
Abstract
Background:
The phenotype of immunoglobulin G4 (IgG4)-related cholangitis (IRC) patients among type 1 autoimmune pancreatitis (AIP-1) patients in Taiwan, where secondary biliary cholangitis is prevalent, is unknown.
Objectives:
To evaluate the phenotype of IRC in AIP-1 patients.
Design:
Retrospective cohort study.
Methods:
A 15-year cohort study of 237 AIP-1 patients was conducted. AIP-1 was diagnosed according to the HISORt criteria.
Results:
Of 237 AIP-1 patients, 90 (37.9%) had IRC (males: n = 80 (88.9%); type 1 IRC: n = 80 (88.8%); mean age: 65.63 years). Among AIP-1 patients, those with IRC had higher alanine aminotransferase (ALT) (179.4 ± 202.6 vs 118.0 ± 167.8 U/L, p = 0.014), alkaline phosphatase (ALP) (322.5 ± 239.1 vs 201.4 ± 193.7 U/L, p < 0.001), total bilirubin (bili-T) (5.69 ± 5.28 vs 2.95 ± 4.19 mg/dL, p < 0.001), and IgG4 (1271.9 ± 1256.3 vs 904.0 ± 811.4 mg/dL, p = 0.015) levels and a borderline higher cumulative incidence of mortality (14.4 vs 7.5%, p = 0.068) than those without IRC did. Moreover, baseline bili-T levels (odds ratio (OR): 1.194, p = 0.031) (cutoff: >2.2 mg/dL) were independently associated with IRC. Among AIP-1 patients, baseline ALP (OR: 1.004, p = 0.001), fibrosis-4 index (OR: 1.156, p = 0.025), cirrhosis (OR: 23.157, p < 0.001), and neutrophil-to-lymphocyte ratio (NLR) (OR: 1.103, p = 0.008) were associated with mortality. Among the IRC-AIP-1 patients, baseline ALP levels (OR: 1.002, p = 0.028) and NLR (OR: 1.091, p = 0.012) were associated with mortality.
Conclusion:
In total, 37.9% of AIP-1 patients had IRC. Higher levels of hepatocellular injury, cholestatic features, and IgG4 were noted in patients with IRC than in patients without IRC. Baseline bili-T level (cutoff > 2.2 mg/dL) is an indicator of IRC among AIP-1 patients. Biliary injury and systemic inflammation are associated with mortality in all AIP-1 and IRC-AIP-1 patients. Liver fibrosis subsequent to IRC might further increase mortality in AIP-1 patients.
Plain language summary
In total, 37.9% of AIP-1 patients had IRC. Higher levels of hepatocellular injury, cholestatic features and IgG4 were noted in patients with than in those without IRC. Baseline bili-T level (cutoff > 2.2 mg/dL) is an indicator of IRC among AIP-1 patients. Biliary injury and systemic inflammation are associated with mortality in all AIP-1 and IRC-AIP-1 patients. Liver fibrosis subsequent to IRC might augment mortality further in AIP-1 patients.
Introduction
Immunoglobulin G (IgG4)-related cholangitis (IRC), 1 namely, IgG4-related sclerosing cholangitis, 2 is the most common hepatobiliary manifestation of IgG4-related disease (IgG4-RD), a systemic fibroinflammatory disorder. 1 IRC is diagnosed mainly in elderly men and is closely associated with type 1 autoimmune pancreatitis (AIP-1), which is the most frequent manifestation of IgG4-RD of the digestive tract. 1 On the basis of the location of the bile duct stenosis, 3 IRC is classified into four types, with type 1 IRC indicating distal bile duct stenosis and being associated mostly with AIP-1. 4 Many years ago, the prevalence and incidence of proximal IRC were suggested to be 1.0 and 0.3 per 100,000 people, respectively. 5 However, a recent study revealed that the point prevalence of IRC was 2.18 per 100,000 people in Japan. 6 The diagnosis of IRC may be challenging at times because it closely resembles other hepatobiliary diseases such as primary sclerosing cholangitis, secondary sclerosing cholangitis, and cholangiocarcinoma. The pathogenesis of IRC is currently viewed as multifactorial. In addition to genetic predisposition, environmental factors, such as blue-collar work, lifelong exposure to occupational toxins, and previous malignancy, are reportedly linked to IRC. IRC has an excellent prognosis when promptly diagnosed and treated with steroids. 2 Among IRC patients, the most common presentation is chronic or recurrent cholestatic jaundice, and this is observed in up to 75% of these patients. 7 Pancreatic exocrine insufficiency, diabetes mellitus, renal impairment, and biliary cirrhosis have been reported to occur in up to 53%, 37%, 12%, and 7.5% of IRC patients, respectively. 1 Furthermore, relapse and cancer are observed in 19.7% and 15% of IRC patients, respectively. 8 Although secondary cholangitis after biliary malignancy 9 or stones 10 is prevalent in Taiwan, the prevalence and phenotype of IRC among AIP-1 patients remain unknown. Accordingly, on the basis of the database of patients who underwent IgG4 assessment, pancreatic biopsy, and imaging studies, we conducted a 15-year hospital-based cohort study to comprehensively explore the impact of IRC on the outcomes of AIP-1 patients.
Methods/materials
Patients
Patients with serum IgG4 levels >200 mg/dL (serum IgG4 levels were measured using immunonephelometry with a Siemens BN ProSpec instrument, with a reference range of serum IgG4: 3–201 mg/dL (Siemens Healthcare Diagnostics, Germany)) or compatible histopathology of AIP-1 (tissues acquired from endoscopic ultrasound (EUS)-guided biopsy or operation) at a medical center in Taiwan between January 2008 and June 2023 were surveyed for the presence of AIP-1. For this retrospective AIP-1 cohort, AIP-1 was defined according to the HISORt criteria (Histology, Imaging, Serology, Other organ involvement, and response to steroid therapy),11,12 and the diagnosis of IRC was based on the following criteria: (I) narrowing of the intrahepatic and/or extrahepatic bile duct on imaging; (II) thickening of the bile duct wall on imaging; (III) serological findings (i.e., elevated levels of serum IgG4); (IV) pathology; (V) other organ involvement; and (VI) steroid effectiveness. 2 The IRC type was defined as described previously. 13 Specifically, the inclusion criteria of this study were as follows: (1) age ⩾18 years; (2) presence of AIP-1; and (3) available pancreatic imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI). Patients without data from CT scans or MRI studies of the pancreas or biliary tree, or those with incomplete clinical data, were excluded. The flowchart of the AIP-1 patient enrollment process is presented in Figure 1.

Flowchart of patient enrollment.
Study design
The demographic data, physical findings, symptoms, and biochemistry results at the time of diagnosis were recorded. Alcohol consumption, smoking habits, and body mass index (BMI) were determined on the basis of medical records. The following biochemical parameters were examined: IgG4 (cutoff: >200 mg/dl), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alpha-fetoprotein (AFP), direct bilirubin (bili-D), total bilirubin (bili-T), estimated glomerular filtration rate (eGFR), alkaline phosphatase (ALP), GT γ-glutamyl transpeptidase (γ-GT), amylase, lipase, alpha-fetoprotein (AFP), carbohydrate antigen 19-9 (CA 19-9), carcinoembryonic antigen (CEA), fibrosis-4 (FIB-4), and neutrophil-lymphocyte ratio (NLR). The biochemical parameters were measured with routine automated methods at clinical laboratories. Liver ultrasound and FibroScan were performed to assess fatty liver and liver cirrhosis (LC).14,15 Abdominal CT and MRI images were reviewed by both experienced radiologists and gastroenterologists with expertise in pancreatic diseases to confirm compatibility with AIP-1 imaging findings and to exclude pancreatic malignancy. The medications used for AIP-1 treatment, including prednisolone, methylprednisolone, and azathioprine, were recorded. The manifestations, including LC, fatty liver, hypertension, diabetes, dyslipidemia, hyperuricemia, cerebrovascular accident (CVA), acute coronary syndrome (ACS), autoimmune diseases (inflammatory bowel disease (IBD), systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SS), Sjögren’s syndrome, psoriasis autoimmune, and thyroid disease), IRC, dacryoadenitis, sialadenitis, retroperitoneal fibrosis, renal diseases, osteoporosis, extrahepatic cancer, and mortality, were assessed and diagnosed in accordance with previous studies.14–19 The primary cancers were diagnosed on the basis of pathology. Each primary cancer was confirmed by specialists. The diagnosis and stage of each cancer were recognized in the database of the National Cancer Registration. Specifically, hepatocellular carcinoma (HCC) was diagnosed on the basis of histology/cytology or ultrasound findings plus high AFP levels or imaging findings as described in generally accepted guidelines. 20 Finally, patients diagnosed with AIP-1 were included in the study cohort and classified into those with and without IRC.
Study endpoints
The primary endpoint of this study was to identify clinical factors associated with the presence of IRC among AIP-1 patients. Secondary endpoints included determining overall mortality and clinical outcomes during the follow-up of the AIP-1.
Statistical analyses
All the statistical analyses were performed with the Statistical Package for Social Science (SPSS package version 21, SPSS Inc., Chicago, IL, USA) or MedCalc (MedCalc version 12.4; MedCalc Software Corp., Maine, USA) software. Continuous variables were analyzed with student’s t test, and categorical variables were analyzed with a chi-square test or Fisher’s exact test, as appropriate. Nonparametric tests were applied in the analysis where indicated. The Kaplan‒Meier method was used to estimate the cumulative incidence of various dependent events. Multivariate Cox regression models were used to assess the relationships between independent and dependent variables by adjusting for the independent variables with a p value < 0.157 21 during univariate Cox analyses. Receiver operating characteristic (ROC) curve analyses were performed to evaluate whether the independent variables predicted the dependent variables. The Youden index was used to identify the optimal cutoff values for the independent variables from the coordinate points of the ROC curves. On the basis of two-tailed tests of the null hypothesis, statistical significance was defined at the 5% level.
Reporting guidelines
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 22
Results
Baseline characteristics
Among the 237 patients with AIP-1, 90 (37.9%) had IRC, 34 had undergone EUS, and 16 had undergone EUS-guided pancreas biopsy to confirm the presence of AIP-1. AIP-1 patients with IRC had higher ALT, ALP, bili-D, bili-T, and IgG4 levels than did those without IRC (Table 1). Among the 90 IRC patients, 80 (88.9%) were males, and the mean and median ages of the IRC patients were 65.6 years and 66.0 years, respectively; 80 (88.8%) had type 1 IRC, 1 (1.1%) had type 2 IRC, and 9 (10%) had type 3 IRC. In total, 20 (22.2%) patients had blue-collar occupations. The other 70 IRC patients had the following occupations: housewife (n = 5), businessman (n = 4), freelancer (n = 3), counter staff (n = 2), salesperson (n = 2), student (n = 1), retiree (n = 16), unemployed (n = 18), or unidentified job (n = 19).
Baseline characteristics of 237 patients with AIP-1.
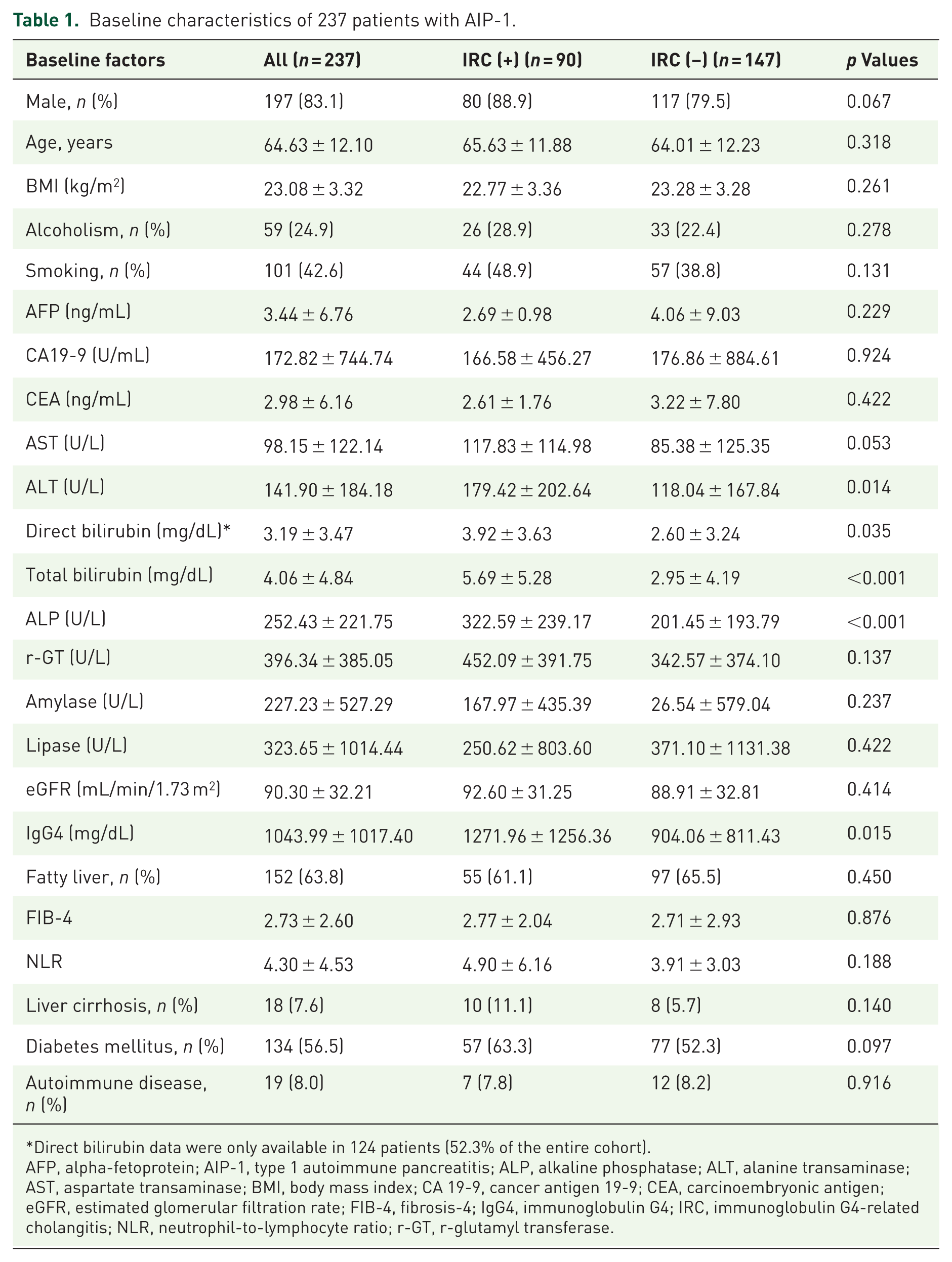
Direct bilirubin data were only available in 124 patients (52.3% of the entire cohort).
AFP, alpha-fetoprotein; AIP-1, type 1 autoimmune pancreatitis; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; CA 19-9, cancer antigen 19-9; CEA, carcinoembryonic antigen; eGFR, estimated glomerular filtration rate; FIB-4, fibrosis-4; IgG4, immunoglobulin G4; IRC, immunoglobulin G4-related cholangitis; NLR, neutrophil-to-lymphocyte ratio; r-GT, r-glutamyl transferase.
Bili-T was independently associated with IRC among AIP-1 patients
As shown in Table 2, bili-T (odds ratio (OR): 1.194, p = 0.031) was independently associated with IRC among the 237 AIP-1 patients. The ROC analysis revealed the area under the ROC curve (0.698; 95% confidence interval: 0.628–0.729; sensitivity, 64.8%; specificity, 70.0%) with a cutoff value of >2.2 mg/dL for bili-T to demarcate IRC (Figure 2).
Baseline factors associated with IRC in 237 patients with AIP-1.

AFP, alpha-fetoprotein; AIP-1, type 1 autoimmune pancreatitis; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; CA 19-9, cancer antigen 19-9; CEA, carcinoembryonic antigen; CI, confidence interval; eGFR, estimated glomerular filtration rate; FIB-4, fibrosis-4; IgG4, immunoglobulin G4; IRC, immunoglobulin G4-related cholangitis; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; r-GT, r-glutamyl transferase.

ROC analyses of total bilirubin (bili-T) levels to predict IRC among AIP-1 patients.
Treatments
In total, 45 (18.9%) of the 237 AIP-1 patients did not receive any immunosuppressive therapy (IST) and experienced spontaneous resolution. Among patients who underwent standard therapy with prednisolone alone, prednisolone with subsequent azathioprine or methylprednisolone, no significant difference in the relapse rate was observed between AIP-1 patients with and without IRC (20.5% vs 21.1%, p = 0.532). For local treatment, 34 (37.8%) of the 90 IRC patients underwent endoscopic papillotomy (EPT), 2 (2.2%) underwent stricture dilatation, 34 (37.8%) underwent endoscopic retrograde biliary drainage (ERBD), and 8 (8.9%) underwent percutaneous transhepatic cholangiography (PTC). Among the IRC patients, the mortality rates did not differ between those with and those without EPT (p = 0.193), stricture dilatation (p = 0.269), ERBD (p = 0.193), or PTCD (p = 0.675).
Outcomes
The cumulative incidences of various outcomes are shown in Table 3. Among AIP-1 patients, a borderline higher cumulative incidence of mortality was noted in patients with IRC than in those without IRC (14.4 vs 7.5%, p = 0.068) (Figure 3). The mortality rate was 10.1% (n = 24) among the 237 AIP-1 patients and 16.6% (n = 15) among the IRC-AIP-1 patients. Specifically, among the 24 AIP-1 patients who died, most (n = 16, 66.7%) died of sepsis, and the others died of terminal cancer (n = 5, 20.8%) or cardiovascular events (n = 3, 12.5%). Among the 15 IRC-AIP-1 deaths, most (n = 12, 80%) were from sepsis, and the others occurred secondary to cardiovascular events (n = 2, 13.3%) or terminal cancer (n = 1, 6.6%). Among the 90 IRC patients, 11 (12.2%) developed cancer, including colon cancer (n = 2), prostate cancer (n = 2), HCC, pancreatic cancer, bladder cancer, gastric cancer, lung cancer, oral cancer, and skin cancer (one patient each). However, there was no difference in the relapse rate between the AIP patients with and without IRC (p = 0.29).
Cumulative incidences of various outcomes in 237 patients with AIP-1.

AIH, autoimmune hepatitis; AIP-1, type 1 autoimmune pancreatitis; IRC, IgG4-related cholangitis; PBC, primary biliary cholangitis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.

Cumulative incidence of mortality in AIP-1 patients with and without IRC. Red line: AIP-1 patients with IRC; black line: AIP-1 patients without IRC.
Factors associated with mortality
Among the 237 AIP-1 patients, baseline ALP, FIB-4, and NLR levels and cirrhosis were independently associated with mortality (Table 4). Among the 90 IRC-AIP-1 patients, ALP and the NLR were independently associated with mortality (Table 5).
Baseline factors associated with mortality in 237 patients with AIP-1.

AFP, alpha-fetoprotein; AIP-1, type 1 autoimmune pancreatitis; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; CA 19-9, cancer antigen 19-9; CEA, carcinoembryonic antigen; CI, confidence interval; eGFR, estimated glomerular filtration rate; IgG4, immunoglobulin G4; IRC, immunoglobulin G4-related cholangitis; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; r-GT, r-glutamyl transferase.
Baseline factors associated with mortality in 90 patients with IRC.
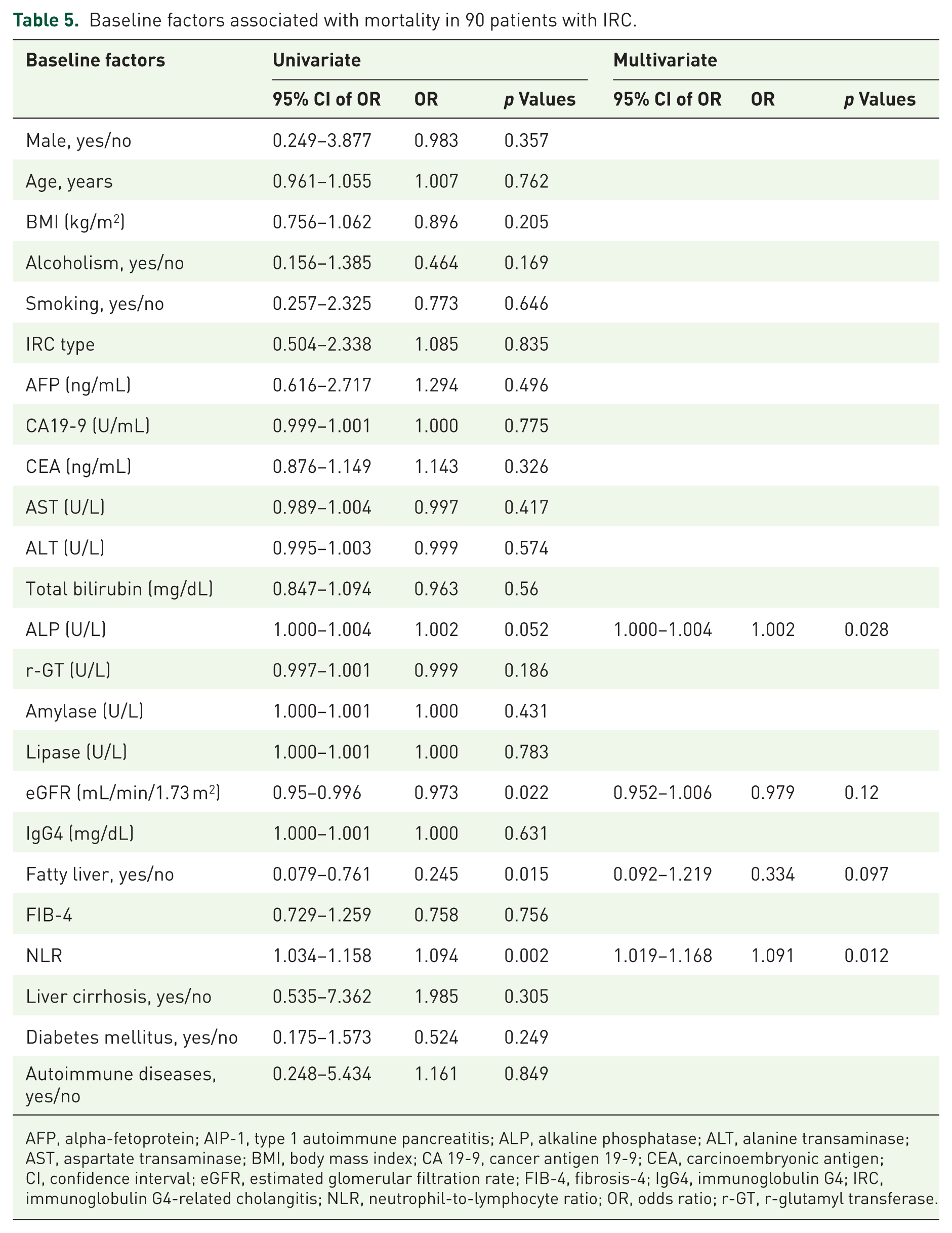
AFP, alpha-fetoprotein; AIP-1, type 1 autoimmune pancreatitis; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; CA 19-9, cancer antigen 19-9; CEA, carcinoembryonic antigen; CI, confidence interval; eGFR, estimated glomerular filtration rate; FIB-4, fibrosis-4; IgG4, immunoglobulin G4; IRC, immunoglobulin G4-related cholangitis; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; r-GT, r-glutamyl transferase.
Discussion
EUS plays an important role in the diagnosis of AIP, particularly in patients with focal lesions where differentiation from pancreatic cancer may be difficult, 23 as EUS‑guided fine‑needle aspiration or biopsy allows targeted tissue acquisition for histological evaluation. 24 In the current study, 34 of the enrolled patients had received EUS, and 16 of them had received EUS-guided pancreas biopsy to confirm AIP-1 and exclude the possibility of pancreatic malignancy. Therefore, unnecessary pancreatic operations and the associated complications were prevented in these patients. The finding that 37.9% of patients with AIP-1 had IRC is within the previously reported range (17%–74%) of AIP-1 patients with concomitant IRC.25,26 The mean age of the patients in our IRC cohort was 65.69 years, and 88.9% were male, which is consistent with previous findings that IRC patients are typically 60–80 years old and that 80%–85% are male. 27 Moreover, the finding that 88.8% of the IRC-AIP-1 patients have type 1 IRC is consistent with the fact that type 1 IRC is present in the majority of IRC-AIP-1 patients. 4 Furthermore, the finding with respect to mortality in AIP-1 patients (10.1%) is similar to that reported previously (10.0%). 28 Finally, blue-collar work was shown to be a risk for IRC, and the prevalence of patients in blue-collar work occupations (n = 20, 22.2%) was close to the previously reported rate (15.8%). 29 The majority of the IRC patients, other than blue-collar workers (n = 53), were retirees, unemployed, or had unidentified jobs, which might overlap with potential exposures and workplace hazards that occur in blue-collar work occupations, and thus potentially contribute to IRC development. Together, the above findings support the reliability of the data.
Notably, our study is the first to identify the phenotype of IRC patients in the AIP-1 cohort in Taiwan, where secondary cholangitis is prevalent,9,10 and our findings highlight the role of baseline bili-T with a cutoff of >2.2 mg/dl as an indicator of IRC among AIP-1 patients. IRC frequently results in biliary occlusion and subsequent hepatocellular damage, which explains why higher levels of hepatocellular and cholestatic features were noted in AIP patients than in those without IRC. Although patients with IRC-AIP-1 have been reported to have higher IgG2 levels than do patients with AIP-1 alone, 30 to our knowledge, our finding of higher IgG4 levels in AIP-1 patients with IRC than in those without IRC is novel and notable. Two parallel immunological responses, namely, a proinflammatory, tissue-destructive process and an anti-inflammatory feedback response, which is likely related to IgG4 production, 31 are thought to underlie the pathophysiology of IgG4-related pancreatobiliary diseases. Although the precise role of IgG4 in AIP-1 remains uncertain, the results of recent studies suggest that IgG4 represents a response that dampens excessive inflammation, 12 and this scenario explains why AIP-1 patients with IRC had higher IgG4 levels than their counterparts, as the former demands greater power to buffer more severe inflammation after cholangitis.
No difference in the cumulative incidence of cancer was noted between AIP-1 patients with and without IRC. Although pancreatic and biliary cancers are reported to be the most common cancers in patients with IRC, 8 we observed that of the 14 IRC patients who developed cancers, only 1 had pancreatic cancer, and none had cholangiocarcinoma. The impact of IRC on the development of pancreatic and biliary cancers seemed to be negligible in the current cohort.
The finding that ALP and NLR levels are associated with mortality in both the AIP-1 patient and IRC-AIP-1 patient groups indicates that biliary tract injury 32 and the balance between the inflammatory response (neutrophils) and the adaptive immune response (lymphocytes) 33 are crucial factors that influenced mortality in the current cohort. Moreover, the higher NLR indicates the higher severity of sepsis and is therefore useful for predicting sepsis. 34 Consistently, over 60% and over 80% of the deaths among all AIP-1 and IRC-AIP-1 patients, respectively, occurred after the onset of sepsis. A borderline higher cumulative mortality was noted in AIP-1 patients with IRC than in those without IRC. This shows that the presence of IRC is detrimental to the AIP-1 prognosis. In addition to ALP and NLR levels, FIB-4 and cirrhosis were independently associated with mortality in the AIP-1 patient group, suggesting that liver fibrosis or even cirrhosis after IRC progression might increase mortality further in AIP-1 patients. Because a borderline higher cumulative incidence of mortality was noted in AIP-1 patients with IRC than in those without IRC, and because of the potential of IRC-AIP-1 patients to develop liver fibrosis, IRC-AIP-1 patients should receive special attention.
The current study has several limitations due to its retrospective nature. First, the local biliary treatments for the enrolled patients could not be standardized, thus leading to potential bias, although mortality did not differ among the groups that received various local treatments. Second, AIP-1 patients with extrapancreatic involvement, particularly IRC, 28 may have a higher risk of relapse and often require maintenance IST. 35 Moreover, compared with AIP-1 patients without IRC, AIP-1 patients with IRC had higher IgG4 levels, which suggests that IRC-AIP-1 patients may be prone to relapse, as high IgG4 levels are considered one of the most relevant risk factors associated with AIP relapse. 36 However, the relapse rates of the AIP-1 patients with IRC were similar to those of AIP-1 patients without IRC under various IST regimens, including prednisolone alone, prednisolone with subsequent azathioprine or methylprednisolone administration. Although unidentified local or ethnic factors might account for the discrepancy, both the limited case number and the reliance on unadjusted physician clinical judgment for IST use in the current study might have introduced additional bias and attenuated the results. Third, although higher bili-D levels were noted in AIP-1 patients with IRC than in those without IRC, detailed data on direct and indirect bilirubin fractions were not consistently available for all AIP-1 patients (only 52.3% of the patients had bili-D data, Table 1). Subgroup or multivariate analysis based on bilirubin fractions was thus not feasible. Fourth, the difference in mortality between patients with and those without IRC was only borderline significant. The precise significance might be underestimated in such a medium-sized cohort. Future large-scale prospective studies of AIP-1 and IRC patients with comprehensive biochemistry assessments, uniform IST regimens, and local treatment procedures are needed to verify the findings described here.
Taken together, our data show that of the 237 enrolled AIP-1 patients, 37.9% had IRC, and these patients had higher levels of hepatocellular and cholestatic features and IgG4 than did patients without IRC. A Bili-T>2.2 mg/dL suggests the presence of IRC among AIP-1 patients. A borderline higher cumulative mortality was noted in AIP-1 patients with IRC than in those without IRC. Biliary injury and systemic inflammation are associated with mortality in all AIP-1 and IRC-AIP-1 patients. Liver fibrosis after IRC might further increase mortality among AIP-1 patients. Special attention is needed for IRC-AIP-1 patients.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261447198 – Supplemental material for Jaundice marks immunoglobulin G4-related cholangitis in type 1 autoimmune pancreatitis patients
Supplemental material, sj-docx-1-tag-10.1177_17562848261447198 for Jaundice marks immunoglobulin G4-related cholangitis in type 1 autoimmune pancreatitis patients by Chi-Huan Wu, Kai-Feng Sung, Chung-Guei Huang, Shih-Chiang Huang, Yung-Lin Chang, Sheng-Fu Wang, Wei-Pin Lin, Tsung-Hsing Chen, Cheng-Jen Chen, Chung-Wei Su, Cheng-Yu Lin, Chia-Jung Kuo, Yi-Chung Hsieh, Jennifer Tai and Ming-Ling Chang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors thank Ms. Shu-Chun Chen, Ms. Yi-Ting Lee, Ms. Ya-Fen Lin, Ms. Li-Chuan Pan, and Mr. Shun-Sian Siao from the Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Taiwan, for their assistance with data mining.
Declarations
Availability of data and materials
The data that support the findings of this study are available from the corresponding author* upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.