an annual HbA1c to screen for its presence.
Prognosis
Patients with chronic alcoholic pancreatitis have been found to have a reduced life expectancy compared with age-matched controls in various studies, but it has been noted that death in most patients results from extra-pancreatic consequences of smoking and alcohol, such as ischaemic heart disease or malignancy, rather than the pancreatitis itself (Lévy et al., 2014).
Notwithstanding this reduced life expectancy, patients with chronic alcoholic pancreatitis may have significant and disabling morbidity, due to severe pain and complications of pancreatic endocrine and exocrine dysfunction. Since chronic pancreatitis is irreversible, clinicians should focus on halting disease progression and managing symptoms, in order to provide their patients with the possible best quality of life.
KEY POINTS
Alcohol is the second most common cause of acute pancreatitis, and the most common cause of chronic pancreatitis Patients with suspected acute alcoholic pancreatitis should be admitted to hospital for investigation, diagnosis and supportive treatment If chronic alcoholic pancreatitis is suspected referral to Gastroenterology is required to confirm the diagnosis Patients with chronic pancreatitis have reduced life expectancy and morbidity from chronic pain, malabsorption and pancreaticogenic diabetes Chronic pancreatitis is irreversible, and management should focus on alcohol reduction to slow disease progression, and treatment of complications GPs have a pivotal role in holistic management and long term follow up of patients with chronic pancreatitis using a multi-disciplinary approach with various secondary care teams based on features of the individual’s disease