
Abstract
Blistering skin conditions encompass a broad spectrum of disorders, ranging from life-threatening emergencies requiring immediate attention to chronic conditions needing secondary care referral. There are also more simple conditions that can be managed with self-care or over-the-counter medication.
Clinical case scenario
A 75-year-old woman presents with a 2-week history of a generalised skin rash characterised by erythematous macules, papules, and large, tense bullae filled with clear fluid. The rash initially started on her abdomen and thighs, but has since spread to her arms, legs, and back. She complains of severe itching over the affected areas, disrupting her sleep. There are no systemic symptoms, and her vital signs are stable. On examination, multiple bullae with erosions and a characteristic ‘rosette’ appearance are observed. The oral cavity appears normal. Mrs Smith has no recent changes in medication or any over-the-counter medication.
What other history you would like to ask about? What examination will you do? Are there any investigations that need doing? How will you manage this patient?
Introduction
The aim of this article is to provide a comprehensive understanding of blistering skin conditions and a general diagnostic framework. This framework includes important aspects of the history and clinical examination to formulate a diagnosis or narrow the possibilities in differential diagnosis. For the purpose of this article, blistering skin conditions are broadly categorised into three groups:
Life-threatening emergencies demanding immediate emergency admission and prompt intervention. Acute blistering skin conditions commonly encountered in day-to-day primary care practice, often easily managed effectively in primary care. Chronic conditions requiring referral for further management in secondary care
It is important in primary care to remain vigilant when assessing skin conditions, as they present with overlapping signs that mimic the symptoms of various other illnesses. This underscores the need for thorough evaluation and differential diagnosis. A comprehensive understanding of the patient’s medical history, symptoms, and possible underlying conditions is essential for accurate diagnosis and an appropriate management plan.
Definitions
Blisters, vesicles, and pustules are distinct types of skin lesions characterised by their size, contents, and underlying causes (Fig. 1).

Blister on medial foot caused by wearing thongs/flip flops.
Blisters
Blisters are small-to-large fluid-filled sacs that form within the upper layers of the skin. They typically arise due to friction, burns, or irritants. Blisters can contain clear fluid, blood, or pus and can provide protective cushioning to the skin during the healing process.
Vesicles
Vesicles are smaller counterparts to blisters, usually measuring less than 5 mm in diameter. They contain clear fluid and are often caused by irritation, injury, or infection. Vesicles are commonly associated with conditions such as chickenpox or herpes simplex infections.
Pustules
Pustules, unlike blisters and vesicles, are characterised by inflammation and the presence of pus. These lesions appear as small, elevated bumps on the skin’s surface and are typically tender or painful to the touch. Pustules commonly occur in inflammatory skin conditions such as acne or folliculitis, where bacteria or other pathogens infect the hair follicles.
Diagnostic work up
As in other dermatological conditions, it is vital to get an accurate and detailed clinical history and to perform a thorough examination. When gathering a medical history, it is crucial to determine if the rash appeared suddenly or developed gradually, and to understand the duration and progression of symptoms. It is important to identify any triggers or factors worsening the rash, and whether this is the first occurrence or a recurring issue. Ask also about associated symptoms such as pain, itching, and oozing. Obtain a comprehensive medical history, paying special attention to recent medications, travel history, and any contact with specific substances or environments.
A thorough skin examination is necessary to document the location, distribution, and characteristics of the rash, including an inspection of mucous membranes. Detailed assessment of blisters involves evaluating their size, shape, and arrangement - whether singular or multiple, clustered or dispersed. By palpating the blisters, their tension can be determined, along with observing the colour and clarity of the fluid inside. Special signs such as the Nikolsky sign may indicate autoimmune blistering disorders. Vital signs and more general systemic examination should be conducted as appropriate.
It is unlikely that investigations are necessary in primary care. If a condition requiring investigation is suspected, referral is usually required. The urgency of this depends on the clinical assessment.
Differential diagnosis
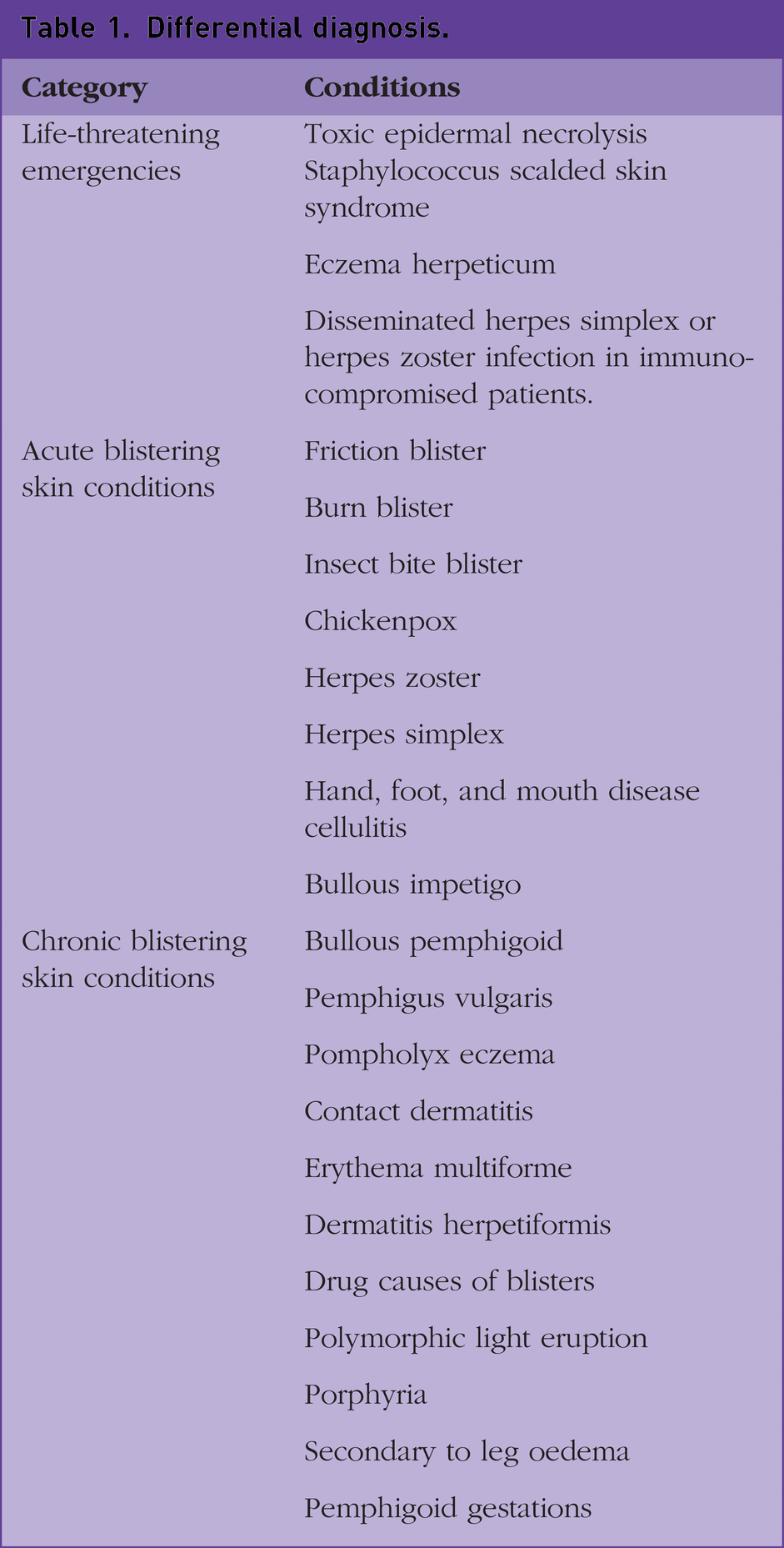
Blistering skin conditions include a spectrum of disorders, ranging from acute to chronic and potentially life-threatening emergencies. Such emergencies include toxic epidermal necrolysis and staphylococcus scalded skin syndrome and these demand urgent medical attention. Acute clinical scenarios often involve everyday occurrences such as friction or burn blisters and viral infections including chickenpox and herpes zoster. Chronic disorders include autoimmune conditions such as bullous pemphigoid and pemphigus vulgaris, as well as contact dermatitis. Each disorder necessitates a distinct management strategy according to the underlying cause and this requires accurate diagnosis and prompt intervention (Table 1).
Differential diagnosis.
Life-threatening emergencies
Several blistering disorders are potentially life-threatening emergencies and need early diagnosis and prompt management. These include:
Toxic epidermal necrolysis
Toxic epidermal necrolysis (TEN) is a rare, life-threatening skin condition that can be caused by an inappropriate immune reaction to certain drugs, infections, vaccines, or even spontaneously. It is characterised by the detachment of the epidermis from the underlying dermis, resulting in widespread blistering and peeling of the skin. The mortality rate of TEN is high, at approximately 30% (Labib and Milroy, 2023).
It typically starts with flu-like symptoms, such as fever, cough, and body aches, followed by the appearance of painful red or purple skin lesions. As the condition progresses, these lesions rapidly spread and merge, causing large areas of the skin to detach from the body, resembling severe burns in appearance. This phenomenon is nicknamed ‘skin burn-like’ appearance. Other signs include blistering, sloughing of the skin, and mucous membrane involvement, affecting the eyes, mouth, and genital regions.
The main treatment for TEN is supportive care. This includes fluid resuscitation, pain management, wound care, and nutritional support. In some cases, corticosteroids or immunosuppressant medications may be used to suppress the immune system and help to reduce the severity of the condition.
Staphylococcal scalded skin syndrome
Staphylococcal scalded skin syndrome (SSSS) is a serious and potentially life-threatening skin condition caused by a Staphylococcus aureus bacterial infection. It primarily affects infants and young children, but can also occur in immunosuppressed adults.
The syndrome is characterised by the appearance of large, painful blisters and widespread peeling of the skin, giving the impression of scalded skin.
The exfoliative toxins produced by the S.aureus bacteria are responsible for causing the separation of the outermost layer of the skin from the underlying layers, leading to blistering and skin detachment.
The initial event in SSSS is often a localised S. aureus infection of the skin or upper respiratory tract, which often goes unnoticed. This is followed by fever, irritability, and non-tender skin. Macular erythema then develops into diffuse, confluent erythema with bullae. The bullae rupture easily, leading to marked epidermal exfoliation. The skin peels off in sheets, leaving exposed moist, bright-red, tender areas. The Nikolsky sign is positive. A positive Nikolsky sign is a clinical indication where slight rubbing of the skin causes the top layer to peel away easily.
Prompt diagnosis and emergency hospitalisation for supportive care and antibiotic treatment is required. With timely and appropriate medical intervention, the prognosis for most patients with SSSS is favourable.
Eczema herpeticum
Eczema herpeticum (EH) is a disseminated cutaneous infection with herpes simplex virus that develops in a patient with atopic dermatitis. EH typically presents as a sudden eruption of monomorphic vesicles and ‘punched-out’ erosions with hemorrhagic crusts over eczematous areas.
Patients may have systemic symptoms, such as fever, lymphadenopathy, or malaise. Referral for systemic antiviral drugs and supportive therapy is required.
Acute blistering skin conditions
Friction blister
Blisters caused by skin friction are a common and painful skin condition. They typically result from repetitive rubbing or pressure on the skin (Fig. 2).

Friction blisters due to running barefoot.
The primary symptoms of friction blisters are painful redness of the affected area followed by blister formation. In some cases, the blister may burst, leaving an open sore that can be susceptible to infection.
Most friction blisters heal spontaneously without complications. In general, patients should be advised to keep the area clean and dry, avoid further friction, and protect the blister with a sterile dressing or bandage as required.
In some cases, where the blister is large it can be drained by pricking with a sterile needle. Infected friction blisters or erosions may require topical antibiotics or antiseptics for a few days. Systemic antibiotics must be used if cellulitis occurs. Antibiotics should not be used if the wound is not infected.
Burn blister
When the skin is exposed to intense heat or cold, it can lead to thermal injury, resulting in blister formation. Blisters occur in superficial and deep dermal (partial thickness) burns. The general principles that underpin burn management apply and includes proper assessment to classify the degree of burn and any possible complication, analgesia and further management as appropriate.
Insect bite blister
Insect bites are common in the UK. It is more common in the summer months and personal factors increase the likeness of exposure to insect bites such as occupation (beekeeping or forestry work associated with bites from ticks or midges) and a wide variety of recreational outdoor activities.
The affected area typically becomes red, swollen, and itchy, followed by the formation of small fluid-filled blisters. These blisters can be painful. Individuals may also experience other symptoms such as localised warmth and tenderness around the bite site.
The management of insect bites needs careful assessment of the patient’s allergy history and medical history looking for any condition or drug that can affect the immune system. Management in primary care includes considering tetanus prophylaxis, quickly removing visible stingers or ticks, using analgesia appropriately and advising the patient about good hygiene practices to prevent secondary infections.
The National Institute for Health and Care Excellence (NICE) recommend that we do not routinely offer antimicrobial prophylaxis or carry out serological tests for Lyme disease (NICE, 2023a). If a rash appears at the site of the bite (erythema migrans) or a fever develops, then prompt medical advice should be sought and guidance followed on further management and treatment.
Chickenpox
Chickenpox is a common viral infection caused by the varicella-zoster virus.
In the UK, roughly 90% of adults are estimated to have immunity to chickenpox (NICE, 2023b).
The virus spreads through respiratory droplets or direct contact with the fluid from the characteristic blisters that form during the illness. Symptoms typically include fever, headache, and tiredness, followed by the development of a rash progressing into itchy blisters.
Treatment mainly focuses on symptomatic relief; encouraging adequate fluid intake, analgesia for pain and fever, topical calamine lotion and antihistamines to alleviate pruritus. Consider prescribing oral aciclovir 800 mg five times a day for 7 days for immunocompetent, non-pregnant adults or adolescents (aged 14 years or older) with chickenpox presenting within 24 hours of the rash onset. This prescription is also appropriate for severe chickenpox or those at increased risk of complications, such as smokers. Vaccination is available on the NHS, and is particularly recommended for high-risk individuals. Vaccination provides effective protection against the disease.
Herpes zoster
Herpes zoster, commonly known as shingles, is a viral infection caused by the reactivation of the varicella-zoster virus, the same virus responsible for chickenpox. The main symptom of herpes zoster is a painful rash typically appearing as a band or stripe in a dermatomal distribution, most commonly on the trunk or face. The rash is characterised by fluid-filled blisters that can break open and crust over. Other symptoms include fever, headache, and general malaise. The most distinctive sign of herpes zoster is the painful rash and its unilateral distribution. Management of the condition involves antiviral medication, pain relief, and sometimes topical treatments for the rash. Early treatment is essential to reduce the severity and duration of the infection and to prevent potential complications, such as postherpetic neuralgia (PN). PN is pain persisting after the rash has healed. Vaccination is now available to prevent the occurrence of shingles according to the NHS vaccination schedule.
Herpes simplex
Herpes simplex infection is a common viral disease in humans caused by the herpes simplex virus (HSV). In the UK, it is estimated that a significant proportion of the population has been exposed to HSV, with prevalence rates varying by age and region. The infection can manifest as oral, ocular and genital.
Ocular herpes, predominantly caused by HSV type 1 (HSV-1) and occasionally by HSV type 2 (HSV-2), is often associated with orogenital sex. Patients typically exhibit general symptoms such as fever, malaise, and fatigue. Specific symptoms include eye pain, irritation, photophobia, and eye watering, which may indicate keratitis. Signs of infection include an acute red eye, clusters of vesicles and ulcers on a red base, or pustules along the lid margin or periocular skin, which eventually crust over. Additional signs include a fixed irregular pupil and reduced visual acuity. Suspected cases of ocular herpes simplex infection should be referred to eye casualty or an emergency eye service for same-day assessment and specialist management. Drug treatment should not be initiated while awaiting specialist ophthalmology assessment.
Oral herpes, primarily caused by herpes simplex virus type 1 (HSV-1), is transmitted through direct contact such as kissing or sharing utensils or towels. Symptoms include painful blisters or sores in areas such as the mouth, lips, or genital region. Patients may also experience fever, headache, and malaise during outbreaks. Symptoms typically begin with a prodrome of pain, burning, tingling, itching, and paraesthesia lasting 6–48 hours, followed by the development of vesicles, which ulcerate, usually at the mucocutaneous junction of the lips.
Management of uncomplicated herpes infection focuses primarily on providing symptomatic relief, ensuring adequate hydration, and advising on over-the-counter topical antiviral treatments. Oral antivirals may be prescribed for certain patients.
Genital herpes can be caused by both HSV-1 and HSV-2. HSV-1 is now more common in the UK, whereas HSV-2 is more likely to cause recurrent genital herpes infection. Following prodromal symptoms, patients develop multiple painful clusters of genital blisters that quickly rupture, leaving erosions and ulcers on the external genitalia, perineum, and/or perianal region. Patients should be referred to a sexual health clinic for confirmation of the diagnosis. General advice regarding self-care and analgesia should be provided, along with guidance on minimising transmission to others through practices such as safe sex and avoiding contact with infected areas during outbreaks.
Hand, foot, and mouth disease
Hand, foot, and mouth disease (HFMD) is a common viral infection that primarily affects infants and young children, although it can occur in individuals of any age.
It is usually caused by the enterovirus, most commonly the Coxsackievirus A16. The disease presents with a distinctive set of symptoms, including fever, sore throat, and a rash that appears on the palms of the hands, soles of the feet, and sometimes on the buttocks. Small, painful, red spots or blisters may also develop in the mouth and throat, causing discomfort during eating and drinking. HFMD is highly contagious and spreads through contact with infected individuals or contaminated surfaces. Although most cases are mild and resolve on their own within a week, management involves relieving symptoms with over-the-counter pain relievers, staying well-hydrated, and practicing good hygiene to prevent further spread.
Bullous impetigo
Impetigo is a common superficial bacterial infection of the skin. The two main clinical forms are non-bullous impetigo which account for the majority of cases and bullous impetigo. It is a contagious skin infection caused by S. aureus bacteria. It is more common in children but can also affect adults.
The primary symptoms include the development of large, fluid-filled blisters or bullae that can be painful and itchy. These blisters usually appear on the face, arms, and legs. As the blisters burst, they leave behind raw, red areas that may crust over.
Managing bullous impetigo involves good hygiene practices, such as regularly washing hands and keeping the affected areas clean. Children younger than a year old should be referred to a paediatrician. Oral antibiotics are required for all cases of bollous impetigo. The UK Health Security Agency provides guidance on exclusion from school, childcare facilities, or work. Individuals should stay away until their lesions have fully healed, become dry, and formed crusts, or until 48 hours after starting antibiotics (GOV.UK, 2024).
Cellulitis
Cellulitis is a bacterial skin infection that can lead to the formation of blisters. When blisters occur in cellulitis, they are often painful and filled with clear fluid. Other common symptoms of cellulitis include redness, swelling, warmth, and tenderness in the affected area. The skin may also feel tight and appear shiny. In severe cases, fever and chills may be present. Management depends on the clinical condition of the patient; antibiotics are usually required.
Chronic blistering skin conditions
Pompholyx eczema
Pompholyx eczema, also known as dyshidrotic eczema, is a specific form of eczema that primarily affects the hands and feet. It is characterised by the development of small, itchy blisters on the palms, fingers, soles, or toes. These blisters may be filled with fluid and can cause redness, swelling, and intense itching. In some cases, the skin may become dry and cracked, leading to discomfort and pain.
The exact cause of pompholyx eczema is not fully understood, but it is believed to be linked to allergies, stress, or exposure to certain irritants. Management of pompholyx eczema involves keeping the affected areas clean and dry, avoiding potential triggers, such as allergens and irritants, and using topical corticosteroids or emollients to reduce inflammation and alleviate symptoms.
Contact dermatitis
Contact dermatitis is a common skin condition characterised by inflammation and irritation resulting from direct contact with certain substances. In the UK, contact dermatitis is one of the most frequently reported dermatological disorders. The condition can be caused by exposure to various irritants or allergens, such as certain chemicals, plants, metals, or cosmetics. Symptoms of contact dermatitis typically include redness, itching, burning sensation, and the formation of small blisters or dry, scaly patches on the affected area. In some cases, the skin can become swollen and tender.
Management involves identifying and avoiding the triggering agents, along with the use of topical corticosteroids or emollients to alleviate symptoms and promote healing (Fig. 3).

A 3-year-old girl with contact dermatitis, a day after contact with poison ivy - a subtype of contact dermatitis called phytodermatosis.
Polymorphic light eruption
Polymorphic light eruption (PLE), also known as sun allergy or sun sensitivity, is a common skin condition characterised by a rash that occurs in response to sunlight exposure. In the UK, PLE affects a significant number of individuals, especially during the spring and summer months when sunlight intensity is higher. Symptoms of PLE typically include itchy or burning red rashes, small bumps, or blisters on sun-exposed areas such as the arms, face, and neck. The condition can cause discomfort and make it difficult for affected individuals to enjoy outdoor activities. Management of PLE involves preventive measures such as wearing protective clothing, using broad-spectrum sunscreen, and avoiding prolonged sun exposure during peak hours. Additionally, topical corticosteroids or antihistamines may be prescribed to relieve symptoms in severe cases.
Porphyria
Porphyria is a rare genetic disorder that can manifest in various forms, including blistering of the skin. Blistering is a common symptom in porphyria, particularly in the subtype known as porphyria cutanea tarda (PCT). These blisters usually occur on sun-exposed areas of the skin and can be painful and itchy. Other signs of PCT include skin fragility, scarring, and hyperpigmentation. Management of porphyria involves avoiding triggers such as alcohol, certain medications, and excessive sun exposure. Patients may benefit from regular therapeutic phlebotomy or medication to reduce porphyrin levels. Early diagnosis and proper management are essential to minimise symptoms and prevent associated complications.
Erythema multiforme
Erythema multiforme (EM) is a relatively uncommon, but distinctive, skin disorder characterised by a target-like rash on the skin’s surface. The condition often presents with sudden-onset, symmetrical, and erythematous lesions that appear in various shapes, resembling a target or bull’s-eye. These lesions may be accompanied by itching, burning, or pain. In severe cases, EM can affect mucous membranes, such as the mouth and eyes, leading to painful sores and swelling. The main causative factors include infections, medications, or allergic reactions.
Management of erythema multiforme involves identifying and removing the triggering agent, supportive care to alleviate symptoms, and in severe cases, corticosteroids or other immunosuppressive medicationss to reduce inflammation and hasten recovery.
Bullous pemphigoid
Bullous pemphigoid is a rare autoimmune skin disorder characterised by the formation of large, fluid-filled blisters (bullae) on the skin’s surface. The condition is more common in older adults, typically over the age of 60 years. Symptoms of bullous pemphigoid include intense itching and red, inflamed skin before the appearance of blisters. These blisters can be large and may occur on various parts of the body, such as the arms, legs, abdomen, and mucous membranes.
Management of bullous pemphigoid involves a combination of treatments to control the autoimmune response, reduce inflammation, and alleviate symptoms. Corticosteroids, both topical and systemic, are commonly used, along with immunosuppressive drugs (Fig. 4).

Blisters due to bullous pemphigoid.
Pemphigus vulgaris
Pemphigus vulgaris is a rare and severe autoimmune disorder that affects the skin and mucous membranes. Painful blisters and erosions appear on the skin and inside the mouth, throat, nose, and genitalia. These blisters are fragile and can rupture easily, leading to significant discomfort and risk of infection. Pemphigus vulgaris is often diagnosed through clinical examination, biopsy, and immunofluorescence testing. The management of this condition typically involves high-dose corticosteroids and immunosuppressive medications to control the autoimmune response.
Dermatitis herpetiformis
Dermatitis herpetiformis (DH) is a chronic skin condition characteried by intensely itchy and blistering rashes. It is often associated with coeliac disease, an autoimmune disorder triggered by gluten consumption. The symptoms of DH include clusters of small, red, and raised blisters, which typically appear on the elbows, knees, buttocks, and scalp. The condition is known for its symmetrical pattern of eruption. The blisters and rashes can be extremely uncomfortable and may lead to scratching, causing further skin damage.
The diagnosis of DH is established clinically, histologically, immunopathologically and serologically. A gluten-free diet (GFD) is the treatment of choice for patients with DH. Dapsone and/or other drugs should be used during the period until the GFD is effective.
Drug causes of blisters
Blisters caused by drug reactions, such as those triggered by ACE inhibitors, penicillamine, and barbiturates, is a relatively rare, but serious, condition. These drugs can sometimes induce a hypersensitivity reaction in certain individuals, leading to the development of blisters on the skin. The prevalence of this adverse drug reaction varies depending on the specific drug and individual susceptibility. Symptoms of drug-induced blisters include the sudden appearance of painful and itchy fluid-filled blisters on the skin, which may be localised or widespread. In severe cases, blisters can also affect mucous membranes, such as in the mouth or eyes. Prompt recognition and management are crucial. The causative drug should be stopped immediately, and further management based on the clinical situation of the patient.
Blisters secondary to leg oedema
Blisters can develop as a secondary complication of leg oedema. When leg oedema becomes severe, the excessive fluid build-up can cause the skin to stretch and become fragile, leading to the formation of blisters. These blisters may present as painful, fluid-filled sacs on the affected areas of the legs.
Managing leg oedema and preventing blister formation involves addressing the underlying cause, such as improving heart or kidney function, along with lifestyle modifications such as elevating the legs, wearing compression stockings, and reducing salt intake.
Pemphigoid gestationis
Pemphigoid gestationis, also known as herpes gestationis, is a rare autoimmune blistering skin disorder that primarily affects pregnant women and, in some cases, women in the postpartum period.
The condition usually presents during the second or third trimester and is characterised by the development of intensely itchy, red, and blistering skin lesions. These blisters often appear in the abdomen and other areas of the body. In severe cases, the condition can also involve mucous membranes. Although the exact cause remains unclear, it is believed to involve an abnormal immune response involving the placenta.
The management of pemphigoid gestationis typically involves a combination of topical and oral corticosteroids to control inflammation and suppress the immune response. In most instances, the condition resolves after delivery, but in some cases, it may recur with subsequent pregnancies.
Epidermolysis bullosa
Epidermolysis bullosa (EB) is a rare genetic disorder characterised by extreme skin fragility, leading to the formation of blisters and painful skin lesions. These blisters can appear on the skin in response to minor friction, trauma, or pressure, even from routine activities such as dressing or scratching. The symptoms of EB range from mild to severe and can include skin redness, itching, and open sores. The affected skin areas may also be susceptible to infections. Signs of EB may involve scarring, skin thickening, and nail abnormalities.
A multidisciplinary approach involving dermatologists, wound care specialists, and other healthcare professionals is crucial for providing comprehensive care to individuals with EB.
The management of EB aims to alleviate symptoms and prevent complications. This includes gentle wound care, using soft dressings, and protecting the skin from trauma. In some cases, pain management and antibiotics to prevent infection are essential.
Key points
Blistering skin conditions include life-threatening emergencies, acute conditions manageable in primary care, and chronic conditions requiring dermatology referral An awareness of the range and variety of conditions that share the blistering phenomenon is important in forming a differential diagnosis Accurate history-taking and thorough clinical examination are crucial for diagnosing blistering skin conditions whilst giving due consideration to the overlapping symptoms of other illnesses Life-threatening emergencies include TEN and SSSS; these warrant immediate attention and intervention Acute conditions encountered in primary care include friction blisters, burn blisters, insect bite blisters, and infections such as chickenpox, herpes zoster, and herpes simplex Chronic conditions requiring dermatology referral include bullous pemphigoid, pemphigus vulgaris, pompholyx eczema, contact dermatitis, and rare conditions such as porphyria and pemphigoid gestationis