
Abstract

A young male patient presents with redness in the left eye. There is no pain or change in vision. He reports having a heavy drink with subsequent vomiting the night before. Apart from wearing contact lenses, he is fit and well and takes no medications. Eye examination is as in the accompanying image.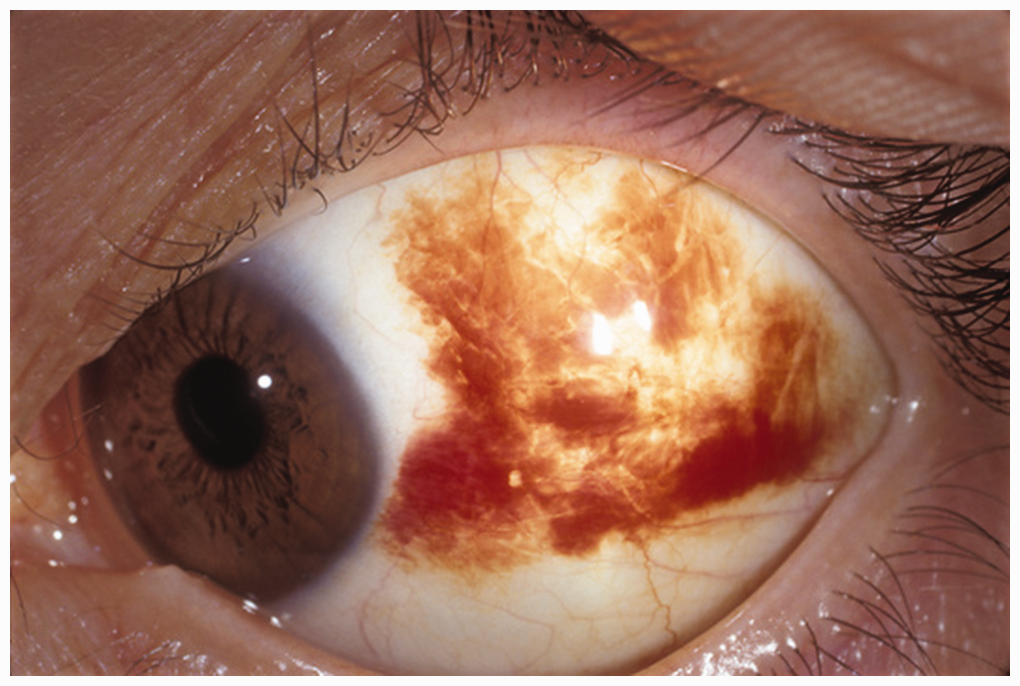 Barraquer, Barcelona - ISM/Science Photo Library.
Barraquer, Barcelona - ISM/Science Photo Library.
This is subconjunctival haemorrhage
The conjunctiva is a thin and clear membrane encompassing the white outer part of the eye (bulbar conjunctiva) and the inner surface of the eyelids (palpebral conjunctiva). The conjunctival fornices connect both. The bulbar conjunctiva covers the anterior sclera and connects to the underlying sclera through Tenon's capsule (Shumway et al., 2023). The deepest conjunctival layer contains the blood supply. Subconjunctival haemorrhage occurs when a blood vessel ruptures under the conjunctiva, causing a bright red appearance in a segment of the eye or of the entire eye.
Most subconjunctival haemorrhage (SCH) occurs spontaneously. However, it can be triggered by any sudden increase in venous or capillary pressure within the conjunctiva secondary to coughing, straining or lifting. Hypertension and diabetes are known risk factors, as well as wearing contact lenses or using anticoagulants.
SCH tends to occur more frequently on the temporal aspect of the eye owing to its larger bulbar conjunctiva and increased vulnerability to trauma (Doshi and Noohani, 2023). Patients typically present with unilateral, painless, well-demarcated redness. The vision, pupillary reflex and eye movements are not affected.
Basal skull fractures can lead to SCH with indistinct boundaries, which is secondary to blood traveling from the orbital floor to the subconjunctival space.
A history of recent eye surgery, periauricular local anaesthesia, contact lens use, anticoagulation therapy, blood disorders and recurrent SCH should prompt further workup. A detailed ophthalmic examination is crucial in confirming the diagnosis and to rule out complications or other differential diagnoses.
Bilateral isolated SCH in an infant or child, mainly when associated with facial petechiae, may be a sign of traumatic asphyxia, raising the possibility of a non-accidental injury (Spitzer et al., 2005).
Conjunctivitis is the most common cause of red eye in general practice and presents with diffuse bilateral redness and watery discharge. Episcleritis is inflammation of the thin layer between the sclera and conjunctiva, characterized by mild pain and redness with no vision changes; this in contrast with scleritis, a sight-threatening condition presenting with deep-seated eye pain and painful eye movement. Anterior uveitis is a systemic condition with photophobia, redness, miosis and anterior chamber cellular debris. Acute angle-closure glaucoma is characterized by diffuse conjunctival redness, particularly pronounced near the limbus. The pupil appears mid-dilated with a poor response to light stimuli.
An isolated SCH needs no treatment other than reassurance. The blood is gradually absorbed within a few weeks, depending on the extent of bleeding. Where the diagnosis is unclear or there is a secondary cause for the bleeding, referral to secondary care is recommended.