
Abstract
Chronic obstructive pulmonary disease (COPD) is a significant global health concern, contributing to morbidity and mortality. Keeping up to date with the advances in COPD management can enhance patient outcomes and is important for primary care clinicians. This review aims to examine current national and international guidelines, providing primary care clinicians with valuable insights into the evolving landscape of COPD management.
Clinical case scenario
You have a telephone appointment with John, a 60-year-old retired air steward with Chronic obstructive pulmonary disease (COPD). John has a 3-day history of cough productive of greenish sputum and a wheezy chest. John describes some shortness of breath on exertion and has needed to use a salbutamol inhaler more often than usual. Over the phone, John can speak in complete full sentences. John tells you a COVID 19 lateral flow diagnostic test was negative this morning and red flag symptoms for pulmonary embolism are ruled out. You decide to see John in clinic for a respiratory examination and this reveals the blood pressure of 135/80 mmHg, a regular pulse rate of 86/m, a temperature of 37.0°C, a respiratory rate of 20/m, and an oxygen saturation in room air of 92%, remaining so after exertion. Chest auscultation reveals scattered expiratory rhonchi, but no focal crackles.
You make a diagnosis of acute infective exacerbation of COPD and prescribe a 5-day course of doxycycline together with Prednisolone. Safety netting advice for worsening symptoms is given to either call the surgery back or the 111/out-of- hours provider.
Introduction
COPD is a lung condition characterised by chronic respiratory symptoms (dyspnoea, cough, sputum production) due to inflammation and narrowing of the airways (bronchitis) and/or alveoli (emphysema) that cause persistent, often progressive, airflow obstruction. COPD is the third leading cause of death globally and it is estimated there were 3 230 000 COPD-related deaths in 2019 worldwide (Global Initiative for Chronic Obstructive Lung Disease (GOLD), 2023). In the United Kingdom, approximately 1 200 000 adults live with diagnosed COPD, and a further 2 000 000 remain undiagnosed (National Institute for Health and Care Excellence (NICE), 2023).
COPD represents a considerable portion of the consultation time in General Practice, and poses a notable financial burden on the NHS. There are estimated to be an average of 1 400 000 consultations with GPs each year for patients because of COPD (NICE, 2015). The total estimated economic cost of COPD in the UK was about £9 billion in 2023, more than asthma (£6 billion) (Asthma and Lung UK, 2023).
The diagnosis of COPD should be considered in patients presenting with the cardinal symptoms of chronic cough (present for at least 3 months in two consecutive years), sputum production, dyspnoea and/or a history of exposure to risk factors (e.g. tobacco smoke, smoke from home cooking/heating fuels). Not all these symptoms are present in the early stages of the disease, and there may be individual variability as the disease progresses.
COPD should be suspected in current or ex-smokers presenting with recurrent ‘chest infections’ and this group should be considered for targeted case-finding with referral for spirometry. Services for delivery of primary care spirometry vary across the UK, but it should be performed and interpreted by appropriately trained professionals. To establish the diagnosis of COPD, a forced spirometry is necessary, with the presence of a post-bronchodilator FEV1/FVC ratio of less than 0.7. The focus of this article is the management of COPD rather than diagnosis; we will broadly divide COPD management into the treatment of acute exacerbations and management of patients with stable disease.
Management of acute exacerbations
Treatment of exacerbations of COPD (ECOPD) aims to provide relief from the negative impacts of the current exacerbation and prevent development of future events. Exacerbations are characterised by dyspnoea, cough, wheeze, and sputum production (which is often purulent). Clinicians should be aware of differential diagnoses of ECOPD, including pneumonia, COVID pneumonitis, heart failure and pulmonary embolism. Other causes of shortness of breath include pneumothorax (e.g. from bulla rupture), pleural effusion, acute coronary syndrome, cardiac arrhythmias (atrial fibrillation/flutter). Thorough history, examination, and use of ancillary investigations such as chest X-ray, COVID swab, electrocardiogram and B-type natriuretic peptide can help exclude other causes of these symptoms. Appropriate safety netting advice should be given, and prompt review should be arranged to assess patient’s improvement and guide decision making on further investigation.
Pharmacological treatment of ECOPD
Pharmacological treatment of exacerbations of ECOPD involves the use of short-acting beta agonists (SABA) and/or short-acting muscarinic antagonists (SAMA) administered through a metered-dose inhaler (MDI) device, preferably with a spacer. A nebuliser may be a more suitable option for severely ill patients though in the community or outpatient setting these are rarely recommended. Patients are generally advised to use their MDI inhaler with one or two puffs every hour for two or three doses initially, and then adjust to every 2–4 hours based on the patient’s response (GOLD, 2023). In the absence of contraindications, a short course of systemic corticosteroids is generally recommended during exacerbations. The usual treatment course is 30 mg prednisolone daily for 5 to 7 days.
Whilst various factors such as viral infections, air pollution, and smoking can trigger ECOPD, changes in sputum colour, volume, or thickness beyond the person’s usual day-to-day variation may indicate a need for antibiotics. If possible, the choice of antibiotic should be guided by the most recent sputum culture and sensitivities. In the absence of specific culture results, empirical treatment should be initiated, taking into consideration patient allergies and potential drug interactions. If symptoms do not improve after antibiotic treatment, it is appropriate to send a sputum sample for testing (NICE, 2018).
The Primary Care Respiratory Society (PCRS) has suggested a ‘pragmatic guide’ based on point of care testing for CRP (CRP-POCT) to determine the patient cohort that would benefit from antibiotic, thus reducing inappropriate antibiotic prescription (PCRS, 2022). Trials of CRP-POCT in the community are ongoing and not available in every area of the UK.
Emergency hospital admission should be considered if the patient’s condition deteriorates despite initial treatment of the exacerbation e.g. severe breathlessness, hypoxia (oxygen saturation SpO2 <90%), acute confusion or impaired consciousness, unfavourable psychosocial factors (e.g. patient lives alone, or inability to cope at home) or general decline, especially if there are significant comorbid conditions.
In patients with hypoxia, while arranging hospital transfer, give patients oxygen via a Venturi 24% mask at 2–3 L/min or Venturi 28% mask at a flow rate of 4 L/min or nasal cannula at a flow rate of 1–2 L/min (if a 24% mask is not available). The SpO2 target should be 88–92% in most cases.
Follow-up appointments should be arranged, especially for patients who have needed hospital management. This is usually within 1 to 4 weeks and 12 to 16 weeks after discharge. These aim of these appointments is to assess any changes in therapy, patients’ understanding and compliance and to evaluate patients’ psychosocial state and inhaler technique (Bollmeier and Hartmann, 2020). In many practices, a structured post discharge COPD review is carried out by a member of the practice nursing team with additional training in respiratory monitoring.
Management of chronic stable COPD
Management incorporates non-pharmacological and pharmacological methods. We will first discuss non-pharmacological treatment, the bedrock of good COPD care (International Primary Care Respiratory Group (IPCRG) 2016). We will then review pharmacological management.
Non pharmacological management
Smoking cessation
Smoking reduces pulmonary function, due to alterations in resistance to airflow, cough, and irritation of the airway. Smoking cessation is the only effective treatment to avoid or reduce progression of this disease. Studies have shown that many smokers want to stop smoking, but a significant proportion have never tried or are contemplating smoking cessation. Most smokers make several attempts at cessation before succeeding (Laniado-Laborín, 2009). Therefore, it is important to counsel smokers during each interaction, emphasising the overall health benefits of quitting smoking.
NICE recommends the use of very brief advice (VBA+) on smoking cessation in primary care, which includes the following 3As:
Establishing smoking status [ASK] Providing advice on the best ways to quit smoking [ADVISE] Offering additional support options and access to stop-smoking medications [ACT]
NICE also recommends behavioural support from trained counsellors to provide stop-smoking assistance. This is usually provided in conjunction with stop-smoking pharmacotherapies (NICE, 2021). NICE are broadly supportive of the use of e-cigarettes as part of a smoking cessation plan. Pharmacotherapies licensed in the UK to support smokers include nicotine replacement therapy (NRT), bupropion, and varenicline. The latter two are usually started by the smoking cessation service.
NRT should be explained to patients in terms of its safety compared with cigarette smoking. NRT aims to replace the addictive substance, nicotine, found in cigarettes while avoiding the other toxic components like carbon monoxide, tar, and chemicals such as benzene, arsenic, and formaldehyde. NRT is available in different forms, both short-acting and long-acting. Combining both forms is considered to increase the chances of successful smoking cessation. Nicotine patches provide a slow, steady level of nicotine over an extended period. Short-acting NRT options include sublingual tablets, lozenges, gum, nasal spray, and inhalators. The choice depends on the patient’s preference and the effectiveness of the chosen method. A quit date should be agreed upon and NRT should be available for the patient to start using the day before the quit date. Bupropion is a Serotonin and noradrenaline reuptake inhibitor (SNRI) which is licensed in the UK as an adjunct to smoking cessation. Buproprion is used in other countries as an antidepressant, but does not have a UK licence for this use. Any patients concomitantly taking a SSRI or SNRI should be counselled about the risk of serotonergic side effects or serotonin syndrome. If abstinence is not achieved at 7 weeks, the drug should be stopped. Varenicline is a selective nicotine-receptor partial agonist it is prescribed as a 12-week course. Both drugs should be prescribed to start 1 to 2 weeks before the set quit date.
Vaccination
Vaccines are known to offer effective preventive benefits to reduce the frequency, as well as severity, of respiratory infections and exacerbations in COPD patients. COPD patients should be offered the following:
Influenza vaccine annually Pneumococcal polysaccharide vaccine (PPV23), as a single one-off dose except in cases of other comorbidities such as asplenia, splenic dysfunction, or chronic renal disease, where vaccination every 5 years may be required COVID-19 vaccination (primary and booster doses) in accordance with national recommendations
Pulmonary rehabilitation
Pulmonary rehabilitation (PR) incorporates an evidence-based exercise and education programme designed for patients who continue to experience symptoms of breathlessness; this includes patients with stable COPD as well as patients experiencing symptoms immediately after COPD exacerbation. Sessions are usually held in groups. PR involves a comprehensive individually prescribed programme including aerobic exercise, resistance training and lifestyle support. The programme typically lasts 6 to 8 weeks with two sessions of around 2 hours each week. It is supported by trained healthcare professionals such as physiotherapists, nurses, and occupational therapists.
Although pulmonary rehabilitation is a very effective option for many patients, it is not appropriate for all patients e.g. late-stage cancer, unstable cardiovascular diseases, severe dementia or patients having had a pneumothorax in the last 6 weeks. Logistical problems such as transport facilities, cost for the patient, and distance from the rehabilitation centre should all be factored in before referral. Tele-rehabilitation, where available, is an evolving option for patients unable to attend treatment sessions in-person.
Pharmacological management
The use of medication in the management of stable COPD helps reduce symptoms and exacerbation frequency and improve patients’ exercise tolerance and ability to carry out activities of daily living. Available modes of administration of these medications include inhaled (mainstay), nebulised, and oral therapies.
Inhaled therapy
Inhaled therapy forms the primary therapeutic approach in COPD, consisting of short-acting bronchodilators and long-acting bronchodilators, with or without inhaled corticosteroids (ICS). SABA and SAMA, administered in inhaled form, are the initial treatment options for providing relief from dyspnoea and improving exercise tolerance as needed. These inhalers are also known as ‘relievers’.
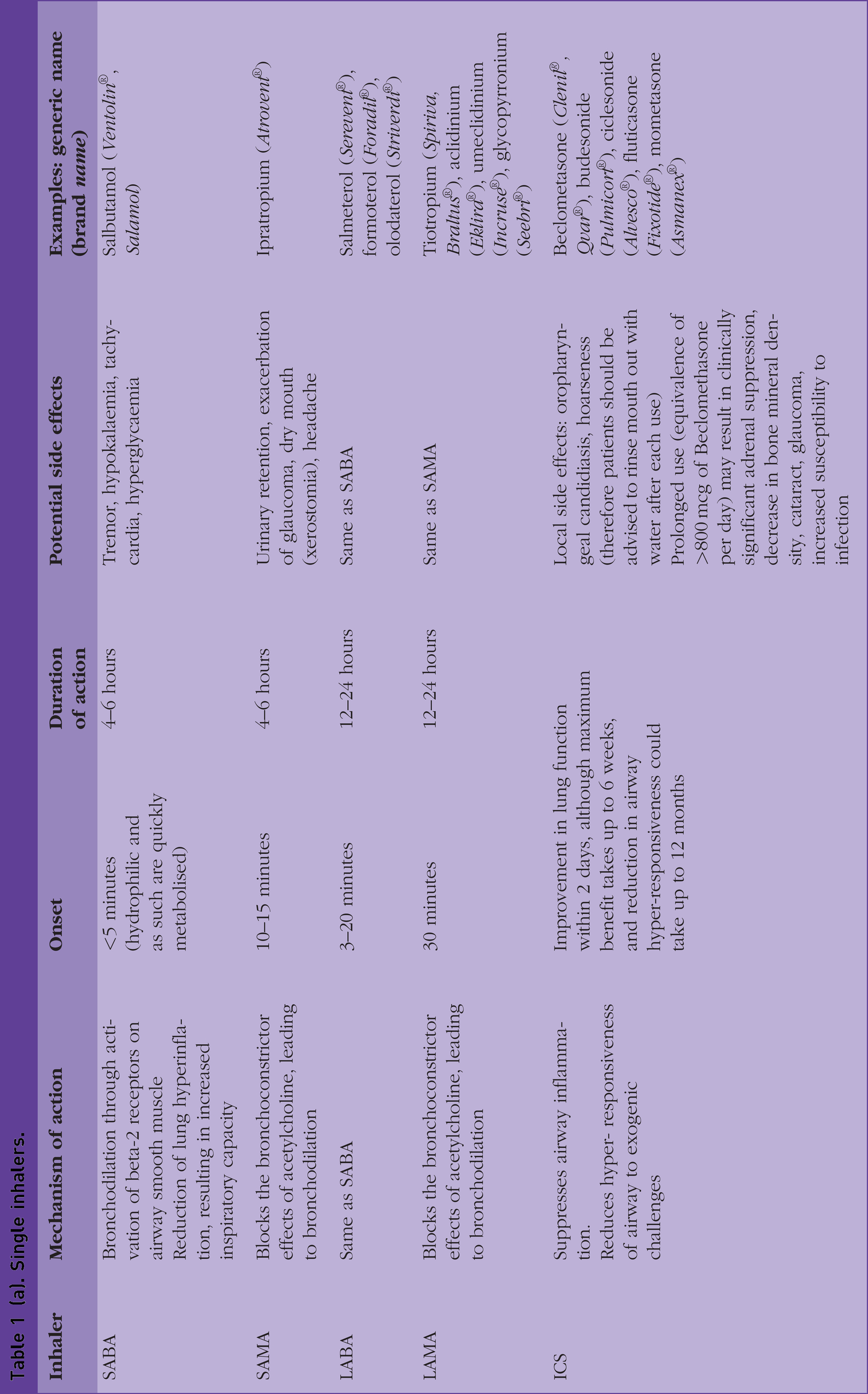
NICE recommends that if patients continue to experience symptoms, combination inhalers should be added depending on the presence of asthmatic features or features suggesting responsiveness to steroids. The flowchart in Fig. 1 shows stepwise management and escalation of inhaler therapy. Also, Tables 1(a) and 1(b) highlight pharmacological actions, potential side effects and examples of these inhalers.
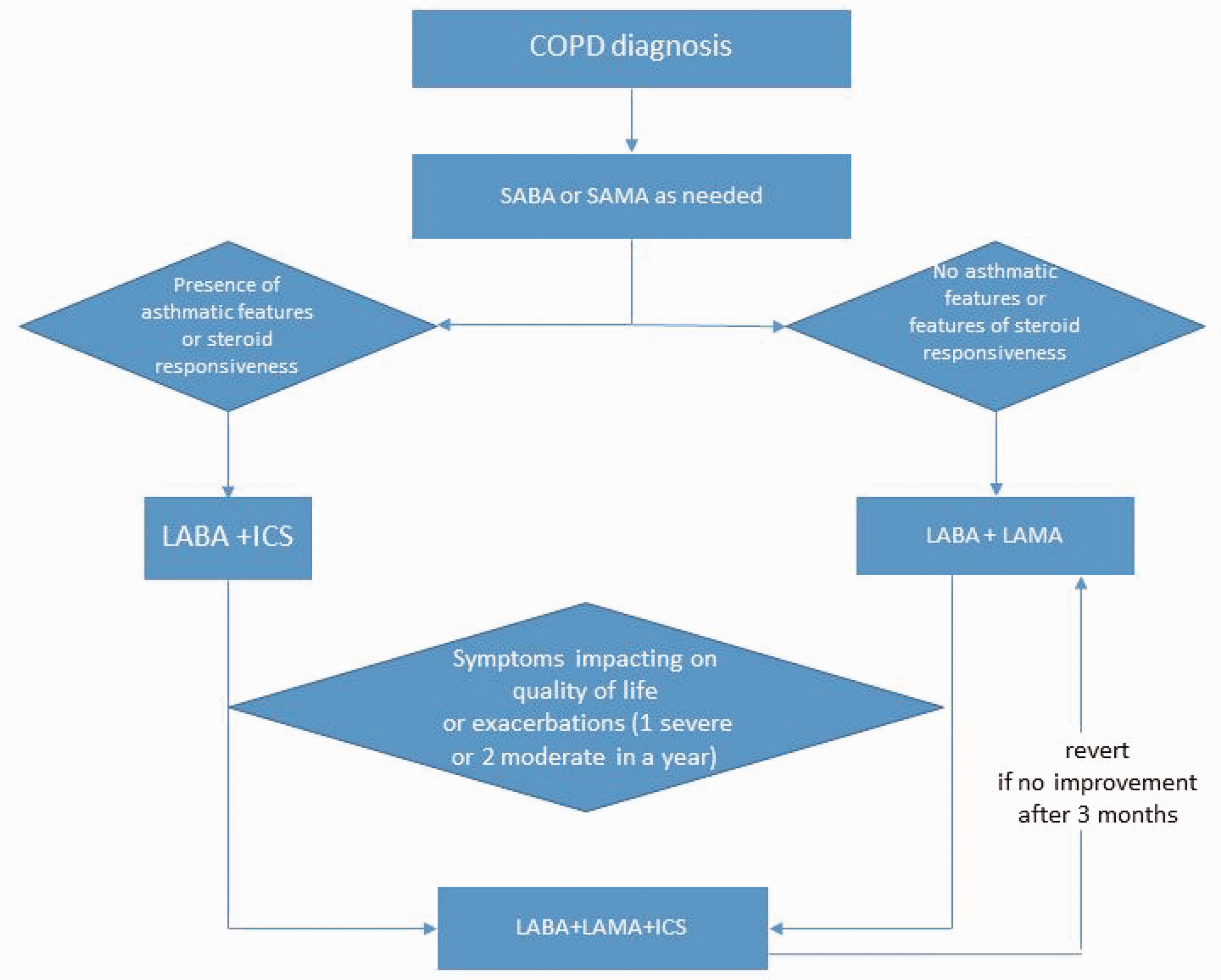
Flowchart showing escalation of inhaled therapy in COPD.
(a). Single inhalers.
(b). Combined inhalers.

It is worth noting the major difference between NICE 2018 and GOLD 2023 guidelines in the management of COPD. GOLD 2023 divides patients into three groups based on symptom burden (primarily breathlessness) and history of exacerbations (as a predictor of future risk of exacerbation) (see Table 2). The use of LABA + ICS is discouraged by GOLD; if ICS is indicated (i.e. asthmatic features or eosinophil >300), then patients should be prescribed LABA + LAMA + ICS, which has been shown to be superior.
GOLD 2023 COPD severity (based on symptoms and exacerbations) and suggested initial treatment.

It is known that patients with blood eosinophil counts of less than 100 cells/µL are unlikely to benefit from ICS, and may be at risk of harm from ICS side effects. The patients most likely to benefit from ICS therapy are those with: a blood eosinophil count exceeding 300 cells/µL; a history of hospitalisation for COPD exacerbations; two or more moderate exacerbations per year or a history of concurrent asthma (PCRS, 2023).
It is essential to consider that ICS use carries potential risks, including an increased risk of pneumonia, mycobacterial infection, oral candidiasis, and bruising. Furthermore, long-term use of ICS exposes patients to the risk of osteoporosis, diabetes, and cataracts. Therefore, these factors should be carefully evaluated before initiating patients on ICS.
Delivery systems
Inhalers
There are different forms, which include pressurised metered dose inhalers, used with or without spacer/valved holding chamber; breath-actuated MDIs, soft mist inhalers and dry powder inhalers (DPIs). A visual guide of inhalers can be accessed through this link: www.mims.co.uk/respiratory-visual-guide.
Choice of inhaler device should be guided by the patient’s preference and ability to grasp inhaler technique. Right Breathe is a good internet resource with videos for inhaler technique (www.rightbreathe.com). Where possible, use the minimal number of devices for inhaler therapy e.g. dual LABA + LAMA, triple LABA + LAMA + ICS inhalers (see Table 1(b)). Patients should have their inhaler technique checked when started on a new device. This is usually the remit of the community pharmacist dispensing the item. It is considered good practice for inhaler technique to be reviewed when patients are seen for their annual practice-based COPD review.
Prescribers should be aware of ‘greener prescribing’ aimed at reducing carbon footprint. The propellant gas in MDIs used to contain CFCs (chlorofluorocarbons). However, the shift is now to use an HFA (hydrofluoroalkane) propellant as this is more environmentally friendly. Wherever possible, patients should be started on DPIs as they have the lowest carbon footprint.
Nebuliser
Consider nebulisers in patients with distressing or disabling breathlessness despite maximal therapy using inhalers. Patients who have cognitive, neuromuscular, or ventilatory impairments, and those with suboptimal peak inspiratory flow (required to overcome the internal resistance of DPIs) may not derive full benefit from handheld inhalers.
Albeit anecdotal, use of nebulisers carries risks (e.g. failing to take corticosteroids, failing to call for medical help, microbial contamination, and potential autoinfection with inappropriate nebuliser use) and benefits (e.g. improved patient confidence or reduced hospital admissions). These risks vs benefits have not been confirmed in large studies. Therefore, use of a nebuliser should be in accordance with a self-management plan agreed with an appropriate specialist. Patients should have easy access to service their nebulisers as well as ongoing advice and support.
Oral therapies
Oral therapies, as add-on treatment in COPD, are usually initiated after respiratory specialist assessment with continued prescription in primary care. Antibiotic prophylaxis with azithromycin (250 mg three times a week as off-label licence) could be considered in patients prone to exacerbations (four or more in a year), prolonged exacerbations with sputum production and exacerbations resulting in hospitalisation. Patients should already have optimised non-pharmacological management and inhaled therapies.
Oral corticosteroid use for daily long-term management of COPD is discouraged, due to systemic side effects. There may patients in whom it is difficult to stop oral corticosteroid completely after an exacerbation; such patients should be referred for specialist review. If long-term low-dose steroids are considered, then bone protection must be considered as well as protection with a proton pump inhibitor.
Mucolytics, e.g. carbocisteine work by reducing the viscosity of sputum. Studies suggest that they have limited impact on lung function or health-related quality of life. There is a role for mucolytics in management of exacerbations, as they ease expectoration and reduce frequency of cough and patients may find they are symptomatically better when taking these drugs. There is no clear evidence of a difference between mucolytics and placebo on mortality (Poole et al., 2019).
Oral theophylline works by relaxing the smooth muscles located in the bronchial airways and pulmonary blood vessels. It is also known to reduce the airway responsiveness to histamine, methacholine, adenosine, and allergens. Its use is limited by the need for baseline bloods before initiation and monitoring of serum levels. Prescribers should be aware of the potential interaction with liver enzyme-inducing and inhibiting drugs, as the dose of theophylline might need to be adjusted accordingly during concomitant use, and drug levels will need to be monitored. Moreover, if patients start or stop smoking, a dose adjustment may be needed because tobacco, which is a hepatic enzyme inductor, can lower the plasma levels of theophylline.
The COPD review in primary care
It is important to highlight the role of multidisciplinary teams in the management of COPD in the community. Some practices have a respiratory lead GP, practice nurses or clinical pharmacists to undertake annual reviews for continuity of care. This ensures a bridge between primary and secondary care, with primary care serving as a ‘gatekeeper’ to keep frequently exacerbating patients out of hospital. Although area dependent, there are integrated community respiratory teams offering access points for pulmonary rehabilitation, support for patients on oxygen, etc.
Frequency of follow up depends on the stage of disease: at least annual review for patients with mild/moderate/severe COPD, and at least twice a year in very severe COPD (NICE 2018).
The key components at each review are:
Assessment of severity, risk of exacerbations and impact of the disease Reinforcement of smoking cessation advice Step-up of management in response to increasing need Review of self-management advice Identification of comorbidities, and their appropriate reviews.
Degree of dyspnoea should be measured using the modified (Medical Research Council (MRC)) dyspnoea scale (see Table 3). It is a validated and widely used method and correlates with other measures of disability such as exercise tests, quality of life, and activities of daily living.
Modified MRC dyspnoea scale.
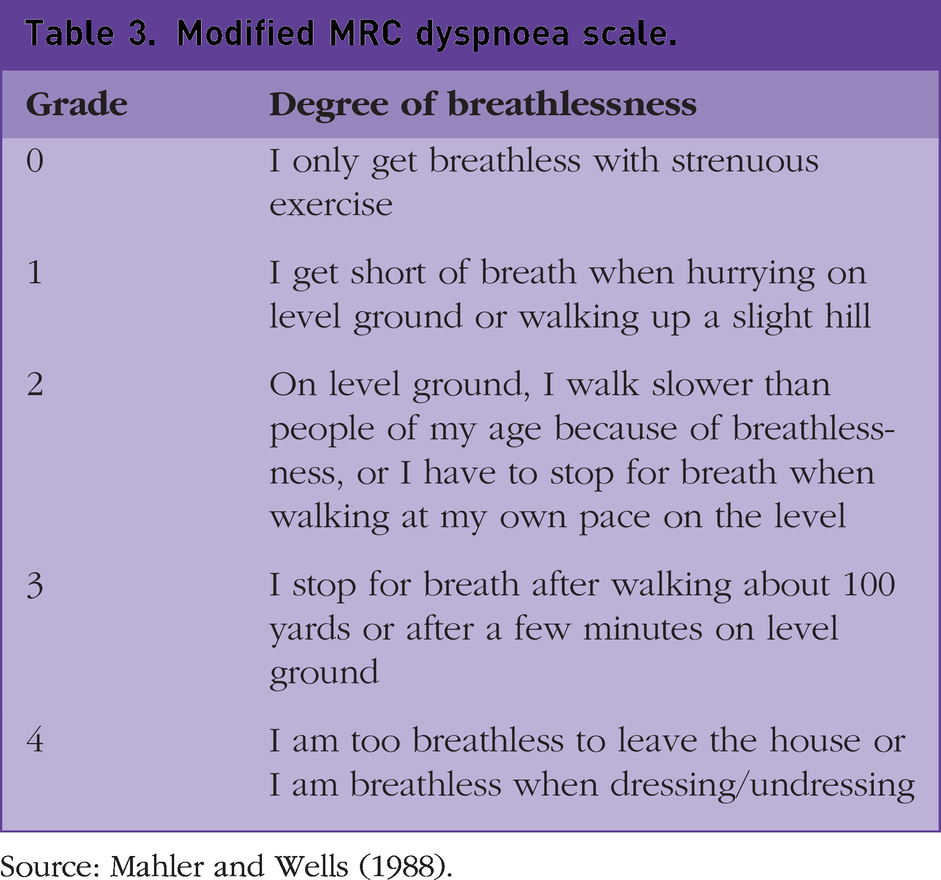
Source: Mahler and Wells (1988).
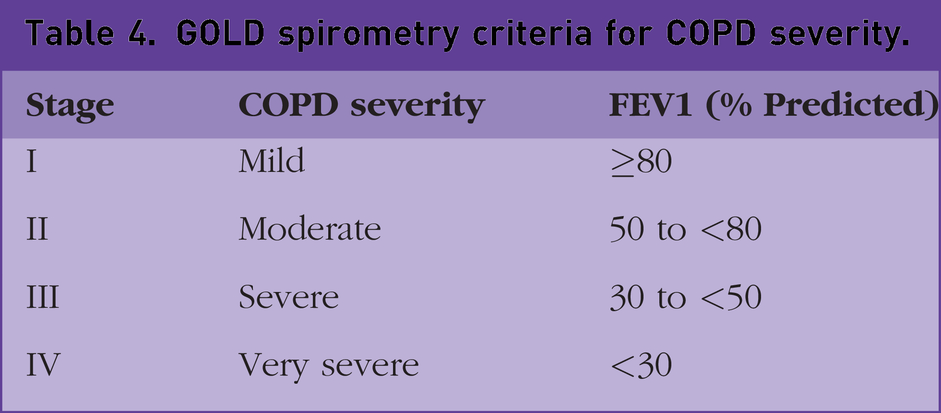
NICE advises checking lung function (FEV1 and FVC) at every COPD review. This would guide staging of severity as demonstrated in Table 4, which would inform the need for further assessment.
GOLD spirometry criteria for COPD severity.
Before each review, patients should be encouraged to complete self-reported outcome measures using questionnaires such as the COPD Assessment Tool (CAT). This provides a measure of health status and symptom burden. Patients’ clinic notes should be reviewed to assess frequency of exacerbations requiring antibiotics and/or oral steroid courses. This should guide assessment of future risk and further evidence of the impact of the disease.
Inhaler technique should be checked using an inspiratory flow meter (e.g. Incheck dial) which is able to simulate the resistance characteristics of different inhalers and, thereby, guide the patient to the correct effort needed; or ‘Teach back’ approach. Patients on ICS that have not experienced an exacerbation in the past year could be considered for dose reduction of inhaler.
COPD self-management
COPD, like every chronic disease, is better managed when the patient can participate in shared decision making regarding their condition. Self-management is based on the premise that the doctor/healthcare professional is an expert in healthcare whereas the patient is an expert in him/herself, and both need to work together for the best possible outcome.
Rescue pack
The use of rescue packs plays a role in patients at risk of frequent exacerbations (two or more in a year). This forms part of a self-management plan, which when used appropriately, with sufficient patient education, could reduce the rate of hospitalisation on account of COPD exacerbations, although evidence for this remains sparse. Antibiotics and steroids are prescribed to be taken in the following instances (Box 1):
Antibiotic: When sputum becomes coloured, purulent or change in the volume COPD rescue pack. COPD patients at risk of having an exacerbation should be given a course of antibiotic and corticosteroid tablets to keep at home for use as part of a self-management strategy. These may be: • Prednisolone 30 mg once daily for 5–7 days • Empirical antibiotic (or based on last sputum culture result): ▪ Amoxicillin 500 mg three times daily for 5 days ▪ Doxycycline 200 mg first day then 100 mg daily for total 5-day course ▪ Clarithromycin 500 mg twice daily for 5 days Steroid: When patient feels more wheezy or short of breath
Use of rescue packs comes with limitations, as it depends on patient’s ability to identify an exacerbation. Also, there is the risk of COPD symptoms masking other conditions. Therefore, the patient should be educated (and their understanding checked) on symptoms to look out for and red flags discussed. Also, patients should be advised that they must contact their healthcare professional if they have started the rescue pack to alert them that they have become unwell.
Patients should be advised that inappropriate and overuse of steroids is linked with adrenal suppression, osteoporotic fractures, diabetes, pneumonia, psychosis, thinning skin and cataracts, and overuse of antibiotics (or not taking them for the full course) risks antimicrobial resistance, both in the individual patient and in our society.
Managing mental health
Estimates suggest that about 30% of people with COPD have comorbid depression (increasing to up to 80% with increasing COPD severity), and between 10% and 50% have comorbid anxiety (IPCRG, 2022). It is important that patients are asked about their mental health and encouraged to seek psychological support when needed. COPD patients should be considered for referral to support groups (e.g. Breathe Easy support groups) offering learning opportunities and opportunities to make new friends, adapt to the condition and engage in self-management.
Supplemental oxygen therapy
Many patients with COPD are significantly breathless without necessarily being hypoxic. Normally, the body is very sensitive to the partial pressure of carbon dioxide (PaCO2), and as this increases, ventilation increases. COPD patients will often have a higher PaCO2 due to impaired ventilation, thus blunting the CO2 - driven ventilation. The physiologic ‘backup mechanism’ is hypoxia – mild hypoxia is not a potent respiratory stimulant, but increasing hypoxia drives respiration. By giving supplemental oxygen to COPD patients, their hypoxic drive is removed causing them to profoundly under-ventilate leading to potentially fatal CO2 narcosis.
Long-term oxygen therapy
Long-term oxygen therapy (LTOT) has been shown to improve survival when used for at least 15 hours per day. Patients should have optimum medical management and stable disease. The criteria for LTOT are highlighted in Box 2. LTOT criteria. When to consider LTOT: • Chronic hypoxemia SpO2 <92% (measured on two occasions at least 3 weeks apart and at least 5 to 6 weeks after an exacerbation) • PaO2 <7.3 kPa (8 kPa in patients with pulmonary hypertension, secondary polycythaemia, peripheral oedema from cor pulmonale)
Like any other drug, to ensure safe prescribing of oxygen, the following issues need to be considered carefully:
The presence of cognitive impairment A current smoker or patient who lives with someone who smokes pose a fire hazard A history of falls (as there is a risk of tripping over the equipment and if the patient is on anticoagulation, this increases the risk of bleeding following a fall)
Ambulatory oxygen
Ambulatory oxygen is aimed at improving exercise tolerance. It is recommended for patients already on LTOT wishing to use oxygen outside the home, those who have exercise desaturation (SpO2 drop of >4% on exertion resulting in <90% saturation) and are shown to have an improvement in exercise capacity with oxygen and have the motivation to use oxygen.
Short-burst oxygen therapy
Short-burst oxygen therapy (SBOT) is intermittent use of supplemental oxygen at home, usually for periods of about 10 to 20 minutes at a time to relieve dyspnoea. SBOT has traditionally been widely used for pre-oxygenation before exercise, to relieve breathlessness during recovery from exercise, to control breathlessness at rest, in palliative care and after an exacerbation of COPD to bridge the time to full LTOT assessment. SBOT should not be prescribed to manage breathlessness in people with COPD and mild or no hypoxaemia at rest.
Non-invasive ventilation
Non-invasive ventilation (NIV) is used acutely in patients who have acidotic exacerbation of COPD and could be used as an initial bridge to intubation and ventilation if patients deteriorate.
Home NIV could be considered in patients that are adequately treated, but have chronic hypercapnic respiratory failure and have needed assisted ventilation (whether invasive or non-invasive) during an exacerbation, or who are hypercapnic or acidotic on long-term oxygen therapy. This will be initiated by the respiratory specialist team. Many NIV devices are designed such that parameters could be monitored remotely by the respiratory physiology units. Recent evidence has shown home NIV compared with standard treatment improves survival of patients with hypercapnic, stable COPD when NIV is targeted to greatly reduce hypercapnia (Duiverman, 2018).
Surgical therapy
Current surgical treatments include bullectomy, lung volume reduction surgery and lung transplantation. These surgical approaches are used only rarely with specific criteria for eligibility. COPD accounted for 25% of primary disease indication on the adult lung transplant list, and 27% of adult lung transplants carried out in the UK between 2021 and 2022 (NHS Blood and Transplant 2022).
Future/trial therapies
Management of COPD holds a promising future in tackling this highly significant disease. These therapies include:
Use of monoclonal antibodies (mepolizumab) and anti-interleukin 5 receptor alpha antibody (benralizumab) in patients with eosinophilic phenotype of COPD and who require frequent oral corticosteroids use for exacerbations Digital health and self-management apps: Their use has very promising outcome, including improved patients’ inhaler technique, CAT score, and providing patients the knowledge and confidence for effective and safe self-management
Palliative care
COPD is a progressive life-limiting condition. All patients with end stage COPD should have open discussions about prognosis and issues such as advance directives covering their wishes about admission to hospital, ventilation and resuscitation in the event of cardiorespiratory arrest. It is important to identify such patients using tools such as The Gold Standards Framework Proactive Identification Guidance and add patients to the practice’s palliative care register. Opiates at low dose (e.g. liquid morphine sulphate 2.5–5.0 mg orally every 2–4 hours) and fans blowing air onto the face can relieve breathlessness. Anxiety and panic attacks are common at this stage and can be reduced by pharmacotherapy (e.g. Lorazepam sublingual) as well as cognitive behavioural therapy and mind−body interventions (e.g. mindfulness-based therapy, yoga).
Referral to the local hospice, where available, for specialist palliative care can help management of difficult to control symptoms and provide patients and their families with support during end of life care. Many hospices run Fatigue, Anxiety and Breathlessness (FAB) Programmes which to help patients cope with some of the symptoms and improve quality of life.
Key points
COPD continues to be a leading cause of morbidity and mortality globally
Smoking cessation should be offered at every contact
GP should be aware of the pharmacological and non-pharmacological treatments available in the management of COPD
Shared decision making and self-management are essential for optimal management
Compassionate palliative care should be a part of managing end-stage COPD