
Abstract
The global prevalence of hypertension is high and continues to rise, making it an increasingly common condition managed in primary care. Untreated hypertension can cause end-organ damage leading to complications that increase morbidity and mortality from cardiac, renal, and cerebrovascular disease. Hypertension can significantly affect an individual patient’s quality of life and can cause a considerable strain on the healthcare system. If hypertension is detected early, these events are avoidable, as there is an opportunity for intervention at a much lesser cost. Several proven, highly effective, and well-tolerated lifestyle and drug treatment strategies can achieve reduction in blood pressure. The aim of this article is to illustrate evidence-based steps that are applicable in the diagnosis and management of hypertension in primary care.
Clinical case scenario
Mr Gibbons, a 54-year-old male who works as a heavy goods vehicle driver presents to his GP for blood pressure (BP) assessment after he was found to have high BP at a routine health check.
His BP in the left arm is 170/98 mmHg, there is no significant inter-arm BP difference. He agrees for ambulatory BP monitoring and baseline investigations; his assessment shows no evidence of end-organ damage.
His ambulatory daytime average BP reading is 148/96 mmHg. Blood results show raised cholesterol only, his QRISK is 12%. He is diagnosed with stage 1 hypertension and offered the treatment option of medication combined with lifestyle modification. Initially, he is keen to solely try lifestyle modifications. After 3 months, his BP is 164/94 mmHg, he says he has been worrying about losing his job due to his high BP. The opportunity is taken to discuss the contribution of stress and anxiety to BP, the role of risk factors, complications, and the Driver and Vehicle Licensing Authority rules relating to hypertension. He is started on an angiotensin-converting enzyme inhibitor, but due to a persistent dry cough this is switched to an angiotensin receptor blocker. Monitoring bloods are organised and a review arranged in 4 weeks. At this review his BP is 132/80 mmHg, which is within the treatment target range.
Epidemiology and aetiology
More than 25% of the adult UK population has hypertension. The 2018 UK Health Survey for England reported a prevalence of 30% in men and 26% in women. The prevalence of hypertension rises to more than 50% in people aged over 60 years. It is estimated that for every 10 people diagnosed with hypertension in England, a further seven remain undiagnosed. Globally, approximately 25% of adults have hypertension, and it is projected to affect more than 1.5 billion people worldwide by 2025 (Public Health England, 2017).
There is evidence from a systematic review (Ettehad et al., 2016) that with every 10 mmHg reduction in BP, there has been:
A 17% reduction in coronary heart disease A 27% reduction in stroke A 28% reduction in heart failure A 13% reduction in all-cause mortality
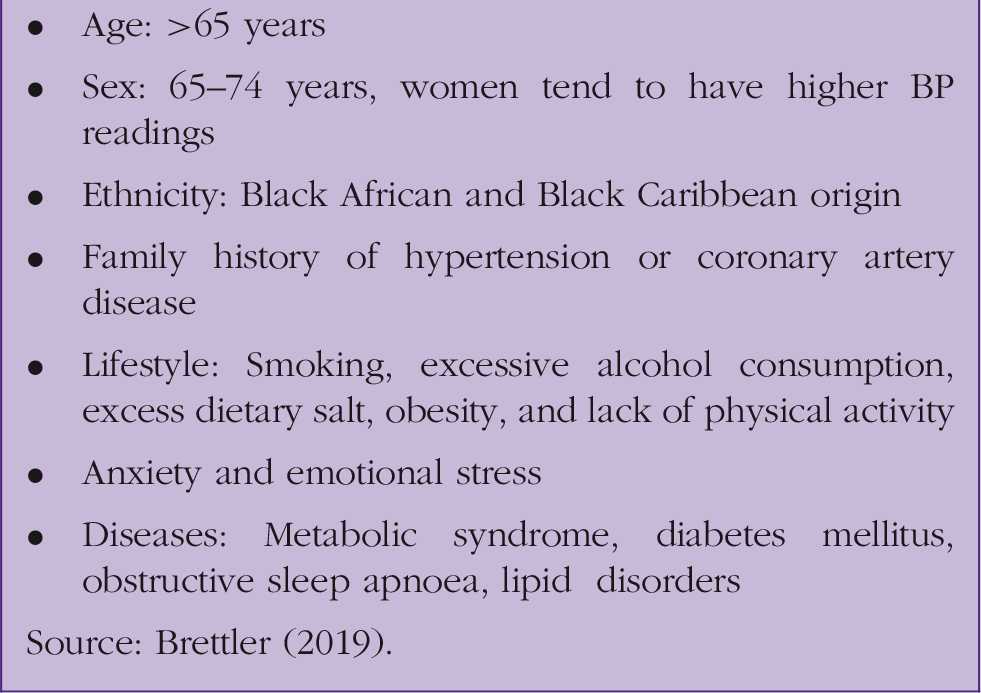
Risk factors for hypertension.
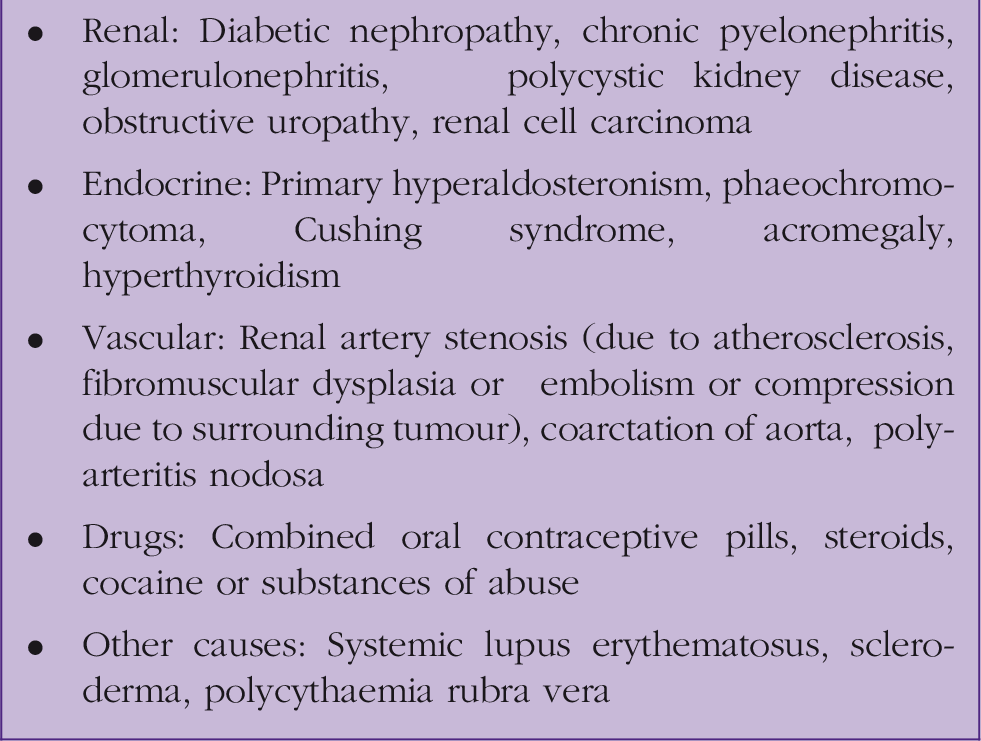
Causes of secondary hypertension.
Defining hypertension
The National Institute for Health and Care Excellence (NICE) defines hypertension as: persistently elevated clinic blood pressure readings of 140/90 mmHg or higher and either a subsequent ambulatory BP monitoring (ABPM) daytime average or home BP monitoring (HBPM) average of 135/85 mmHg or higher (NICE, 2019a).
Stages of hypertension.

Source NICE (2019b).
In the European Society of Cardiology and European Society of Hypertension (ESC/ESH) 2018 guidelines, hypertension is defined as clinic systolic blood pressure of ≥140/90 mmHg, which is equivalent to a 24-hour average ambulatory BP measurement of ≥130/80 mmHg (daytime or awake mean ambulatory reading is BP ≥135/85 mm Hg and night-time/asleep mean ambulatory reading is BP ≥120/70 mm Hg), or a home BP measurement average of ≥135/85 mmHg (Williams et al., 2018).
The American College of Cardiology/American Heart Association guidelines (ACC/AHA) 2018 advocate a diagnostic threshold of 130/80 mmHg, however, they advise treatment below 140/90 mmHg if risk factors are present. This recommendation is largely based on the results of the SPRINT study (Williamson et al., 2016), a randomised trial of intensive versus standard BP treatment. Their methodology included taking three BP measurements after a 5-minute rest. Therefore, these readings were likely to be lower, one reason why NICE have not approved lower thresholds (NICE, 2019b).
White-coat hypertension refers to the condition in which BP measured in a clinic setting is consistently higher than when measured at home. ABPM or HBPM helps in identifying this diagnosis. There should be a difference of at least >20/10 mmHg between the clinic and average daytime home or ambulatory measurements at the time of diagnosis. Masked hypertension refers to a condition where BP is consistently less than the diagnostic threshold (<140/90 mmHg) in the clinic, but is elevated when measured outside of the clinic. This is diagnosed by either ABPM or HBPM. Isolated systolic hypertension is the term used to define hypertension when only systolic BP is raised and has a value of more than or equal to 160 mmHg.
Malignant hypertension and referral criteria
Malignant or accelerated hypertension is defined as marked elevation of BP to 180/120 mmHg or higher, which is associated with signs of acute end-organ damage, such as retinal haemorrhage and/or papilledema, or life-threatening symptoms such as acute chest pain, heart failure, new onset confusion or acute kidney injury. This requires urgent same-day specialist review and urgent admission for BP control. Urgent same-day assessment is also required if phaeochromocytoma is suspected based on significantly elevated BP along with symptoms such as headache, pallor, diaphoresis and abdominal pain. In asymptomatic patients with severe hypertension (BP ≥ 180/120 mmHg) in the absence of signs of target organ damage, an urgent same-day referral to secondary care is usually not needed. The investigations for target organ damage should be arranged as early as possible, and if damage is evident, antihypertensive drug treatment should be initiated immediately without ABPM/HBPM. If there is no evidence of target organ damage in clinical or laboratory findings, the clinic BP should be repeated within 1 week and if the second clinic BP confirms severe hypertension, treatment should be initiated.
Making a diagnosis of hypertension
Diagnosis of hypertension has implications in terms of a patient’s perception of health, future health risk and need of treatment, it is therefore important to be accurate. In general, do not diagnose hypertension based on a one-off clinic reading.
BP should be measured in both arms at the initial visit, using an appropriate cuff size for the arm circumference. When there is a difference in BP between arms, the arm with the higher BP reading should be used for all subsequent visits, and the treatment target should be aimed at this arm’s BP reading. A significant inter-arm systolic BP difference (if difference in both arms is >15 mmHg systolic) should be seen as an important cardiovascular risk marker, it is associated with higher risk of cardiovascular events, including mortality in people without any pre-existing vascular morbidity (Clark et al., 2016). In people with type 2 diabetes, aged ≥80 years, and patients with symptoms of postural hypotension (e.g. dizziness) standing BP should be measured after the patient has stood for at least a minute. If there is significant postural drop in systolic BP (>20 mmHg), measure all subsequent BP values in such patients in a standing position.
When clinic BP in a person is ≥140/90 mmHg and <180/120 mmHg, ABPM is advised to confirm the diagnosis of hypertension. Alternatively, HBPM can be advised for those where ABPM is not tolerated. When using ABPM to confirm a diagnosis, make sure at least two BP measurements per hour are taken during a person’s waking hours (for example, 08:00 and 22:00) and use the average value of at least 14 measurements. On the other hand, for HBPM, advise the patient to record at least two BP measurements twice daily, ideally morning and evening for 4 to 7 days. Disregard the first day of readings and calculate the average from the remaining values. A diagnosis of hypertension can be confirmed in a person whose clinic BP ≥ 140/90 mmHg and ABPM daytime average or HBPM average of 135/85 mmHg or higher. A diagnosis of hypertension can be also confirmed in a patient without ABPM/HBPM who presents with severe hypertension (elevated BP ≥180/120 mmHg associated with evidence of target organ damage).
If hypertension is not diagnosed by ABPM or HBPM results and there is no target organ damage, NICE suggests measuring clinic BP at least every 5 years and measuring more frequently if the persons clinic BP is close to 140/90 mmHg (NICE 2019a).
Clinical evaluation
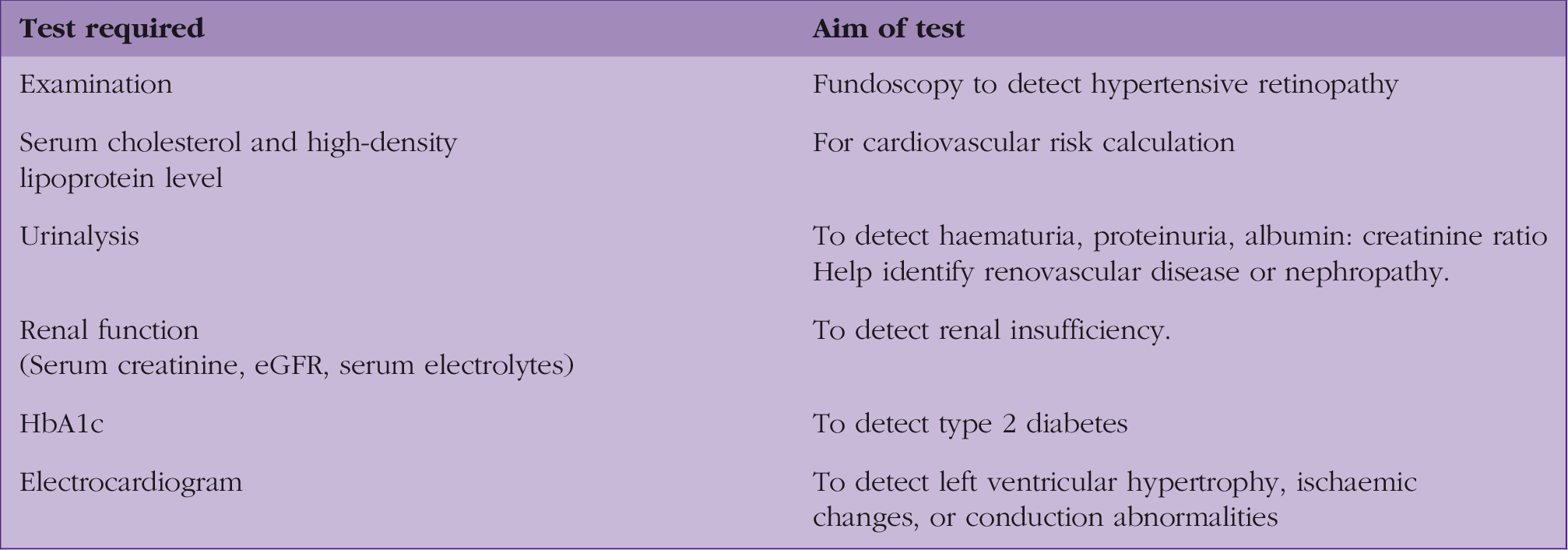
Tests required for clinical evaluation of hypertension.
Estimate the persons' 10-year risk of developing cardiovascular disease using the latest version of the QRISK assessment tool. More extensive testing is indicated if the BP is difficult to control or clinical or routine laboratory data suggest an identifiable secondary cause (Whelton et al., 2017). Some of the commonly considered special investigations are sleep studies, thyroid-stimulating hormone, plasma renin aldosterone level, pheochromocytoma screen, renal duplex ultra-sound/magnetic resonance angiography, renal arteries/computerised tomography angiography. In routine practice, if a secondary cause is suspected or a patient is resistant to standard treatment, referral to secondary care is considered for further investigations and management.
Treatment threshold and special circumstances
The treatment target threshold of BP has been debated by various studies and guidelines. The goal is to reduce morbidity and mortality from renal and cardiovascular disease (Musini et al., 2019).
Although all people with stage 1 hypertension and aged under 80 years require lifestyle advice, treatment is now suggested for those who have an estimated cardiovascular disease 10-year risk score of ≥10%, or those with either end-organ damage, or renal disease or cardiovascular disease. The reduction of cardiovascular disease risk to ≥10% from ≥20% is the major change in the NICE guideline (NICE 2019a). The guideline further suggests considering treatment in younger patients (under 60 years) with less than 10% risk where there might be concern of their lifetime risk, as risk calculators tends to underestimate life-time risk in young patients. This new recommendation means that most patients with stage 1 hypertension aged between 60 and 80 years will now be eligible for treatment, which may cause significant impact on primary care practices. However, evidence suggests that around 50% of these patients with uncomplicated stage 1 hypertension are already on antihypertensive drugs, suggesting little additional workload for practices (Sheppard et al., 2018).
NICE (2019b) recommends a clinic BP target of <140/90 mmHg or 135/85 mmHg if using HBPM for everyone aged under 80 years, including people with type 2 diabetes. The treatment target thresholds for type 2 diabetes patients have now been brought in-line with people who do not have diabetes. This is based on evidence from the ACCORD study, that there is no risk reduction (non-fatal myocardial infarction, stroke, or death from cardiovascular cause) from achieving lower BP targets of 120 mm Hg systolic compared with standard 140 mmHg in people with diabetes (Cushman et al., 2010). NICE (2019b) has relaxed the treatment threshold in those aged over 80 years to 150/90 mmHg, this is to avoid risk of falls and adverse effects, although this needs to be individualised by taking frailty and co-morbidities into account, particularly where treatment below 150 mmHg is being considered.
In patients with symptoms of postural hypotension, treatment should be targeted at the standing BP level, this is to avoid over treatment and prevent risk of falls. Ideally the target needs to be individualised based on factors such as patient preference, adverse effects, presence of cardiovascular disease risk, co-morbidities, or frailty.
The European guidelines 2018 approve a target of <140/90 mmHg in all patients and, if treatment is tolerated, a BP target of ≤130/80 mmHg in most patients, even in older patients, the target has been intensified to ≤130–140/80 mmHg (Williams et al., 2018).
Management
All patients should have the risks associated with hypertension and the need for adequate control by changing lifestyle habits or adhering to medications when necessary explained to them. It is essential to identify patients' ideas, concerns and expectations and address them. Offer patient information leaflets and signpost to useful online resources such as the ‘blood pressure information resource BPassoc’, the British Heart Foundation or patient.info.
Lifestyle modification
Lifestyle modification should be recommended to all patients with suspected or diagnosed hypertension at all stages. A 3-month trial of lifestyle modification is recommended before commencing pharmacological therapy. However, most patients will require drug therapy alongside lifestyle changes to eventually achieve their target reading. Lifestyle changes include weight reduction to maintain waist circumference of <102 cm for men and <88 cm for women and a body mass index of 25 kg/m2. It can also improve the efficacy of antihypertensive medications and the cardiovascular risk profile (Mancia et al., 2013). Increasing physical activity to at least 30 minutes of moderate-intensity, dynamic aerobic exercise (walking, jogging, cycling, or swimming) five days per week, as tolerated. Managing weekly alcohol consumption, encouraging smoking cessation and promoting a healthy diet that includes plenty of fruits and vegetables, whole grains, sodium reduction (≤1.5 g/day) and low-fat proteins is recommended.
Pharmacotherapy
The pharmacological treatment for people with hypertension is summarised in a flow chart in Fig. 1. At each step of therapy, it is important to optimise medication dose and check compliance before moving on to the next step. If BP cannot be controlled with a single medication, a second medication from a different class is added. Consider resistant hypertension if BP remains uncontrolled in people taking optimal doses of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, a calcium channel blocker and a thiazide-like diuretic. In such people, adherence should be checked, and elevated BP should be confirmed using ABPM/HBPM as well as considering specialist advice. In step 4, if further treatment is indicated for resistant hypertension use low-dose spironolactone for adults who have potassium levels ≤4.5 mmol/L or an alpha-blocker or beta-blocker for those with serum potassium more than 4.5 mmol/L. If BP remains uncontrolled despite taking optimal doses of four drugs, then seek specialist advice.
Hypertension treatment flow chart.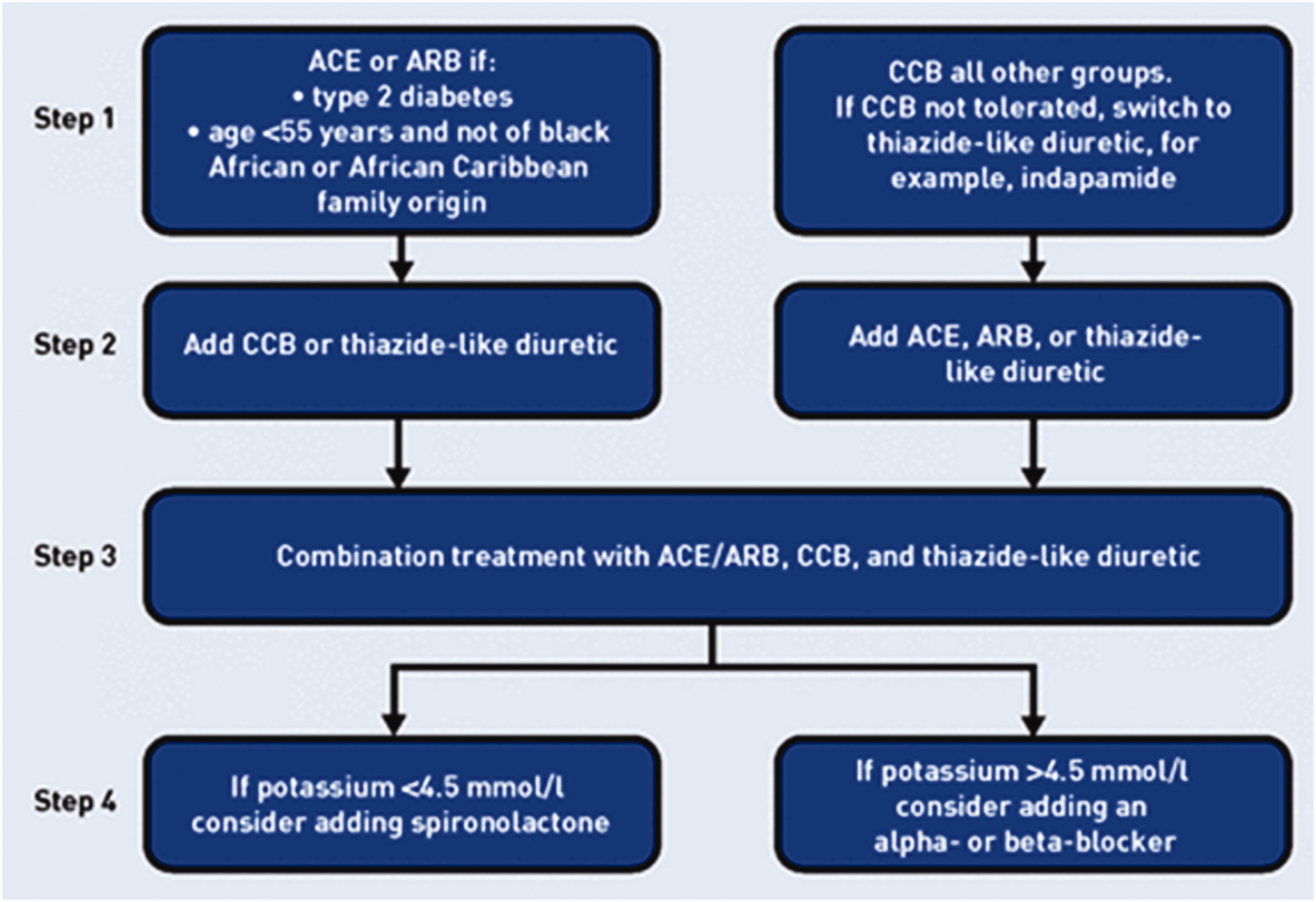
Annual review
When BP reaches the target range and treatment is well tolerated, a review in 12 months is recommended (NICE 2019a). At these reviews, reiterate the importance of lifestyle amendment, check compliance with medication and assess for the presence of any new symptoms or signs to suggest end-organ damage. Check renal function, and perform urinalysis to check for haematuria, proteinuria, and albumin-to-creatinine ratio.
Fitness to drive in hypertension
Fitness to drive advice in hypertension.

Reproduced from GOV.UK. Cardiovascular disorders: assessing fitness to drive, under the terms of the Open Government Licence v3.0
KEY POINTS
If there is inter-arm BP difference of ≥15 mmHg systolic, use the arm with higher reading for subsequent measurements and the treatment target should be based on this arm’s BP reading In people >80 years, type 2 diabetes, and patients with symptoms of postural hypotension measure BP and record subsequent BP readings in a standing position People with severe hypertension (clinic BP ≥ 180/120 mmHg) and acute signs such as chest pain, new onset confusion, heart failure, acute kidney failure, retinal haemorrhage or papilledema should be referred for a same-day specialist review In asymptomatic people with clinic BP ≥ 180/120 mmHg and no signs of acute target organ damage, a same-day specialist review is usually not needed, but investigations for target organ damage should be carried out as soon as possible and clinic BP should be repeated within a week The threshold cardiovascular risk score (the risk of having a stroke or heart attack in the next 10 years) for initiation of drug therapy in stage 1 hypertension has been reduced to 10% for patients under age 80 years in age; drug therapy should be initiated in patients with stage 1 hypertension and end-organ damage, renal disease or cardiovascular disease The diagnostic and treatment threshold for hypertension are now the same for people with or without diabetes
ORCID iD
Dr Ayesha Afroze https://orcid.org/0000-0003-4570-2463