
Abstract
Dyspareunia is persistent pain on attempted or successful vaginal penetration. It is under-reported, infrequently asked about by healthcare professionals, and affects quality of life and relationships. Dyspareunia is multifactorial and possesses biopsychosocial components. Pain may be distinct and localised, deep or persistent. Among the symptoms, women describe sensations of aching, throbbing and tearing. Disinterest in sex and relationship problems can result. This article discusses dyspareunia, its common differential diagnoses and aims to improve clinician confidence in assessing and managing dyspareunia in primary care.
Clinical case scenario
Julie, a 22-year-old woman attends the surgery complaining of vaginal discomfort. She has been frequently treated for candida.
On direct questioning it becomes apparent that Julie and her partner have attempted vaginal intercourse, but Julie has found even digital penetration painful. She has been experiencing symptoms for 6 months, but has not disclosed due to embarrassment. Julie has had no previous partners. On external examination there are no signs of infection or candida.
Julie cannot tolerate vaginal or speculum examination. A good therapeutic relationship is developed. You suspect vaginismus and offer explanations for the symptoms. Julie is referred for psychosexual therapy.
Definition
A consensus definition for dyspareunia is: Persistent or recurrent difficulties of the woman to allow vaginal entry of a penis, a finger, and or any object, despite the woman’s expressed wish to do so (Basson et al., 2004)
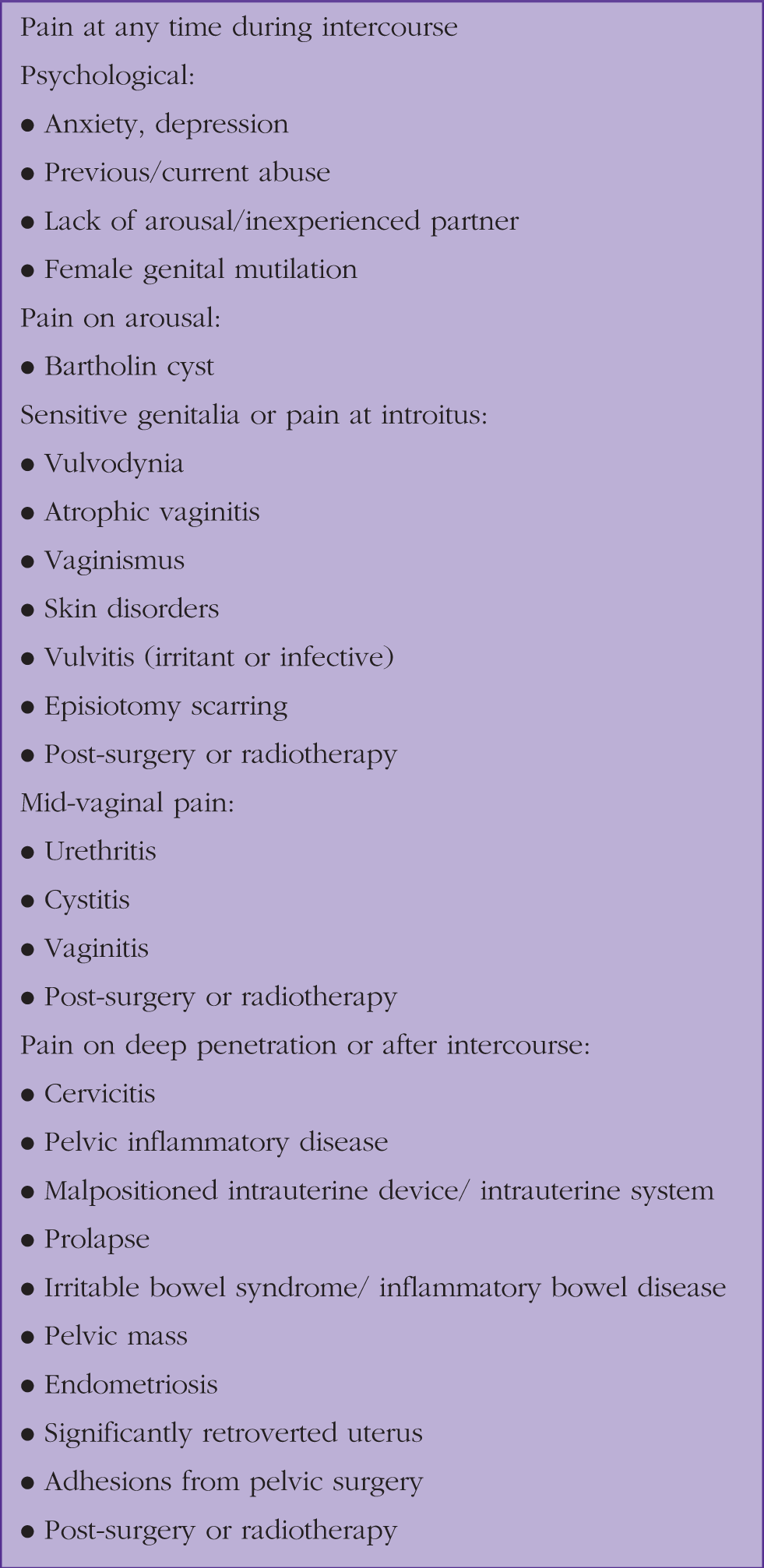
Pain can occur from any part of the genital tract, at any time during intercourse. There are multiple causes, many of which are treatable.
Epidemiology
The prevalence and incidence of dyspareunia are probably significantly underestimated. Global prevalence estimates vary from 3–18%, with 7.5% women in a large UK survey reporting dyspareunia (Mitchell et al., 2017).
Causes
Symptoms and causes of dyspareunia: adapted from Payne, 2016.
Principles for assessment
Assessment aims to identify medical or gynaecological causes of dyspareunia and gather psychosexual information. Management depends on the cause and usually involves a multidisciplinary approach. Considering the pain as biologically mediated or psychological is an oversimplification (Mitchell et al., 2017).
History and symptoms
A detailed history should be taken in a sensitive manner. Questions should include a clarification of what the patient is experiencing, a detailed pain history, whether dyspareunia is of new onset (secondary) or has always been present (primary) and at what point during intercourse the pain starts. It is useful to establish if anything else causes the same pain, or if anything facilitates successful intercourse.
Symptoms of a specific cause should be explored, including whether there has been a recent change of sexual partner, any skin changes, vaginal discharge, intermenstrual or post-coital bleeding and whether menopausal symptoms or vaginal dryness are present. It is important to establish if there are symptoms of other medical conditions that could cause the dyspareunia, such as irritable bowel syndrome, endometriosis or urinary tract infection (UTI), among others.
The psychosocial context should be explored, including mood, anxiety and previous traumatic experiences. Consider asking directly about abuse or any forced/coerced sexual activity. Discuss the relationship with her partner, how the dyspareunia affects them both and whether she has had the same problem with other partners.
Understanding symptom onset is important. A sudden onset may suggest a psychological cause, whereas a more gradual onset may suggest a physical cause (Lee et al., 2018). Exploring recent life events can identify triggers (Lee et al., 2018).
Joint consultation with the couple may be beneficial in facilitating dialogue, identifying shared goals and promoting joint commitment to management (Payne, 2016). If coerced sexual activity is suspected, interviewing the woman alone is essential. Consider a psychosexual assessment (Lee et al., 2018) with an open approach, allowing patients to discuss psychosexual aspects of dyspareunia and explore anxiety, fear, anger or other emotions.
Examination and signs
Physical examination is important in dyspareunia. Women may be extremely concerned about genital or speculum examination. This should be understood, and one should consider booking multiple appointments over time.
Facilitating a relaxed, comfortable environment for examination is crucial. A preferred gender clinician should be offered where possible. An appropriately trained chaperone must be offered for intimate examination in all circumstances (General Medical Council (GMC), 2013). Cultural and language needs must be considered, for example preferred gender interpreters to explain the examination and gather consent.
Suggested approach
The abdomen should be examined to palpate for any pelvic masses or tenderness suprapubically (Lee et al., 2018). External genitalia should be examined and consider testing for provocation of vulvodynia using a cotton bud to test for vulval sensitivity or pain (Reed, 2006). Examination in the left lateral position while asking to cough, or when standing helps assess for uterovaginal prolapse (Thiagamoorthy, 2018).
Observe the condition of the external genitalia, including skin changes, dryness or inflammation and if there is any sign of scarring or female genital mutilation (FGM). Assess for swellings or lesions suggestive of herpetic ulcers or Bartholin’s cysts.
If the woman agrees, digital vaginal examination by an appropriately trained clinician can add diagnostic value. Asking the woman to clench and relax the vaginal muscles can be helpful (Payne, 2016). In some instances, the digital examination itself may promote painful vaginal contractions suggestive of vaginismus (Crowley et al., 2009; Payne, 2016).
Bimanual examination is indicated. Cervical motion tenderness or excitation is a sign of pelvic inflammatory disease (PID) requiring urgent treatment (Payne, 2016). Assess the size, shape, position and mobility of the uterus. Palpable masses require further investigation.
Rule out UTI if symptoms are suggestive and consider vaginal swabs for chlamydia and gonorrhoea; opportunistic cervical screening can be undertaken if indicated. A pregnancy test should be considered.
Dyspareunia alongside repeated UTI, vaginal infections or incontinence may prompt suspicion of FGM. Questioning should be sensitive and non-judgemental in nature. Department of Health guidance suggests two introductory questions:
Do you, or your partner, come from a community where cutting or circumcision is practiced? Have you been cut?
If answering yes, examination should be sensitively discussed, to identify the type of FGM. Onward referral to an FGM specialist may be necessary. If identified, there is mandatory reporting for patients less than 18 years of age and important considerations for the woman and family members; an FGM safeguarding pathway is available from the Department of Health (Department of Health and Social Care, 2017).
Differential diagnosis and management
Vaginismus
Vaginismus describes painful vaginal contractions in response to physical contact. Women with vaginismus often avoid intercourse, experience pelvic muscle contraction involuntarily, and may anticipate and experience pain with any form of penetration. Biopsychosocial mechanisms usually contribute (Crowley et al., 2009).
Vaginismus can be lifelong (primary) or develop after previously normal sexual function. It may be situational and dependent on partner or circumstance, or global (Crowley et al., 2009). Women with total vaginismus are unable to tolerate penetration at all; women with partial vaginismus can tolerate penetration with discomfort and pain. Fear of the pain associated with penetration rather than simply physical muscle spasm may be present (Crowley et al., 2009).
Further questioning should establish if penetration is possible, for example, whether she can insert fingers or tampons. Discussion of levels of anxiety at the thought of penetration is useful, as is exploring the onset and enquiring about previous traumatic sexual experiences.
If vaginismus is suspected, examination is indicated to rule out contributing physical causes. External genitalia usually appear normal on observation. Digital examination may reveal painful or involuntary vaginal muscle contraction suggestive of vaginismus (Crowley et al., 2009). Women with vaginismus may struggle to tolerate speculum examination even with a virgin speculum.
Once the diagnosis is made, treatment strategies include progressive relaxation, a sequence of tensing and relaxing specific muscle groups which is taught prior to self-fingering or insertion of vaginal trainers. Explanation of the anatomy and exploration of concerns may help some women (Crowley et al., 2009).
Desensitisation/vaginal trainers can be used to treat vaginismus. Desensitisation is a behavioural therapy used to treat anxiety disorders. Women are exposed gradually to more anxiety-provoking situations (increasing sized vaginal trainers) until these are tolerated comfortably (Crowley et al., 2009).
Local referral pathways differ, but generally referral to an integrated sexual health service or specialist gynaecological physiotherapy is required. Treatment is usually with guidance from specialist therapists, with subsequent exercises/use of vaginal trainers at home.
Cognitive behavioural therapy (CBT) may improve vaginismus (terKuile et al., 2007), or referral for psychosexual counselling may be indicated (Crowley et al., 2009). Many local areas have psychosexual services, although waiting times can be long.
Treatments such as Botox, hypnotherapy, topical lidocaine and antidepressants have had mixed effects; there is a lack of robust data on the best treatment strategy for women (Crowley et al., 2009). Often specialist advice is required from gynaecologists, psychiatry and/or psychosexual specialists.
Self-help resources are available. These include support groups and information about causes and treatments. Home-use vaginal dilators are available to purchase with guidebooks that support women to use these effectively; vaginismus.com is a helpful resource (www.vaginismus.com/). Women can self-refer privately to vaginismus or vulval/vaginal pain specialist physiotherapists for support and treatment. The ‘squeezy directory’ (www.squeezyapp.com/directory/) was designed to facilitate easier access for women to these services.
Vulvodynia
Vulvodynia is chronic vulval pain for 3 months or longer without an identifiable cause. The diagnosis should be made after ruling out other causes, alongside evidence of eliciting pain on response to light pressure on the vulva.
Vulvodynia can be either localised or generalized in nature. Most women have pain at one specific site of the vulva. If the pain is in the area surrounding the vaginal opening (the vestibule) this is termed vestibulodynia. Most women with vestibulodynia have provoked vulvodynia. This is when pain occurs during or after application of pressure on the vestibule. This may be due to a tampon being inserted, gynaecological examination or sexual intercourse. Ninety-one percent of sufferers report that sexual intercourse worsened the pain of vulvodynia.
With generalised vulvodynia, pain occurs spontaneously and is relatively constant. Sexual intercourse typically exacerbates the symptoms. Symptoms may have been present since childhood or may develop after years of painless sex. Pain is often described as burning, sharp or prickly. Pain often begins suddenly when provoked, but dissipates gradually. It can last hours or even days after intercourse (Reed, 2006).
Vulvodynia is most common in women aged between 20 and 50 years (Reed, 2006). On examination, the vulva may be mildly erythematous. Rashes, altered mucosa and ulceration are not consistent with vulvodynia; further investigation of the cause for these problems needs to be undertaken (Reed, 2006). A cotton swab used to gently indent several locations of the labia and introitus on examination will elicit discomfort in most women with vulvodynia. Allodynia (when non-noxious stimuli cause pain) or hyperpathia (when stimuli cause far greater pain than expected) suggests a neuropathic cause for the symptoms (Reed, 2006).
If vulvodynia is confirmed with history and examination, the British Society for Study of Vulval Disease suggests a multidisciplinary approach to treatment (Mandal et al., 2010). Few randomised control trials exist, meaning guidance is based on lower-quality evidence.
Avoidance of irritants such as soaps, use of loose-fitting cotton underwear, antihistamines or antifungal treatments may benefit some women. Topical lidocaine used as required, once daily at night or before sexual intercourse, relieves symptoms in some cases (Mandal et al., 2010).
Tricyclic antidepressants, gabapentin and pregabalin have been used to some effect in published studies (Mandal et al., 2010). Amitriptyline in doses of 10–100 mg can be effective. Unfortunately, side effects often limit use. Venlafaxine and paroxetine have been suggested as alternatives. In practice, most GPs would seek further advice from specialists if no improvement after a trial of treatment with neuropathic painkillers.
CBT or a more extensive pain management approach may be required. If there are psychological issues, for example, anxiety around provoking pain leading to avoidance of intimacy, exploring a psychological/psychosexual approach may be helpful (Mandal et al., 2010).
Surgery was previously considered to be the main treatment for vulvodynia. Nowadays, vestibulectomy is reserved for women with localised, but severe, debilitating symptoms. For women with intractable and severe vulvodynia, there may be some benefit (Lavy et al., 2005).
Self-help resources are available. The National Vulvodynia Association (www.nva.org/for-patients/self-help-tips/) and Vulval Pain Society (www.vulvalpainsociety.org/vps/) are particularly useful reources to which to signpost women. The latter includes support for common vulval skin complaints.
Pelvic inflammatory disease
PID is a general term used to describe infection of the upper genital tract. It is most commonly due to a sexually transmitted infection (STI), with Chlamydia trachomatis being the most common causative organism. Neisseria gonorrhoeae, Mycoplasma genitalium and normal vaginal flora may be causative (National Institute for Health and Care Excellence (NICE), 2019). Risk factors for PID include age under 25 years, multiple partners, recent new partner, history of STI in either partner, recent uterine instrumentation or termination of pregnancy (NICE, 2019).
The classic presentation of PID is with secondary, deep dyspareunia of sub-acute onset. Women may describe fever, abdominal pains, abnormal discharge and change to menstrual bleeding pattern. Examination may reveal lower abdominal tenderness, adnexal or cervical motion tenderness, mucopurulent discharge or cervicitis.
Management of PID is normally completed by genito-urinary medicine (GUM)/sexual health clinics, to ensure cultures for gonorrhoea are taken, treatment of partners and contact tracing. PID is a clinical diagnosis and if suspected, same-day referral to a specialist clinic is indicated to ensure appropriate antibiotics are prescribed as soon as possible (NICE, 2019). Antibiotic treatment should not be delayed while awaiting test results.
Vulvitis and STIs
Vulvitis from infection may cause dyspareunia, often superficial dyspareunia, of recent onset. Vaginal discharge, vulval ulceration or inflammation, changes in bleeding pattern and post-coital bleeding may indicate infection, which may be sexually or non-sexually transmitted.
Candida
Superficial dyspareunia with new onset cottage cheese/curd-like discharge suggests candida infection; most commonly Candida albicans. If the diagnosis is clear from history and examination, swabs may not be necessary. General advice around hygiene and loose-fitting cotton underwear should be given. For mild thrush, clotrimazole cream or pessary or a one-off dose of oral fluconazole are usually sufficient to resolve the symptoms.
If candidiasis is severe with vulval erythema, oedema, fissuring and excoriation, vaginal/vulval swabs are indicated. Non-albicans candida species may be identified. Recommended treatment is two doses of oral fluconazole 150 mg, or 500 mg clotrimazole pessaries taken 3 days apart (NICE, 2017a).
In recurrent candida, swabs should be taken and predisposing causes, such as diabetes, considered. Initially prescribe an induction course of oral fluconazole 150 mg, or intravaginal antifungals, three doses 3 days apart. Treatment should be continued with oral fluconazole or intra-vaginal antifungal to be used weekly for 6 months (NICE, 2017a).
Herpes
Painful genital blisters or ulcers, both with and without lymphadenopathy and discharge, suggest herpes infection. This may be extremely painful and distressing. There is risk of secondary bacterial infection. Acyclovir can be given as treatment, and advice about gentle bathing in salt water, keeping the area clean and dry and using regular analgesia should be given. Referral to GUM is ideal for first infection, for full advice and confirmation on PCR swab. A full STI screen including HIV and syphilis tests should be offered. If the patient declines referral to GUM, these tests can be carried out in primary care.
Bacterial vaginosis, trichomonas or retained tampon/foreign body
Offensive smelling discharge may indicate bacterial vaginosis, trichomonas or retained tampon/foreign body, any of which may cause dyspareunia. Bacterial vaginosis uncommonly causes dyspareunia directly, but the offensive odour may lead to avoidance of intimate relationships when present. If the diagnosis is clear, swabs to confirm may not be required. Treatment is with oral or intravaginal metronidazole. Clindamycin is an alternative (Hay et al., 2012).
If vulvitis or vaginitis is present, swabs for trichomonas should be offered and taken from the posterior fornix. If positive, metronidazole 400 mg BD for 7 days is the recommended treatment (Sherrard et al., 2014). Sexual contacts should be tested for trichomonas and treated if necessary.
Chlamydia and gonorrhoea
With dyspareunia, alongside dysuria, changes in discharge, abdominal pain or bleeding pattern Chlamydia Trachomatis (CT) or Neisseria Gonorrhoeae (NG) infection should be considered, particularly in the context of a recent change in sexual partner. Vulvovaginal Nucleic Aid Amplification Test (NAAT) swabs are the specimen of choice to diagnose NG or CT in women. Women may perform self-taken swabs if they wish. Urinary tests are less reliable in women. Tests for HIV and syphilis should be routinely offered as part of a sexual health screen (Nwokolo et al., 2015).
If the woman tests positive for CT or NG, referral to sexual health is appropriate. This allows contact tracing, a full screen and specialist advice. If the woman declines, treatment for CT is doxycycline 100 mg BD for 7 days (contraindicated in pregnancy), or azithromycin 1 g orally, followed by 500 mg OD for two further days (Nwokolo et al., 2015). If a woman is NG positive she should be strongly encouraged to attend a sexual health clinic for treatment, with a 1 g injection of ceftriaxone likely to be needed (Fifer et al., 2020).
Lichen planus
Lichen planus is an erosive dermatosis that affects the mucosa of the mouth and the vagina. The erosions cause significant dyspareunia and can lead to vaginal stenosis. Women may report superficial dyspareunia, with bleeding, burning or pruritus (Lotery and Galask, 2003). It should be suspected in cases of erosive skin lesions with vaginal narrowing. Tacrolimus 0.1% ointment may be effective (Lotery and Galask, 2003); if suspected most women require referral to secondary care.
Lichen sclerosus
Lichen sclerosus (LS) is a chronic, inflammatory skin disorder. Although LS can affect any part of the body, it commonly affects the vulva and can lead to scarring, dyspareunia and sexual dysfunction (Krapf et al., 2020). It peaks in pre-pubertal girls with a prevalence of around 0.1%, and again in post-menopausal age women, with an estimated prevalence of 3%. It is under-reported, under-recognised by clinicians and may be misdiagnosed for several years.
Patients may report itching, soreness, dysuria and superficial dyspareunia (Lewis et al., 2018). Examination reveals white, atrophic patches, with a ‘cigarette paper’ appearance of wrinkling of the epidermis. Depigmentation, hyperpigmentation, ecchymoses, fissuring and resorption of the labia can occur. LS rarely involves the vaginal mucosa, but can affect the labia minora, inner labia majora, inter-labial sulcus, clitoris, vestibule, perineum and perianal region (Krapf et al., 2020). A small risk of transition to squamous cell carcinoma is associated with LS (Lewis et al., 2018).
The aetiology is unclear, but it is likely an autoimmune condition occurring in women with a genetic predisposition. Studies suggest sexual function is significantly impacted, with women reporting painful sex, less desire, lubrication, orgasm and satisfaction before and after treatment (Krapf et al., 2020).
Although there is no cure, there are treatments which induce remission and prevent progression of the disease. Treating LS may improve dyspareunia; however, some women report sexual dysfunction even after adequate treatment (Burrows et al., 2011).
Gold standard treatment is with ultrapotent topical corticosteroids, using clobetasol propionate 0.05% and a barrier preparation (Lewis et al., 2018). Guidelines advise that unless experienced in the management of LS, hydrocortisone 1% should be prescribed alongside emollients, and referral made to a specialist with expertise in vulval disease (Lewis et al., 2018).
Psychological causes
The psychological causes of dyspareunia should not be underestimated. These can be distinct from other causes. Anxiety and stress can reduce libido and sexual arousal, which may contribute to vaginal dryness and muscle contraction (NICE, 2017b, 2020). The possibility of previous or current abuse should be considered and specifically discussed.
If depression and anxiety are present, treating these issues may improve dyspareunia and increase libido. If the patient is already taking antidepressant medication, consider the possibility that the treatment is contributing to the symptoms.
If sexual dysfunction is the primary concern, psychosexual therapies may provide most benefit. These include targeted counselling or longer-term psychotherapy. Therapy focuses on how physical and psychological factors interplay and addresses these emotionally and psychologically through techniques such as person-centred therapy, CBT or psychodynamic psychotherapy (College of Sexual and Relationship Therapists (COSRT), 2021). Other psychological interventions include relationship therapy sensate focus training and desensitisation (Crowley et al., 2009).
Pelvic organ prolapse
Women with pelvic-floor disorders and prolapse have high rates of sexual dysfunction; these conditions should be considered as a cause of dyspareunia (Thiagamoorthy, 2018). Pelvic organ prolapse is the descent of the anterior or posterior vaginal wall, uterus or apex of the vagina allowing nearby organs to herniate into the vagina. Mild prolapse is common, and unless symptomatic should not be considered pathological. Dyspareunia associated with prolapse may be due to local pressure, psychological aspects, body image or urogenital atrophy. If prolapse is identified, the grade should be assessed, and its impact discussed. Treatment options include pelvic floor exercises, physiotherapy, pessaries and referral for surgery.
Endometriosis
Dyspareunia is an important symptom in endometriosis. Typically, deep dyspareunia is described; symptoms do not necessarily correlate with the extent of endometriotic lesions. It is not completely clear how endometriotic deposits cause pain either generally or in dyspareunia. Theories include hormonal stimulation of deposits, stimulation of neural pathways, inflammation, scarring or a combination. Deep dyspareunia in conjunction with other features of endometriosis should prompt consideration of the diagnosis, investigation and referral.
Peri and post-menopausal dyspareunia
Case scenario 2
A 55-year-old woman presented with vasomotor and mood symptoms. She described severe superficial and deep dyspareunia, present for the past few years. She described intercourse as feeling ‘like a sword inside’. Examination revealed dryness and atrophy consistent with genitourinary symptoms of menopause.
She was treated with vaginal oestrogen pessaries, nightly for 2 weeks and twice weekly thereafter. Localised symptoms improved.
Dyspareunia is one of the most common problems reported by peri and post-menopausal women (Kao et al., 2008). Genitourinary symptoms of the menopause (GSM) describes symptoms arising from reduced oestrogen in the female genital tract. Reduced vaginal oestrogens result in changes to secretions, decreased collagen, increased vaginal pH and reduced vascularity.
The female genital and lower urinary tracts have a common embryonic origin, and so the urinary tract is also affected by decreased oestrogen levels post-menopausally (Faubion et al., 2020). Symptoms include dryness, atrophy, dyspareunia, dysuria and recurrent UTI (Faubion et al., 2020). Some studies suggest up to 84% women report symptoms consistent with vaginal atrophy around the menopause (Faubion et al., 2020). Low oestrogen levels may contribute to reduced arousal and lack of lubrication (Kao et al., 2008).
Dyspareunia in post-menopausal women is often multifactorial. Physical health issues are more likely, pelvic organ prolapse is common, scarring or atrophy post-surgery or radiotherapy may be present. Psychological issues relating to age, womanhood, fertility and social factors must be considered.
Many of the causes discussed in Box 1 may apply to post-menopausal women. If other conditions are ruled out, and GSM are determined as the main cause of dyspareunia, several treatment options may improve symptoms. Effectively treating post-menopausal dyspareunia may have a dramatic effect on the symptoms and quality of life. Figure 1 shows a suggested treatment approach.
Suggested treatment approach for post-menopausal dyspareunia.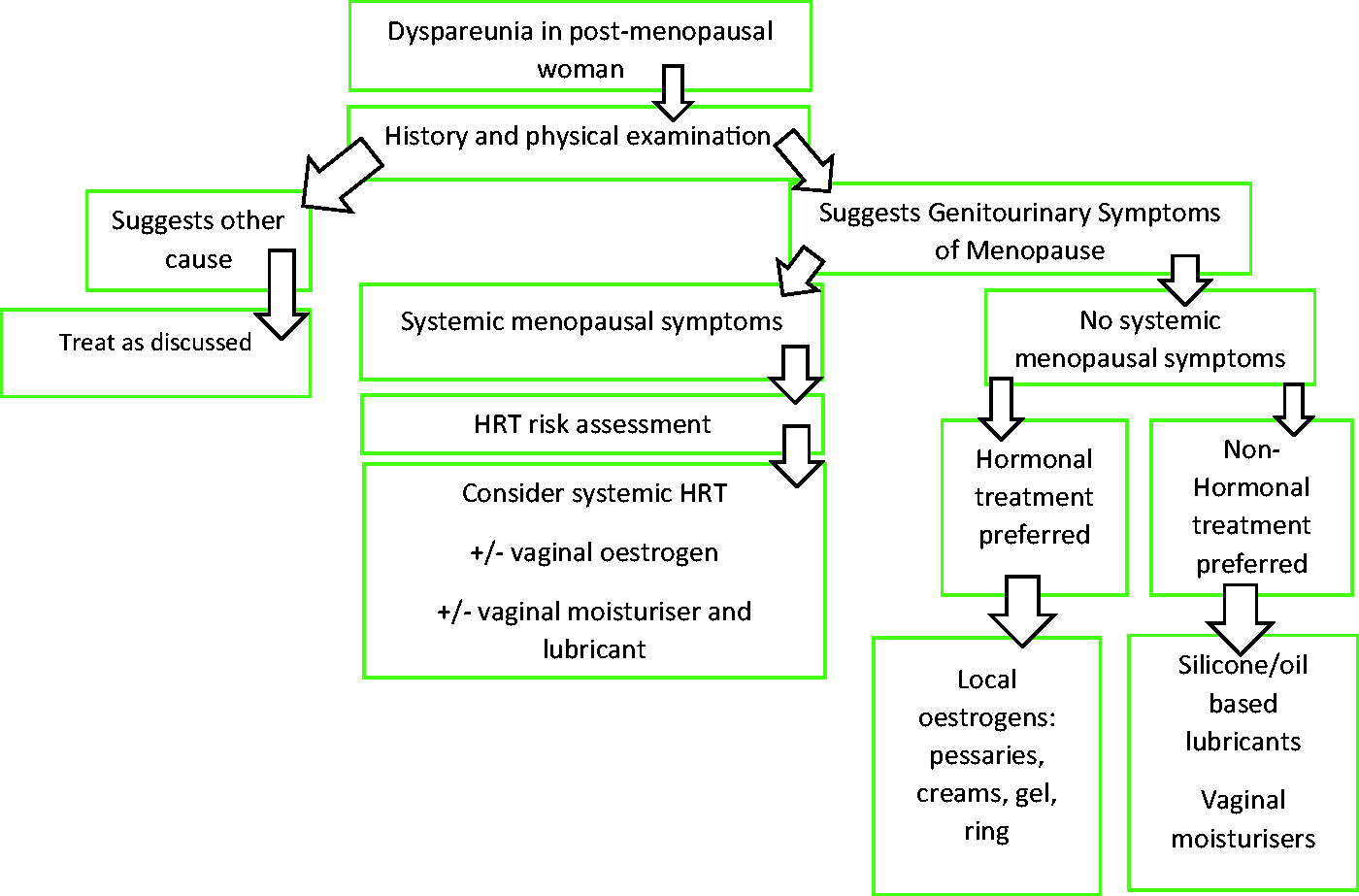
Non-hormonal vaginal moisturisers can be considered and are used three-to-four times weekly. During intercourse, lubricants can be used; silicone or oil-based lubricants may be more effective than water-based lubricants.
Systemic hormone replacement therapy (HRT) may not help local symptoms; local oestrogen treatment is more beneficial when dyspareunia is the main presenting menopausal symptom (Kao et al., 2008). Local oestrogens are equivalent to a very low dose of systemically absorbed oestrogen. Even with systemic HRT, additional vaginal oestrogens may need to be used for local symptoms. The British Menopause Society suggests continuing topical low-dose vaginal oestrogen therapy indefinitely, with annual review, if it improves symptoms (Pitkin, 2018).
Local oestrogens include creams, vaginal tablets, low and ultra-low dose pessaries, gels and an oestrogen-releasing ring. Discussion of which option is best for an individual woman should take account of patient preference. Creams and pessaries are usually applied twice weekly as maintenance after initial daily treatment for 2 to 3 weeks. Vaginal rings are changed every 3 months and have a licence for 2 years’ use. The vagina usually responds well to localised hormone treatment, with improvements in pH, moisture and comfort and reduced dyspareunia.
Prasterone is a new local treatment for menopausal vulvo-vaginal atrophy licenced for moderate-severe symptoms and is approved by some local formularies as a second-line treatment. It contains dehydroepiandrosterone , converted intracellularly to oestradiol and testosterone. It has shown efficacy compared with placebo for reducing dyspareunia, it has only local side-effects and contraindications are similar to those of other hormonal-based treatments (Labrie et al., 2016). Ultra-low dose oestrogen creams and pessaries can be useful in patients with thin atrophic vaginas, allowing symptomatic relief with fewer oestrogenic side effects.
Conclusion
Dyspareunia is under-reported, affects women of all ages and has significant effects on quality of life. Thorough history and examination in most cases can point to the cause. Exploration of the psychosexual context is important. Treatment is dependent on the cause. It may involve psychological, psychosexual and/or physical treatments, including specialist referral. Women may be reluctant to report dyspareunia. Sensitive and considerate questioning to identify women suffering from dyspareunia is crucial. The effect of dyspareunia on mental and physical health, quality of life and relationships should not be underestimated. It is important that GPs identify women suffering with dyspareunia and have knowledge of treatments for dyspareunia using appropriate, holistic, evidence-based methods.
KEY POINTS
Dyspareunia is under-reported, under-diagnosed and causes significant morbidity A careful history often points to a main cause, but the condition is multifactorial Psychosexual assessment is important Examination of the external genitalia and speculum examination are important to investigate potential physical causes Treatment is usually based on the underlying cause; referral for psychosexual counselling is an important part of management in some cases Peri and post-menopausal dyspareunia are often due to genitourinary symptoms associated with declining oestrogen levels and can be treated effectively; always enquire about genitourinary symptoms in patients with menopausal symptoms
ORCID iD
Dr Charlotte Morris https://orcid.org/0000-0002-9047-0481