
Abstract
Salivary gland tumours are uncommon and account for just 6% of all head and neck neoplasms. Worldwide incidence varies, from 0.4 to 13.5 cases per 100 000 population. The parotid gland is by far the most commonly affected site, accounting for 80% of cases. The vast majority of these tumours are benign; only approximately 20–25% being malignant. This article considers the relevant clinical anatomy of the parotid gland, key aspects of assessment with history and examination, and when to refer to secondary care for further investigation. It will touch on the common benign and malignant parotid neoplasms and give an overview of secondary care management.
Clinical case scenario
A 71-year-old male patient presents in a routine appointment with some swelling to the left side of his neck. He thinks it may have been there for some time, but is unsure exactly how long. He thinks it may be very slowly getting larger. It does not cause him any discomfort, but he is starting to worry and thought he should see a doctor. The patient’s co-morbidities include hypertension and type 2 diabetes for which he takes metformin. He smokes approximately 15 cigarettes a day and has done so for 30 years. On examination you find a non-tender, nodular mass just inferior to his left ear. This appears to be unilateral, there are no overlying skin changes and there is no associated cervical lymphadenopathy:
What would be your differential diagnosis? What type of parotid tumour are you suspicious of in this patient? How would you manage this patient in primary care?
Clinical anatomy
The parotid glands are the largest of the three paired salivary glands and can be palpated on the lateral surface of each cheek, anterior and inferior to the ear, see Fig. 1. The gland is bordered superiorly by the zygomatic arch, anteriorly and medially by the masseter muscle and posteriorly by the sternocleidomastoid muscle. The tail of the gland sits inferior to the lobe of the ear just posterior to the angle of the mandible (Chason and Downs, 2020).
Anatomy of the parotid gland.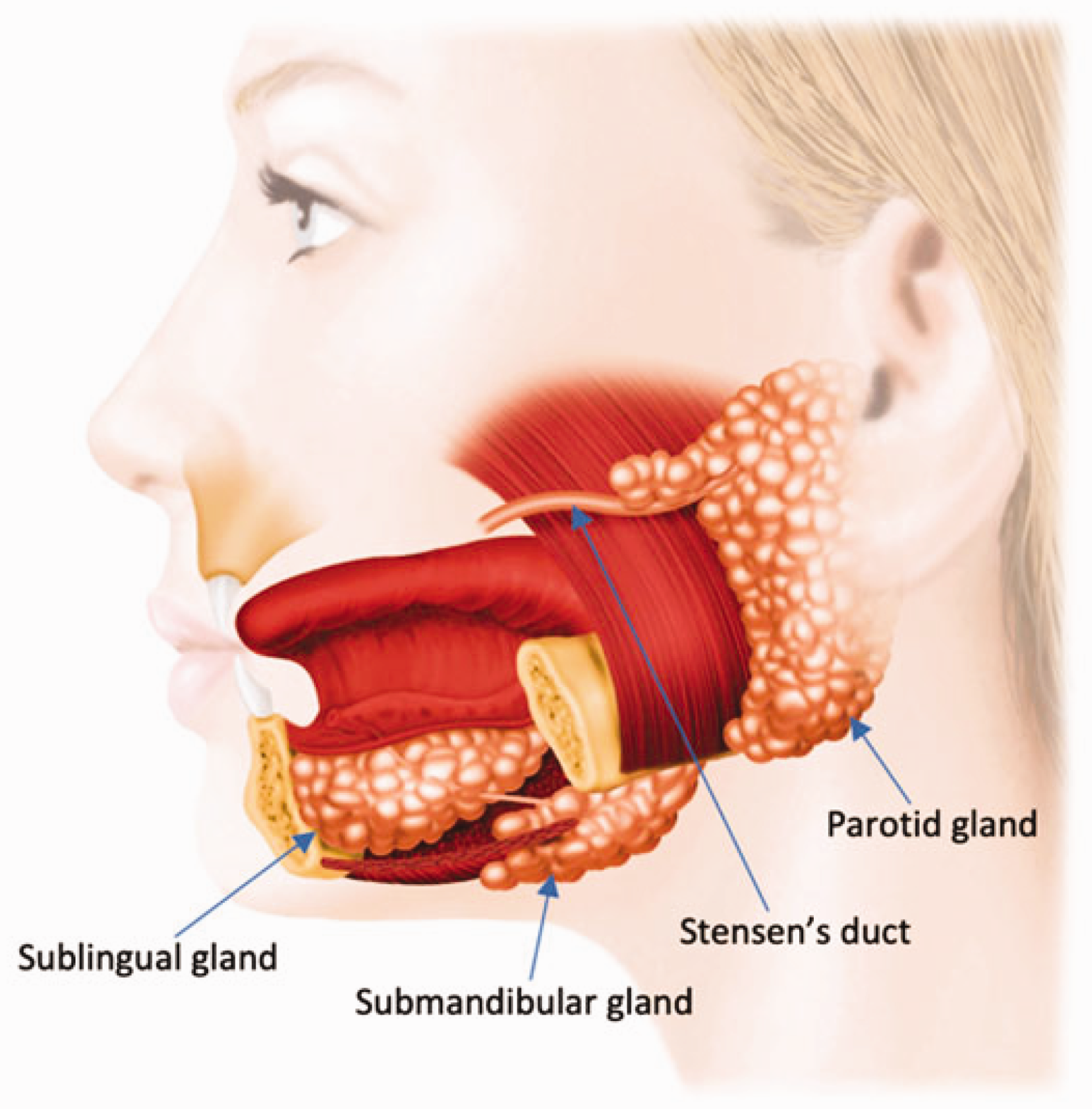
Each parotid gland is divided into a superficial and deep lobe by the facial nerve and the posterior facial vein. At a histological level, the tissue is organised into secretory units with serous acinar cells surrounded by contractile myoepithelial cells (Zhan et al., 2016). Saliva flows from these units into the intercalated ducts and then the striated ducts, lined by cuboidal epithelium and simple columnar epithelium respectively (Lewis et al., 2016). From there secretions move into the main excretory ducts before passing along Stensen’s duct into the oral cavity lateral to the second maxillary molar.
History
Differential diagnosis of a parotid lesion.
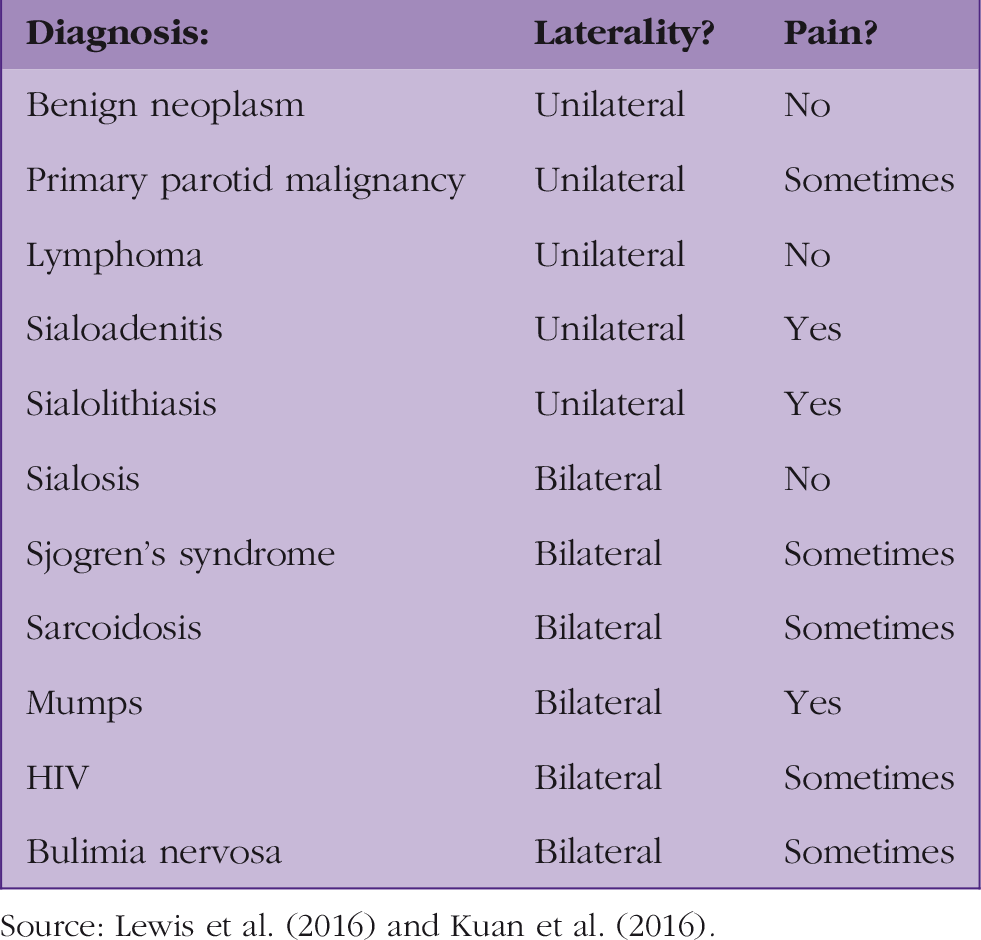
Source: Lewis et al. (2016) and Kuan et al. (2016).
After determining laterality of the mass, it is important to enquire for how long it has been present, whether it developed rapidly or gradually, and whether there have been any changes over time. Benign parotid tumours typically present with a painless, slow-growing, pre-auricular or upper-neck swelling. It should, however, be noted that up to 50% actually lack any symptoms and present as so called ‘incidentalomas’, found when a patient has head or neck imaging for an unrelated indication (Lewis et al., 2016). In contrast, rapid growth of a mass may indicate a primary malignancy or malignant transformation of a pre-existing benign lump.
Within the history the differential diagnosis for parotid gland swelling should be kept in mind. Although a malignant mass may also be tender, sudden painful swelling of the parotid often suggests obstruction, inflammation or infection. Intermittent swelling that occurs with eating or drinking may imply parotid duct obstruction, due to a calculus. The presence of symptoms, such as xerostomia and xerophthalmia may indicate Sjogren’s syndrome, whereas bilateral swelling suggests a metabolic or viral aetiology (Kuan et al., 2016).
The clinician should enquire about any relevant past medical history, such as diabetes, liver cirrhosis, kidney failure and bulimia, and also any past surgeries involving the face, neck and ears, or previous head and neck radiation therapy. A social history to determine smoking status and any history of chronic excess alcohol intake should also be taken.
The history should also include a review for possible red flags such as facial nerve weakness and weight loss. If the patient is found to have facial nerve weakness, the time course must be ascertained. A gradual decline in facial nerve function would raise the suspicion of underlying malignancy (Kuan et al., 2016).
Examination
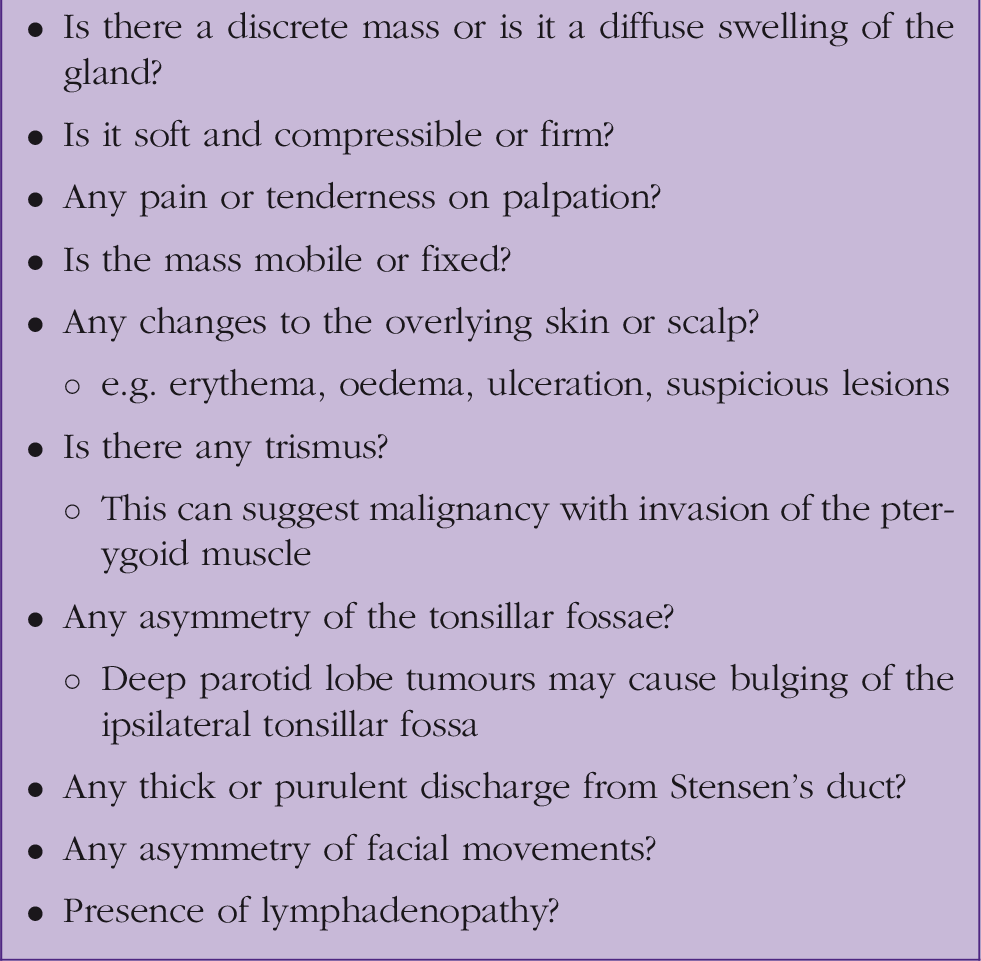
Features to consider on examination.
Referrals
Any patient with a swelling in the parotid gland persistent for greater than 3 weeks, or an unexplained lump in the neck of recent onset or that has changed over a period of 3–6 weeks, should be referred for urgent specialist review by Otolaryngology on a suspected cancer referral pathway.
Investigation
Cytology
From clinic, generally the first line investigation for a parotid gland lesion is fine needle aspiration cytology (FNAC) performed with or without ultrasound guidance. FNAC has shown a sensitivity level in the range of 40–100%, a specificity level in the range of 67–100%, and an inadequacy rate of around 8% (Schmidt et al., 2011). An alternative is to perform core needle biopsy. This technique allows a larger sample size to be taken for assessment for capsular invasion and diagnosis of lymphoma. A meta-analysis looking at this technique in the investigation of all types of salivary gland lesions found specificity to be 100% and sensitivity to be 92%, with an inadequacy rate of 1.2% (Schmidt et al., 2011). However, core need biopsy is more painful for the patient, causes more anxiety (due to the larger needle), has higher rates of bleeding and haematoma, and is thought to have a potential greater risk of tumour seeding.
Radiology
Ultrasound imaging is typically used as the first line radiological investigation and, as mentioned, it may be performed at the same time as FNAC. It is reported to be able to allow differentiation between benign and malignant salivary gland lesions in up to 80% of cases (Lee et al., 2008). If malignancy is confirmed or there is high suspicion, further cross-sectional imaging in the form of a magnetic resonance imaging (MRI) scan is needed to assess the deep lobe of the parotid gland and identify any regional or distance metastases, see Fig. 2 (Eveson and Cawson, 1985).
Magnetic resonance imaging of a large tumour in the superficial lobe of the left parotid gland (arrows).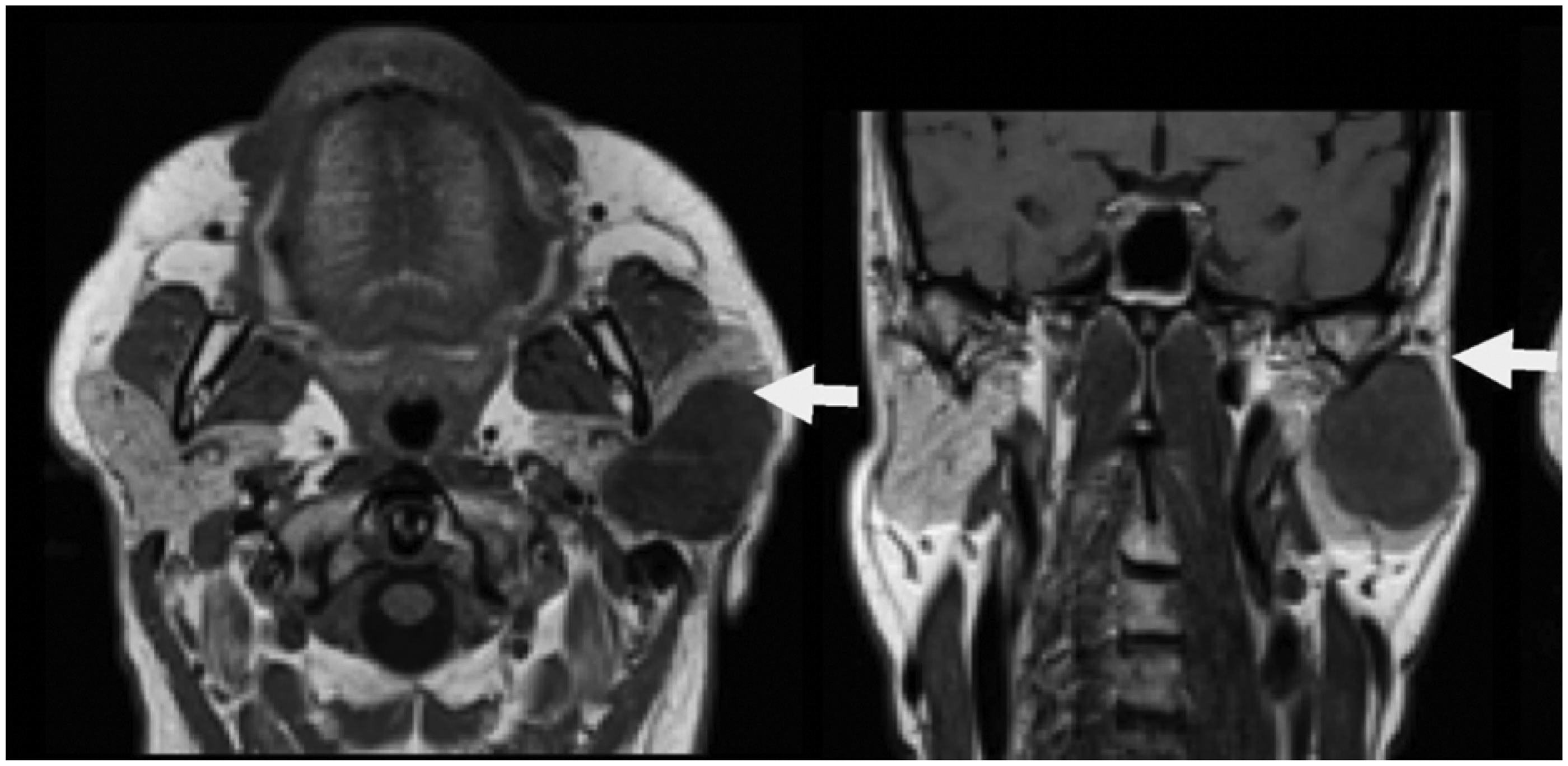
Benign parotid tumours
Benign tumours of the parotid gland.
Pleomorphic adenoma
This is the most common benign parotid tumour (approximately 60%), with 80% found in the superficial lobe and parotid gland tail (Ichihara et al., 2014). They are derived from both epithelial and myoepithelial cells that have undergone mesenchymal metaplasia, on a stromal background that can be mucoid, mixoid, cartilaginous or hyaline (Chason and Downs, 2020). These tumours present most often in women and middle-aged individuals as a slow growing, firm, unilateral, asymptomatic mass (Pinkston and Cole, 1999). When found in the parotid tail, the patient may present with eversion of the ear lobe. Malignant transformation has been reported to occur in 3–15%, with the risk increasing over time.
Warthin’s tumour
Warthin’s tumour, also known as a papillary cystadenoma lymphomatosum, is the second most common benign parotid tumour and accounts for 25–30% of cases (Eveson and Cawson, 1986). Histologically, these tumours contain epithelium that is arranged into cystic and papillary structures with surrounding lymphocytes. They most commonly present as a unilateral slow growing, painless, nodular mass in the tail of the parotid gland, see Fig. 3. Patients are generally male (2:1 predominance) with a peak incidence in the seventh decade of life. Smoking is estimated to increase the risk by 4 to 8-fold, and tumours are bilateral in 10% of cases (Eveson and Cawson, 1986). Malignant transformation is very rare, being reported as 1% (Yoo et al., 1994).
A Warthin’s tumour in the tail of the right parotid gland.
Malignant parotid tumours
The World Health Organisation lists 28 separate entities in their histological classification of salivary gland tumours of the parotid gland (Barnes et al., 2005). The three most common and clinically relevant are mucoepidermoid carcinoma, adenoid cystic carcinoma and acinic cell carcinoma. Each of these will be discussed in more detail. Primary and metastatic squamous cell carcinoma and lymphoma of the parotid gland will also be considered.
Mucoepidermoid carcinoma
Mucoepidermoid carcinoma is the most common type of salivary gland cancer, more than 90% of them occur in the parotid gland, and they account for approximately 30% of malignant parotid tumours (Eveson and Cawson, 1985). Male and females are affected equally, with the highest incidence found in the third to fifth decades of life. Mucoepidermoid carcinoma is composed of mucous-secreting cells, intermediate cells, and epidermoid squamous cells. They are classified as high-grade, intermediate, or low-grade depending on the ratio of epidermoid cells to mucous cells. High-grade tumours are associated with male sex, older age, larger size and local spread, and higher rates of nodal and distant metastasis (Eveson and Cawson, 1985). Prognosis depends on the grade of the tumour, but overall it is generally favourable with a reported 5-year survival rate of 79% (McHugh et al., 2012).
Adenoid cystic carcinoma
As the second most common malignancy of the parotid gland, adenoid cystic carcinoma typically occurs in the fourth to sixth decades of life and has a slight predisposition for the female sex (Eveson and Cawson, 1985). The tumours are composed of myoepithelial cells and epithelial luminal cells that grow with a gland-like cystic architecture. Although they tend to behave in an indolent manner with a course drawn out over 10 to 15 years, there can frequently be perineural and bone invasion, and they present with pain and facial nerve dysfunction more often than other types of parotid malignancy (Ellington et al., 2012). Although spread to regional nodes is rare, late recurrence with distant metastasis to the lungs or bones is common and can occur many years after the initial treatment. This is an important feature for GPs to consider when caring for patients diagnosed with this parotid malignancy. The 5-year survival is reported to be approximately 85% in those without distant metastasis at presentation, but falls to approximately 40% at 15 years (Guntinas-Lichius et al., 2015).
Acinic cell carcinoma
Acinic cell carcinoma is a low-grade malignancy that accounts for 10–15% of parotid tumours. It can occur at any age, tending to have a mean age of occurrence that is younger than the other parotid malignancies (Eveson and Cawson, 1985). This type of parotid malignancy was previously thought to be benign, however, late recurrences and metastases led to its re-classification. The tumour itself is made up of serous acinar cells. Although it is commonly indolent in nature, it can have a high incidence of recurrence, with studies suggesting this occurs in up to one-third of patients (Guntinas-Lichius et al., 2015).
Squamous cell carcinoma
Primary squamous cell carcinoma (SCC) is the least common primary malignancy occurring in the parotid gland, with a reported incidence of just 2–3% (Flynn et al., 1999). It is believed to arise due to chronic inflammation leading to metaplasia of the ductal epithelium. Although rare, the tumours are frequently aggressive in nature, with high rates of perineural invasion, regional lymph node metastasis, and a 5-year survival rate of <50% (Sterman et al., 1990). SSCs may also present within the parotid gland as a metastasis from a cutaneous SCC of the head and neck. The parotid gland has a dense lymphatic network that drains the temple and cheek areas of the face. While in its cutaneous phase, SCC metastasizes to regional lymph nodes in approximately just 5% of patients (Yilmaz et al., 2012), if a tumour in this region does metastasize, it is likely to be to the parotid region and then subsequently the upper cervical lymph nodes. Of particular interest to the primary care clinician, it should be noted that the majority of patients with metastatic parotid disease present sometime after the primary cutaneous SCC has been treated. Typically, this is up to 12 months after treatment, but has been reported to be as long as 2 to 3 years (Lee et al., 2017). Prognosis for patients with metastatic cutaneous SCC is generally poor, with an overall 5-year survival rate of 34% (Rowe et al., 1992).
Lymphoma
After the gastrointestinal tract, the head and neck region is the second most frequent site for extra-nodal non-Hodgkin lymphoma. Approximately 12% of these occur in the salivary glands, and although the parotid glands are by far the most common site, parotid lymphoma is still rare and accounts for just 1–4% of patients presenting with a parotid tumour (Jamal, 2018). Patients will generally present in the sixth decade of life and typically present with a painless mass that enlarges over a period of 4 to 6 months. Parotid lymphomas are usually low grade, with mucosa-associated lymphoid tissue being the most common. They carry a good prognosis, with an overall 5-year survival rate of 75% (Feinstein et al., 2013).
Management
Surgery is the mainstay of treatment for both benign and malignant parotid gland tumours. Due to the risk of malignant transformation increasing with time, it is recommended that pleomorphic adenomas and Warthin tumours are resected at the time of diagnosis (Phillips et al., 1995). This can be as an extracapsular dissection, superficial parotidectomy, or total parotidectomy, with the chosen approach dependent on the location and size of the mass and the experience of the surgeon. The extent of parotidectomy in the case of parotid malignancy is still a matter of debate. Total parotidectomy is the most frequently used approach for resection; however, some surgeons will perform a superficial parotidectomy for superficial low-grade tumours that are sufficiently distant from the facial nerve (Lim et al., 2005). If there is normal preoperative facial nerve function and an absence of microscopic perineural infiltration, the facial nerve should be carefully preserved during surgery. If the facial nerve is unfortunately infiltrated, then a radical parotidectomy with resection of parts of the nerve is required (Yilmaz et al., 2012). Patients who are found to have regional spread to cervical lymph nodes will also undergo a modified radical neck dissection.
In all types of parotid malignancy, postoperative radiotherapy is indicated for advanced stage disease, intermediate or high-grade tumours, close or positive margins, lymph node metastases, or bone and perineural invasion (Lee et al., 2017). If the parotid cancer is unresectable, for example, if it involves the skull base, then radiotherapy may be the definitive treatment of choice.
In the case of parotid lymphoma, although surgical open biopsy may be performed, radiotherapy and chemotherapy form the basis of treatment and are tailored to the specific grade and histological type (Feinstein et al., 2013). Chemotherapy does not currently play any role in the standard treatment of other primary parotid malignancies (Yilmaz et al., 2012).
KEY POINTS
The parotid gland is the most common site for salivary gland tumours, accounting for 80% of cases Approximately three quarters of these are found to be benign Features of malignancy include rapid growth of the mass, pain, facial paresis, numbness and weight loss All patients with a swelling in the parotid gland for more than 3 weeks should be referred for urgent specialist review by Otolaryngology on a suspected cancer referral pathway Investigations will include FNAC or core biopsy, ultrasound imaging, and cross-sectional imaging with MRI Surgical resection forms the mainstay of treatment for both benign and malignant parotid tumours
ORCID iDs
Dr Edward Balai https://orcid.org/0000-0003-1086-1552
Dr Karan Jolly https://orcid.org/0000-0002-0344-282X