
Abstract
The potential of endoscopic evaluation in the management of inflammatory bowel diseases (IBD) has undoubtedly grown over the last few years. When dealing with IBD patients, histological remission (HR) is now considered a desirable target along with symptomatic and endoscopic remission, due to its association with better long-term outcomes. Consequently, the ability of endoscopic techniques to reflect microscopic findings in vivo without having to collect biopsies has become of upmost importance. In this context, a more accurate evaluation of inflammatory disease activity and the detection of dysplasia represent two mainstay targets for IBD endoscopists. New diagnostic technologies have been developed, such as dye-less chromoendoscopy, endomicroscopy, and molecular imaging, but their real incorporation in daily practice is not yet well defined. Although dye-chromoendoscopy is still recommended as the gold standard approach in dysplasia surveillance, recent research questioned the superiority of this technique over new advanced dye-less modalities [narrow band imaging (NBI), Fuji intelligent color enhancement (FICE), i-scan, blue light imaging (BLI) and linked color imaging (LCI)]. The endoscopic armamentarium might also be enriched by new video capsule endoscopy for monitoring disease activity, and high expectations are placed on the application of artificial intelligence (AI) systems to reduce operator-subjectivity and inter-observer variability. The goal of this review is to provide an updated insight on contemporary knowledge regarding new endoscopic techniques and devices, with special focus on their role in the assessment of disease activity and colorectal cancer surveillance.
Keywords
Introduction
Endoscopy plays a crucial role in the management of patients with inflammatory bowel diseases (IBD), as it represents the mainstay of both initial diagnostic assessment and evaluation of disease activity.1,2 To date, endoscopic remission is the main treatment target as mucosal healing (MH) is associated with better long-term efficacy outcomes.3–5 However, there is growing evidence that, in addition to MH, the objective of attaining histological remission (HR) might result in further improved outcomes.6,7 In fact, histological disease activity can be detected in up to 40% of patients with endoscopic remission and is associated with a greater risk of clinical relapse. 8
It is currently recommended that endoscopic procedures should be performed with high definition white-light endoscopy (HD-WLE) in order to ensure optimal evaluation of the mucosa. 2 Importantly, residual inflammatory activity persists even if HD-WLE identifies a normal-appearing mucosa. 9 Besides the certain discordance between HD-WLE and histopathology, there is a multitude of histological scoring systems, which makes disease activity estimation more complex. 10 Of note, in recent years, several methods have been introduced to ameliorate the evaluation of the mucosa by endoscopists. New diagnostic devices, such as confocal laser endomicroscopy (CLE), have been developed to better predict histopathology, but their real incorporation in daily practice is not yet well defined. 11 The use of artificial intelligence (AI) systems to standardize operator-subjectivity in IBD and molecular imaging have also come to light as captivating areas of reasearch. 12 In addition, endoscopic surveillance is fundamental in the prevention of colorectal cancer in IBD and the use of modalities such as chromoendoscopy, which involves the spraying of topical dyes to enhance visualization of the mucosa has become the gold standard for dysplasia detection. 13 The Surveillance for Colorectal Endoscopic Neoplasia Detection and Management in Inflammatory Bowel Disease Patients (SCENIC) recommendations highlighted the superiority of HD-WLE over standard definition (SD)-WLE and, most importantly, put emphasis on the preferential use of dye-chromoendoscopy (DCE) over WLE, in guiding targeted biopsies. 14 Despite the authoritative position of the SCENIC consensus, debate is still ongoing, as further research has produced contradictory results, with a recent meta-analysis failing to show a significant superiority of DCE over HD-WLE in dysplasia identification [relative risk (RR) = 1.36; 95% confidence interval (CI): 0.84–2.18]. 15 Moreover, long examination time, need for adequate training, and additional costs for dye spraying might limit the wider application of this technique.16,17 In this context, dye-less chromoendoscopy or virtual chromoendoscopy (VCE) is emerging for its advantageous role in IBD surveillance. 18 In this review, we aim to summarize the current evidence on the most recent endoscopic techniques and devices in two cornerstones of IBD management: evaluation of disease activity and colorectal cancer surveillance. The review also focused on the strengths and limitations of the new advances to provide physicians with an updated insight on what is feasible and effective in a real-life setting.
Methods
We searched the PubMed, Ovid MEDLINE and EMBASE databases using the following keywords ‘endoscopy’, ‘dye-chromoendoscopy’, ‘virtual chromoendoscopy’, ‘endocytoscopy’, ‘confocal laser endomicroscopy’, ‘capsule enteroscopy’, ‘artificial intelligence’, ‘molecular imaging’ individually or in combination with ‘IBD’, ‘Inflammatory Bowel Disease(s)’, ‘Crohn’s disease’, ‘CD’, ‘Ulcerative Colitis’, or ‘UC’. The search focused on full text papers published in English up to December 2020. Abstracts were selected when relevant. No publication date restrictions were imposed. Finally, articles were included in this review if they were relevant, while additional publications were identified through their reference lists. Ethics approval and informed consent were not required for this review.
Endoscopic technologies for the assessment of mucosal inflammation
Endoscopy plays a key role in both Crohn’s disease (CD) and ulcerative colitis (UC). However, in patients with CD inflammation is extended to deeper layers and additional cross-sectional imaging techniques are required to assess transmural healing. 19 Rapid advancements in endoscopic technologies including DCE, VCE, endocytoscopy (EC), and CLE have enabled a more precise assessment of mucosal inflammation (Figure 1). 18

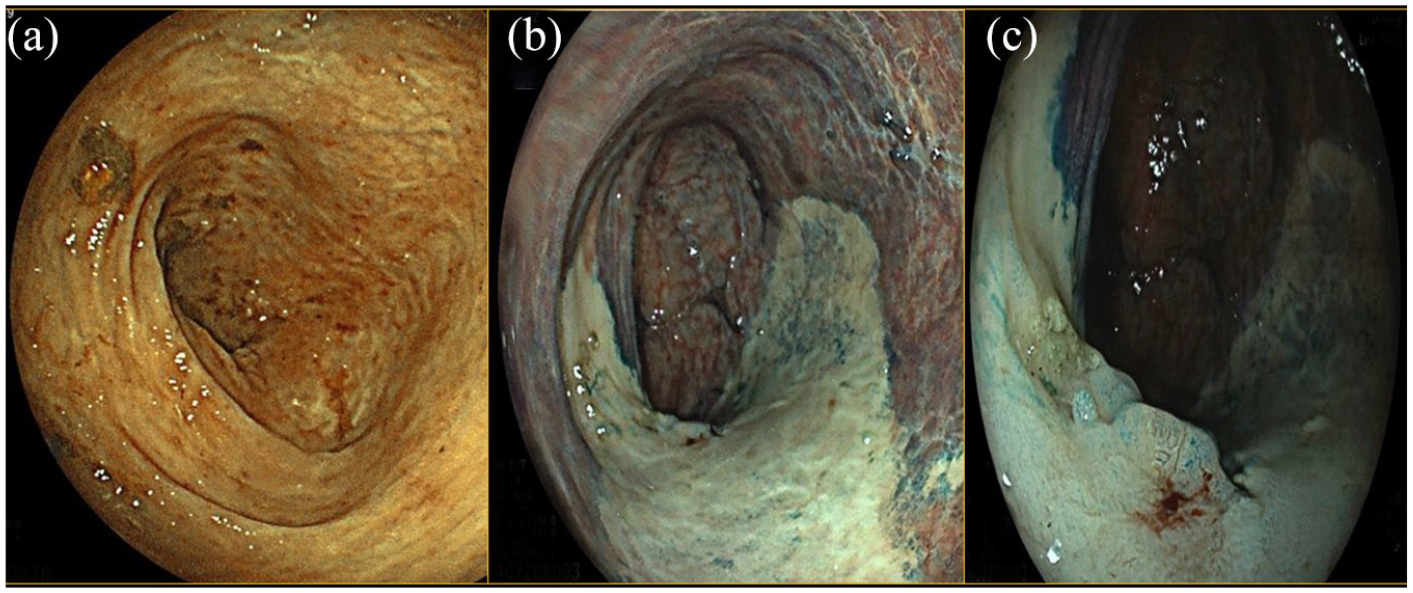
Rectum flat elevated lesion (IIa + IIb according to the Paris classification), pit Patter IIIL–IV according to the Kudo classification. (a) WLE. (b) LCI. (c) BLI. Histologic examination: high grade dysplasia.
Dye-chromoendoscopy
DCE was introduced more than a decade ago. In this procedure, dye agents (e.g., methylene blue and indigo carmine) are applied to improve the detection of the mucosal surface and any potential abnormalities. 20 The interest in DCE derives from the clear benefit in the adenoma detection rate (ADR) in the context of IBD surveillance (Figure 2). 21 Several studies have demonstrated the role of this technology in accurately determining mucosal inflammation.22–24 A paradigmatic trial randomized 263 clinically inactive, UC patients at a 1:1 ratio to undergo conventional colonoscopy or colonoscopy with DCE. 24 A significantly improved correlation between endoscopic assessment of disease extent and histologic data was observed in the group of patients undergoing DCE (89% versus 52%, p < 0.0001). This technique was also able to better predict the degree of inflammatory activity, as a higher percentage of agreement between endoscopic and histopathologic findings was described in the DCE arm (87% versus 54%, p < 0.0002). 24
Descending colon flat lesion (IIb according to the Paris classification), pit Patter IIIL according to the Kudo classification at the same specific points. (a) WLE. (b) DCE. (c) Detail with DCE. Histologic examination: biopsies on the white area compatible with chronic inflammation; biopsies on the lesion compatible with low grade dysplasia.
Dye-less chromoendoscopy
Unlike DCE, which utilizes staining agents and has a long procedure time, dye-less chromoendoscopy or VCE [narrow band imaging (NBI), Fuji intelligent color enhancement (FICE), i-scan, blue light imaging (BLI), and linked color imaging (LCI)] can be performed easily without complex equipment (Table 1). 25
Dye-less chromoendoscopy techniques.

BLI, blue light imaging; FICE, flexible imaging color enhancement; LCI, linked color imaging; NBI, narrow band imaging; OE, optical enhancement; VCE, virtual chromoendoscopy.
NBI uses an optic filter that reduces the light spectrum emitted from the endoscope, thus being absorbed by hemoglobin and providing an enhanced image of the mucosal vascularity. 26 FICE and i-scan belong to DCE. A digital post-processing system is used to enhance the real-time vascular and surface images. 25 Among most advanced developments in light emitting technologies, BLI is based on the not-filtered emission of short wavelength blue light, which is selectively absorbed by hemoglobin. 27 By increasing shades of reddish and whitish tones through the BLI light, an image-enhanced endoscope called LCI, increases slight differences in the red region of the mucosa that are related to inflammation and neoplasia (Figure 3). 28 A prospective study compared structural and vascular alterations of Peyer’s paths (PPs) between 60 IBD patients and 23 healthy controls (HC) through the use of NBI. 29 IBD patients had significant abnormalities in the vessels of PPs (e.g., branch-like structures) compared with HC (p < 0.001). 29 When compared with conventional HD-WLE, NBI was shown to be more accurate in assessing the mucosal vascular pattern (p = 0.0001), which was correlated with the inflammatory histological features in patients with quiescent UC. 30 Danese et al. 31 suggested that NBI colonoscopy might be a useful tool for the in vivo detection of angiogenesis in IBD. 23 In fact, a significant increase in vessel density in inflamed areas was identified in endoscopically normal NBI-positive areas compared with NBI-negative areas (12 ± 1 vessels/field versus 18 ± 2 vessels/field, respectively; p < 0.05). 31 A more recent study reinforced the previous findings on vascular patterns, by showing a correlation between magnified NBI and histological disease activity and prognosis. 32 In particular, Sasanuma et al. 32 focused on the shapes of capillary vessels with magnifying NBI and reported that patients with vessels shaped like bare branches had a greater risk of recurrence compared with those showing a honeycomb-like appearance [odds ratio (OR) = 14.2, 95% CI: 3.3–60.9]. A randomized study comparing i-scan and HD-WLE in 78 IBD patients reported that i-scan correlated better with histologic findings in terms of extent (92.3% versus 48.7%, p = 0.0009) and degree of disease activity (89.7% versus 53.9%, p = 0.066). 33 Accordingly, Iacucci et al. developed and validated a new endoscopic score, the Paddington International Virtual Chromoendoscopy Score (PICaSSO), 34 for assessing the severity of mucosal inflammation in UC by using the i-scan. PICaSSO assesses mucosal (e.g., crypts, erosions, ulcerations) and vascular (e.g., vessels appearance, bleeding) findings and is associated with the HR. 34 Here a particularly positive interobserver agreement was found among experts (kappa = 0.92 and 0.89 in the pre and post evaluations, respectively). Furthermore, the correlation between i-scan optical enhancement (OE) magnification and two histological scores has been evaluated recently. 35 The overall i-scan OE score correlated moderately with two histologic scores used in UC: Robarts Histopathology Index (RHI) (r = 0.61, p < 0.01) and ECAP (Extent, Chronicity, Activity, Plus additional findings) (r = 0.70, p < 0.001). 35 Notably, a strong correlation between magnification endoscopy with i-scan OE and histological inflammation was established also in CD patients. 36 In this population, i-scan OE plus magnification endoscopy demonstrated to precisely identify histological inflammation, defined by the modified Riley score (r = 0.74, 95% CI: 0.58–0.85; p < 0.05). 36 The first study using LCI in UC patients showed that endoscopic assessment with LCI strongly correlated with Matts histopathological grade (p = 0.001). 37 The interobserver agreement for LCI was excellent (kappa > 0.8) between experts and non-experts. 37 Furthermore, LCI is a promising tool for the prediction of clinical relapse in UC, as the average of the LCI-index (based on the redness of the lesion in the region of interest) in relapsing patients was statistically higher than that in non-relapsing (47.23 versus 31.91, p = 0.0003). 37

Flat elevated lesion in the ascending colon (IIa according to the Paris classification), pit pattern serrated (IIO according to the Kudo classification). (a) WLE. (b) LCI. (c) BLI. Histologic examination: serrated lesion without dysplasia.
Endocytoscopy
Endocytoscopy (EC) is an endoscopic imaging technique that allows histological analysis of in vivo optical biopsies during the endoscopic procedure itself, in order to evaluate inflammatory disease activity. 18 In EC, the microscopic visualization of the superficial mucosal layer can extend up to 50 μm in depth. In a pilot study involving 40 IBD (UC = 21, CD = 19) subjects, a concordance of 100% between EC and histopathology assessment (Riley score) of bowel disease activity was found and the intraobserver agreement between two investigators was almost perfect (kappa = 0.76–0.88). 38 Nakazato et al. hypothesized that EC was able to differentiate among patients in endoscopic remission, those in HR (defined as Geboes score ⩽ 2) from patients with histologically active disease. 39 The agreement between EC remission and HR was substantial in patients with a Mayo endoscopic score of 0 (kappa = 0.72). The authors therefore suggested considering the possibility of evaluating histological activity through EC without collecting biopsy specimens. 39 Ueda et al. recently stratified EC appearance into four groups (A, B, C, and D), according to crypt alterations in UC patients. 40 They found significant differences in terms of relapse among the different groups, since patients with disruptive or hidden pits (group D) had higher recurrence rates compared with individuals without crypt abnormalities or with milder EC appearance (75% versus 0, 50% and 40% in group A, B, and C respectively; p < 0.005). 40 Interestingly, a pilot study combined the EC system with the dye-less chromoendoscopy NBI (EC-NBI). 41 A strong correlation between EC-NBI capillary appearance and histological activity according to Geboes index was found (r = 0.871, p < 0.01). 41
Confocal laser endomicroscopy
Confocal laser endomicroscopy (CLE) is an additional endomicroscopic technique that allows for tissue analysis with a maximum depth of imaging of 250 μm. 42 In UC patients in remission, CLE revealed a significant rate of mucosal pathologic abnormalities such as impaired and distorted crypt regeneration, sustained inflammation, and abnormal vascular patterns (all p < 0.001). 43 Interestingly, the Erlangen group investigated the ability of CLE to evaluate and define MH during biological therapy with anti-TNF, aiming at validating the first CLE MH score for UC. 44 The endomicroscopic MH score (eMHs), which includes number of crypts, lumen deformity and leakage, and vascular endothelial permeability, showed high sensitivity, specificity, and accuracy values (100%, 93.75%, and 94.44%, respectively) and a good correlation with the histological Gupta score (r = 0.82, p < 0.0001) and the endoscopic Mayo subscore (r = 0.81%, p < 0.0001). 44 All patients with an eMHs score < 1 were in remission (Partial Mayo score 0) after 3 years, suggesting that CLE and eMHs were valuable tools for prediction of a deep sustained remission. 44 The above-mentioned PICaSSO score and a new probe-based CLE (pCLE) grading system have been tested recently for their ability to approximate histopathologic results and therefore predict HR (defined as RHI ⩽ 6). 45 Preliminary results found that a PICaSSO of ⩽4 and a pCLE of ⩽10 predicted HR with accuracy of 92.7% (95% CI: 84.8–97.3) and 95.1% (95% CI: 88.0–98.7), respectively. 45 A recent prospective observational study focusing on CD patients evaluated the role of CLE in predicting clinical outcomes. 46 The presence of both discontinuous crypt architecture and focal cryptitis was described in 63.3% of patients (n = 31, CLE+ group). 46 After 12 months of follow up, the CLE+ group showed an increased incidence of medical treatment escalation (RR = 3.27, p < 0.001) and transmural lesions (RR = 1.70, p = 0.025) compared with CLI–, suggesting that CLE might represent an attractive prognostic tool. 46 The most relevant studies on available techniques for the evaluation of IBD activity are summarized in Table 2.
Most relevant studies on available techniques for the assessment of mucosal inflammation.

BV-BB, blood vessels shaped like bare branches; BV-H, honeycomb-like blood vessels; CD, Crohn’s disease; CI, confidence interval; CLE, confocal laser endomicroscopy; CO, cryptal opening; DCE, dye-chromoendoscopy; EC, endocytoscopy; ECAP, Extent; Chronicity; Activity; Plus additional findings; eMHs, endomicroscopic MH score; HC, healthy controls; HR, histological remission; IBD, inflammatory bowel diseases; IR, in remission; κ, kappa; LCI, linked color imaging; ME, magnifying endoscopy; MH, mucosal healing; MPV, mucosal vascular pattern; mRI, modified Riley index; NHI, Nancy histology index; NWP, network pattern; OE, optical enhancement; pCLE, probe-based CLE; PICaSSO, Paddington International Virtual Chromoendoscopy Score; PP, Peyer paths; RHI, Robarts histopathology index; RCT, randomized controlled trial; RR, relative risk; UC, ulcerative colitis; WLE, white light endoscopy.
Endoscopic technologies for the detection of dysplasia
Patients with longstanding colonic IBD have an increased risk of developing colorectal cancer (estimated prevalence is approximately 3.5% in both longstanding UC and CD).49,50 Subsequently, 8–10 years after disease onset, IBD patients are enrolled in surveillance colonoscopy programmes. 2
At the moment DCE is recognized as the gold standard method for dysplasia surveillance in IBD, as it was demonstrated to be superior to WLE for dysplasia detection. 14
Dye-chromoendoscopy
A prospective study by Picco et al. reported that indigo carmine CE for UC surveillance resulted in higher rates of dysplasia detection as compared with WLE (21.3% versus 9.3%, p = 0.007). 51 The superiority of DCE over HD-WLE for identifying dysplasia was confirmed by a recent trial that assigned IBD patients randomly to HD-DCE with indigo carmine (n = 152) or HD-WLE (n = 153). 52 Dysplastic lesions were identified in a more significant number of patients with HD-DCE (17 versus 7, respectively; p = 0.032). 52 However, there is contradictory evidence concerning superiority of DCE over HD-WLE (RR = 1.36; 95% CI, 0.84–2.18), and additional studies are needed to support these data. 15
Dye-less chromoendoscopy
The first results from studies evaluating the effectiveness of VCE in revealing dysplastic lesions in IBD are now becoming available. 15 To compare the performance of DCE with NBI for the detection of neoplastic lesions in patients with long-standing UC, a multicenter prospective study randomized 1:1 131 patients to DCE (n = 66) or NBI (n = 65). 53 After targeting suspicious lesions and surrounding mucosa, no significant difference was found in neoplasia detection between NBI and DCE with a mean number of neoplastic lesions per colonoscopy of 0.47 and 0.32, respectively. 53 In addition, per lesion analysis revealed a neoplasia detection of 17% and 16% for NBI, respectively. 53 The authors concluded that, given the longer withdrawal time for DCE, the gold standard might be replaced by NBI. 53 A meta-analysis included 10 randomized controlled trials with the aim of comparing DCE with other endoscopic techniques (SD-WLE, HD-WLE, NBI). 54 DCE was able to identify more dysplastic lesions compared with SD-WLE (RR = 2.12; 95% CI: 1.15–3.91). 54 No significant difference was found between DCE and HD-WLE (RR = 1.42; 95% CI: 0.80–2.52) or NBI (RR = 1.05; 95% CI: 0.64–1.71). 54 The advantages of new VCE techniques are sustained by yet another meta-analysis that confirmed no significant differences among DCE, HD-WLE, NBI, and FICE in detecting neoplasia during IBD surveillance, and also supported the use of Full spectrum HD-WLE. 55 Full-spectrum endoscopy is characterized by supplementary lateral camera lenses in addition to the standard forward-viewing camera. According to Iannone et al., 55 this new colonoscope showed higher odds of detecting neoplastic (OR = 3.22, 95% CI: 0.55–18.98) and non-polypoid lesions (OR = 18.04, 95% CI: 0.49–668.36) in IBD patients.
Two studies by Hoffman et al.56,57 demonstrated that i-scan imaging was superior to standard colonoscopy (neoplasia detection rate: 38 % versus 13 %, p < 0.0001) and equal to DCE in identifying neoplastic lesions (number of neoplastic lesions: 11 versus 11). More recently, a comparative study by Iacucci et al. 48 proved that i-scan and HD-WLE were not inferior to DCE in detecting neoplastic lesions. Adenoma, dysplasia (polypoid and non-polypoid), and adenocarcinoma detection rates were similar in the three-arms study (number of total lesions: 42 versus 27 versus 23 with HD, DCE, and VCE, respectively; p = 0.84). 48 Along these lines, the VIRTUOSO trial randomized 188 longstanding IBD patients (>8 years after disease onset) to VCE with i-scan OE or HD-WLE during colorectal cancer surveillance. 58 The neoplasia detection rate was not statistically different between the two groups (14.9% versus 23.4% with i-scan OE and HD-WLE, respectively, p = 0.14). 58
In addition, an updated meta-analysis conducted by El-Dallal et al. strengthened the concept that dye-less chromoendoscopy, including both NBI and i-scan, was not statistically different in colorectal cancer screening compared with DCE (RR = 0.77; 95% CI: 0.55–1.08) or HD-WLE (RR 0.72; 95% CI: 0.45–1.15). 59
A new classification of lesions discovered during IBD surveillance, FACILE, (Frankfurt Advanced Chromoendoscopic IBD LEsions classification) was recently proposed. 60 It integrates four endoscopic findings (e.g., morphology, surface and vessel pattern, and inflammation), focusing on predictors of dysplasia (e.g., flat shape, irregular vessel and surface pattern, and signs of inflammation). 60 Finally, data about the use of either BLI or LCI to identify neoplastic lesions in patients with IBD are not available yet. However, these newer-generation endoscopic devices proved to be promising in gastrointestinal tumor surveillance in the general population.61–63 A prospective randomized study including 245 patients proved that BLI was more accurate in predicting the histopathology of colon polyps when compared with HD-WLE (92% versus 84%, p = 0.011). 61
Endocytoscopy and CLE
At the moment, consistent evidence from using EC and CLE for dysplasia detection is lacking, probably due to the intrinsic difficulties of obtaining clear images during breathing and cardiac motion. 64 A prospective pilot study in 2011 aimed to evaluate feasibility and diagnostic accuracy of pCLE in UC surveillance. 65 Even though accuracy, specificity, and sensitivity of pCLE were 81%, 82%, and 65%, respectively, these performance measures were inferior to those provided by NBI/HD-WLE in real time (92%, 89% and 100%, respectively). 65 In line with these findings, a study assessing the diagnostic value of CE combined with integrated CLE (iCLE) reported a relatively good accuracy (86.7%, 95% CI: 78.1–95.3 versus 80.3%, 95% CI: 70.7–89.9), but a very poor sensitivity (42.9%, 95% CI: 11.8–79.8 versus 28.6%, 95% CI: 5.1–69.7). 11 The most relevant studies on available technologies for cancer surveillance in IBD are summarized in Table 3.
Most relevant studies on available techniques for dysplasia detection in IBD.

CD, Crohn’s disease; CLE, confocal laser endomicroscopy; CRC, colorectal cancer; DCE, dye-chromoendoscopy; FICE Fujinon intelligent color enhancement; FUSE, full-spectrum endoscopy; HD, high definition; IBD, inflammatory bowel diseases; iCLE, integrated CLE; ns, not significant; NDR, neoplasia detection rate; OE, optical enhancement; OR, odds ratio; pCLE, probe-based CLE; RCT, randomized controlled trial; RR, relative risk; SD, standard definition; UC, ulcerative colitis; VCE, virtual chromoendoscopy; WLE, white light endoscopy.
What is next: capsule endoscopy, artificial intelligence, and molecular imaging
Capsule endoscopy
Small bowel capsule endoscopy (SBCE) is a particularly sensitive instrument used to detect mucosal alterations in the small bowel. 2 It should be considered for patients with clinical suspicion of CD who have already undergone an endoscopy, as stated in more recent guidelines. 2 Since the introduction of the first wireless capsule endoscopy (CE) in the 2000s, several advances, such as improved resolution systems and new types of capsules, have been made to further increase diagnostic yield. 66 Several clinical trials have investigated the potential role of SBCE in MH assessment.67,68 A prospective, multicenter, case-series included 40 patients who underwent SBCE before therapy initiation and after achievement of clinical response. 67 The number of large ulcers detected through SBCE was significantly reduced after treatment (8.3 ± 1.4 versus 5 ± 0.8; respectively, p = 0.01), suggesting that SBCE was a valuable method not only for CD diagnosis, but also for disease activity assessment. 67 Another study demonstrated the effectiveness of SBCE in assessing small bowel treatment response in CD patients with active disease. At week 52, 42% of subjects achieved complete mucosal healing (absence of ulcers) and deep remission (Harvey–Bradshaw Index ⩽ 5 + C-reactive protein ⩽5 mg/l or fecal calprotectin ⩽50 μg/g). 68 More recently Ben-Horin et al. supported the use of CE for the monitoring of quiescent CD patients, 69 as CE was able to predict disease flares within 6 months in a cohort of 61 patients [area under the curve (AUC) of 0.79, % 95 CI: 0.65–0.89; p = 0.011]. In this context, the pan-enteric video capsule system through Pillcam Crohn’s Capsule (Medtronic) constitutes a very promising innovation. 70 In a pilot study including 41 patients with suspected or established CD, the Pillcam Crohn’s Capsule was performed successfully in all 41 videos, allowing for an overall evaluation of the whole intestine without risk of capsule retention. 70 Moreover, thanks to a new integrated reading system, this video capsule permitted the recording and further comparison of patients’ images over time, thus monitoring disease activity and extent under treatment. 71 It is particularly relevant in the pediatric population, where this type of “pan-endoscopy” was shown to effectively monitor mucosal inflammation and successfully guide a treat-to target strategy (twofold increase in the rate of MH and deep remission from baseline to week 54; p < 0.05). 72
Artificial intelligence
The broad term AI generally refers to the ability of a computer to perform functions and reasoning that are typical of the human mind. 73 AI tools are used in the field of endoscopy, and studies evaluating AI systems for endoscopic support have shown good results.74,75 This can be highly valued also in IBD, where the endoscopic assessment can be influenced by operator subjectivity. 76 A computer-aided diagnosis (CAD) system in use with EC was developed to predict persistent histologic inflammation in UC patients. 47 CAD provided good performance measures, showing sensitivity, specificity, and accuracy of 74% (95% CI: 65–81%), 97% (95% CI: 95–99%), and 91% (95% CI: 83–95%), respectively. 47 A CAD system based on GoogLeNet architecture was applied to identify normal mucosa (Mayo endoscopic sub-score 0) and MH (Mayo endoscopic sub-score 0–1) in an independent test set of 3981 images from 114 UC patients. 77 This new system performed well, with AUCs of 0.86 and 0.98 in the two groups, respectively. 77 Moreover, a computer algorithm based on the integration of pixel color data from the redness map and vascular pattern recognition, called red density (RD), was tested in a validation cohort of 29 UC patients. 78 In this latter study, Bossuyt et al. found a correlation between RD score and endoscopic (Mayo endoscopic subscore and UC Endoscopic Index of Severity scores with r = 0.76, p < 0.0001 and r = 0.74, p < 0.0001, respectively) and histological scoring systems (RHI, r = 0.74, p < 0.0001), 78 suggesting that this tool might overcome interobserver variability and subjectivity for disease activity assessment. Deep learning convolutional neural networks (DCNN) belong to the AI field aiming to obtain automatically detailed imaging features, by using multiple network layers without human perceptual biases. 79 Given input data, DCNN manage to autonomously classify images and find the most relevant and useful ones for solving problems. 73 Su et al. conceived of an automatic quality control system (AQCS) based on DCNN and investigated whether it could improve the identification of abnormal lesions such as adenomas and polyps in a large cohort of 659 non-IBD patients. 80 The ADR (0.289 versus 0.165, p < 0.001) and the mean number of adenomas (0.367 versus 0.178, p < 0.001) were significantly higher in the AQCS group when compared with the control. 80
Taking advantage of convolutional neural networks, a fully automated video analysis system was developed recently, aimed at generating Mayo endoscopic scores automatically. 81 The analysis of 264 videos from a multicenter clinical trial proved that this system was able to distinguish remission from endoscopic activity in more than 80% of videos reviewed, with a positive level of agreement with gastroenterologist scoring (kappa = 0.84). 81
Molecular imaging
Molecular imaging is based on the topical or intravenous administration of specific and label structures and the subsequent visualization of targeted structures through simultaneous confocal imaging. 82 Molecular imaging with fluorescent labeled antibody for membrane-bound TNF (mTNF) in conjunction with CLE can be used for in vivo assessment of mTNF-expressing cells in CD inflamed mucosa. 83 In a single-arm clinical study including 25 CD patients, subjects with high numbers of mTNF(+) cells had significantly higher short-term response rates (92%) after 12 weeks of an anti-TNF therapy when compared with patients in the low-mTNF group (15%). 83 Moreover, the clinical response in the high-mTNF group was sustained over a 1-year follow-up period, and was associated with MH at follow-up endoscopy. 83 Similarly, the topical application of fluorescein-labeled antiadhesion (α4β7) molecule antibody was tested in five CD patients with active disease. 84 α4β7+ cells were observed during ex vivo confocal microscopy in only two patients responding to vedolizumab (VDZ). On the contrary, no α4β7+ were detected in the three non-responders to VDZ. 84
Multiphoton imaging is a molecular imaging technique that provides both high cellular resolution and great depth of penetration into the tissue without the need for labels. 85 An endoscopic application of this system, named multiphoton endomicroscopy (MPEM), has recently been proven to yield label-free in vivo histopathologic results in experimental colitis models. 86
Discussion
Progress in endoscopy has paved the way for a more accurate approximation of histopathologic results. Histological modifications, inflammation, and healing are well reflected by endoscopic images provided by cutting-edge techniques. Furthermore, with the introduction of new advanced endoscopic modalities, such as VCE, most dysplastic lesions are visible and a smaller number of biopsy specimens is required, making surveillance less cumbersome for both patients and clinicians.53,87 Among image enhancement techniques, the available evidence suggests that dye-less chromoendoscopy is not inferior to the gold standard DCE in terms of neoplastic lesions detection.48,53,54,59 Moreover, dye-less chromoendoscopy modalities offer the advantage of requiring less procedure time without additional spray-agent costs (median withdrawal time: 15 versus 20 min with VCE and DCE, respectively).53,88 To date, no comparative studies are available between the different VCE techniques and there is no standardized training to evaluate the expertise of operators. The use of one method rather than another is currently linked to cost and the preferences of individual centers. Head-to-head trials between the different VCE modalities are necessary to define whether one approach is in fact superior to the other. Future data well may result in this modern methodology becoming the routine approach for MH assessment and colorectal cancer screening in IBD.
EC and CLE are also available, and they provide the clear advantage of allowing in vivo estimation of inflammatory activity.38,89 These methods could make endoscopic examinations less invasive by reducing the risk of complications related to biopsies. However, they are not yet widely adopted in clinical practice due to the associated costs and the prolonged time required by the procedure (an average increase of approximately 30–40 min). 65 Less expensive confocal probes and economic analyses are eagerly awaited to overcome this significant disadvantage. Moreover, there is no standardized training and the level of expertise among operators is not high, so further studies are needed to increase the use of these techniques in clinical practice.
In addition, SBCE might be seen not only as a diagnostic tool in patients with suspected small bowel CD and normal endoscopy and magnetic resonance enterography (MRE), but also as an accurate investigation method to evaluate MH in small-bowel CD patients. Capsule retention leading to an urgent endoscopic or surgical intervention remains one of the main concerns of this device; as a result, it is not considered in patients with known or suspected stenotic disease or with a history of bowel obstruction. Of note, the new Pillcam Crohn’s capsule with a pan-enteric video system is a promising and safe tool for the assessment of MH in selected populations such as pediatric patients in order to avoid endoscopy deep sedation and biopsy-related complications. The use of pan-enteric CE for activity monitoring should be encouraged in centers where video capsule is a routine examination, and the staff are adequately trained to read images. Due to its likely cost-effectiveness (mean total 20-year cost per patient: £38,043 versus £42,266 with pan-enteric CE and colonoscopy ± MRE, respectively) it may well represent a valid alternative to colonoscopy combined with MRE. 90
AI represents a revolutionary technique in the endoscopy field, providing an objective and accurate evaluation of disease severity. AI offers enormous potential to improve the quality of endoscopic procedures and ultimately to reduce the number of biopsy specimens. 91 The use of AI in endoscopy is also expected to increase the ADR and help non-expert endoscopists in the challenging differentiation between inflammatory and neoplastic lesions, although this will need to be confirmed in studies involving IBD patients. Finally, implementing molecular imaging in endoscopy could provide physicians with a real-time in vivo view of targeted biomarkers, but it is still a research field that requires further validation [ClinicalTrials.gov identifier: NCT02852850].
Conclusion
The goal of HR in IBD management has certainly influenced new advances in the endoscopic field. Endoscopy is now asked to accurately describe inflammatory disease activity and promptly identify suspected lesions during the ongoing procedure, thus getting as close as possible to microscopic findings. Dye-less chromoendoscopy has already demonstrated to be feasible and cost-effective in a real-life setting, whereas endomicroscopy systems still appear as complex and costly techniques. New pan-enteric video capsules might enrich the endoscopic armamentarium for monitoring disease in specific populations. Further clinical studies are expected to confirm the great expectations placed on AI tools and molecular imaging.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848211005692 – Supplemental material for Rediscovering histology: what is new in endoscopy for inflammatory bowel disease?
Supplemental material, sj-pdf-1-tag-10.1177_17562848211005692 for Rediscovering histology: what is new in endoscopy for inflammatory bowel disease? by Virginia Solitano, Ferdinando D’Amico, Mariangela Allocca, Gionata Fiorino, Alessandra Zilli, Laura Loy, Daniela Gilardi, Simona Radice, Carmen Correale, Silvio Danese, Laurent Peyrin-Biroulet and Federica Furfaro in Therapeutic Advances in Gastroenterology
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
V. Solitano, F. D’Amico, A. Zilli, L. Loy, D. Gilardi, S. Radice, and C. Correale declare no conflict of interest. M. Allocca received consulting fees from Nikkiso Europe and lecture fees from Janssen and Pfizer. G. Fiorino received consultancy fees from Ferring, MSD, AbbVie, Takeda, Janssen, Amgen, Sandoz, Samsung Bioepis, and Celltrion. S. Danese has served as a speaker, consultant, and advisory board member for Schering-Plough, AbbVie, Actelion, Alphawasserman, AstraZeneca, Cellerix, Cosmo Pharmaceuticals, Ferring, Genentech, Grunenthal, Johnson and Johnson, Millenium Takeda, MSD, Nikkiso Europe GmbH, Novo Nordisk, Nycomed, Pfizer, Pharmacosmos, UCB Pharma, and Vifor. L. Peyrin-Biroulet has served as a speaker consultant and advisory board member for Merck, Abbvie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Hospira/Pfizer, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, HAC- Pharma, Index Pharmaceuticals, Amgen, Sandoz, Forward Pharma GmbH, Celgene, Biogen, Lycera, Samsung Bioepis, and Theravance. F. Furfaro received consulting fees form MSD and Abbvie and lecture fees from Janssen and Pfizer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.