
Abstract
Background:
Gastric variceal bleeding is a common and serious complication of liver cirrhosis and carries a high mortality. Endoscopic variceal ligation (EVL) is widely used, but its efficacy for gastric varices is limited by incomplete variceal capture and a high rate of post-ligation rebleeding.
Objectives:
To evaluate the effectiveness and safety of metal clip-assisted endoscopic variceal ligation (MEVL) versus traditional ligation (TL) in adults with cirrhotic gastric varices.
Design:
Single-center retrospective observational cohort study, reported according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
Methods:
Adults with cirrhosis and gastroesophageal (gastroesophageal varices)-type varices undergoing elective ligation for primary or secondary prophylaxis at Henan Provincial People’s Hospital between May 2019 and December 2023 were included; emergency endoscopies were excluded. Non-selective beta-blocker co-therapy was standardized. Baseline imbalance was addressed by propensity score matching and inverse probability of treatment weighting (IPTW), pre-specified as the primary balancing method. Multivariable logistic regression, Cox proportional hazards modeling, and post hoc power were computed in SPSS 26 and Python 3.11.
Results:
Ninety-nine patients were analyzed (MEVL n = 46; TL n = 53) with comparable baseline characteristics. One-session eradication was achieved in 33 of 46 MEVL patients (71.7%) compared with 26 of 53 TL patients (49.1%), favoring MEVL after IPTW adjustment (odds ratio (OR) 2.55, 95% confidence interval (CI) 1.03–6.27; p = 0.042) and on Cox regression (adjusted hazard ratio 1.53, 95% CI 1.00–2.35; p = 0.049). Early rebleeding between 120 h and 6 weeks occurred in 0 of 46 MEVL patients versus 5 of 53 TL patients (9.4%; p = 0.059; post hoc power 87%); the adjusted OR for any rebleeding favored MEVL (0.24, 95% CI 0.07–0.82; p = 0.023). All-cause mortality (3/46 vs 6/53) and adverse reactions (11/46 vs 14/53) did not differ.
Conclusion:
MEVL was associated with higher one-session eradication than TL, with no increase in adverse reactions. A reduction in cumulative rebleeding was suggested by adjusted logistic regression but was not confirmed by time-to-event Cox analysis; this finding should be interpreted as exploratory rather than definitive. Multicenter prospective validation is required.
Clinical trial registration:
Since this is a retrospective, non-randomized study, it was not registered as a clinical trial.
Plain language summary
Bleeding from enlarged blood vessels (varices) in the stomach is a serious complication of advanced liver disease, and the standard endoscopic treatment of placing rubber bands around the varices works less reliably for stomach varices than for esophageal varices. In this single-hospital retrospective study, we compared a modified technique called MEVL, in which small metal clips are placed on the vessels feeding each varix before band ligation, with traditional band ligation alone in 99 selected adult patients with cirrhosis-related cardiofundal-extension gastric varices (Sarin GOV1 and GOV2 types). Patients in the MEVL group were more likely to achieve complete eradication of varices after a single procedure (33 of 46 patients, 71.7 percent, versus 26 of 53 patients, 49.1 percent). The rate of procedure-related complications was similar in both groups. Because patients in this study were not randomly assigned to a treatment, and because MEVL was used predominantly in the later years of the study, these results should be interpreted as preliminary. A multicentre randomised trial is needed before MEVL can be recommended as superior to traditional band ligation for routine use.
Keywords
Introduction
One of the most serious complications of decompensated liver cirrhosis is gastroesophageal variceal bleeding, which accounts for 30%–40% of all cirrhosis-related mortality.1–3 Among gastroesophageal varices, esophageal varices are more common than gastric varices2,4; however, gastric varices are associated with a higher mortality rate and an increased risk of bleeding.5,6 The unique vascular anatomy, high blood flow, and deeper submucosal location of gastric varices make bleeding episodes more severe and more challenging to control than those arising from esophageal varices. 7
The endoscopic management of esophagogastric varices includes two primary techniques: endoscopic variceal ligation (EVL) and endoscopic tissue adhesive injection (ETAI).8,9 ETAI requires significant operator expertise and may lead to adverse events such as ectopic embolism and glue expulsion ulcers.8–10 EVL is favored due to its procedural simplicity and low incidence of complications. 11 However, the fixed diameter of EVL ligators limits their effectiveness against larger varices, which restricts their application. 12
To address this limitation, metal clips can be employed in the treatment of varices. These clips exert a mechanical flow-restricting effect. Nonetheless, there are few reports regarding the use of metal clip-assisted endoscopic variceal ligation (MEVL) for gastric varices. Our team has pioneered the incorporation of metal clips in combination with EVL therapy. The current study aims to assess the effectiveness and safety of MEVL in comparison to traditional ligation (TL) methods for managing gastric varices in an elective, non-emergent clinical setting.
Materials and methods
Study design and settings
A non-randomized retrospective cohort analysis was conducted using the hospital records of Henan Provincial People’s Hospital, Henan, China. The study period was from May 2019 to December 2023. The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for observational cohort research 13 ; the completed STROBE checklist is provided as Supplemental Material 1. The study population consisted of adult patients with cirrhosis and esophagogastric varices who were admitted to Henan Provincial People’s Hospital during the study period. Patients who met the eligibility criteria were identified through review of medical records. Ethical approval for the study was obtained from the hospital’s ethics committee. Baseline information was collected for all patients, including demographic characteristics such as age and sex, as well as liver function indicators, including the Child-Pugh classification, hemoglobin, albumin, and coagulation markers.
PICO
Population
Adult patients (⩾18 years) with cirrhosis and gastroesophageal varices (GOV)-type esophagogastric varices who were indicated for EVL.
Intervention
MEVL, where metal clips were applied to blood-supplying vessels before ligation.
Comparator
Traditional endoscopic variceal ligation (TL) without clip assistance.
Outcomes
The primary outcome was one-session eradication, defined as complete variceal eradication achieved after a single index ligation procedure (operational definition in section “Outcomes and operational definitions”). Secondary outcomes were: cumulative (overall) variceal eradication across all sessions, time to eradication, early rebleeding (120 h to 6 weeks), delayed rebleeding (greater than 6 weeks), any rebleeding (cumulative), all-cause mortality, ligation bands deployed per procedure, treatment sessions required to achieve eradication, and adverse events (post-ligation ulcer bleeding, post-operative nausea or vomiting, fever).
Eligibility criteria
Several inclusion and exclusion criteria were followed to recruit the patients. The following are inclusion criteria: (a) age ⩾18 years; (b) diagnosis of cirrhosis with esophagogastric varices based on medical history, clinical manifestations, and auxiliary examinations; (c) GOV-type esophagogastric varices; (d) Esophageal varices indicated for EVL treatment. And, the list of exclusion criteria is as follows: (a) prior endoscopic, interventional, or surgical treatment for esophagogastric variceal bleeding; (b) severe heart, lung, kidney, or other organ dysfunction, making the patient unable to tolerate endoscopy; (c) presence of liver cancer or other malignancies; (d) history of developing another disease during follow-up requiring discontinuation of ligation or switching to other treatments such as endoscopic variceal obturation or transjugular intrahepatic portosystemic shunt (TIPS); (e) gastric variceal diameter >15 mm on contrast-enhanced computed tomography (CT); (f) urgent endoscopic treatment after admission (time from admission to endoscopy ⩽12 h); (g) absence of thoracic or abdominal contrast-enhanced CT prior to endoscopic therapy.
Intervention procedure
Pre-operative preparation
All patients underwent comprehensive pre-treatment evaluation, including complete blood counts, liver and kidney function tests, coagulation profiles, electrolyte panels, electrocardiograms, and contrast-enhanced CT scans of the chest and abdomen. Informed consent was obtained, and the risks associated with endoscopic procedures were explained. Each patient was evaluated by an anesthesiologist and confirmed to be suitable for general anesthesia.
Treatment procedure
Endoscopic assessment
Before ligation, an endoscopic examination was performed to document the location, number, and diameter of gastric varices, as well as the presence of red color signs and thrombus protrusions. The estimated number of required bands was recorded.
Ligation procedure
The ligation device was fitted to the endoscope, and treatment was performed as follows:
Traditional Ligation Group (TL): Sequential dense zig-zag ligation was performed along the lesser curvature, starting below the cardia and extending toward the gastric body until complete ligation of all varices was achieved. 14
Metal Clip-Assisted Ligation Group (MEVL): Feeding vessels supplying each varix were identified based on preoperative contrast-enhanced CT and endoscopic findings. Metal clips were applied to reduce blood flow before ligation. Dense zig-zag ligation was then performed in the same manner as in the TL group.
Adequate suction was applied during ligation to ensure complete aspiration of the varix into the cap, achieving a “full red view” prior to band deployment. When ligation was incomplete or varices were thick, supplementary metal clips were applied at the base of the band to reinforce occlusion. Ligation was continued until varices were obliterated or could no longer be suctioned. Following gastric variceal ligation, dense ligation of esophageal varices was performed upward from the cardia.
Post-operative management
Post-treatment care followed national guidelines for the prevention and treatment of esophagogastric variceal bleeding in portal hypertension. 15 Patients fasted for 48 h and were monitored for adverse events. Prophylactic antibiotic therapy using quinolones or third-generation cephalosporins was administered for a period of 3 days. Continuous intravenous proton pump inhibitor infusion and somatostatin therapy were also given for 3 days.
Follow-up
Patients were followed at 1, 3, and 6 months after the initial treatment and then annually. The follow-up assessment included laboratory testing, gastroscopy, and an abdominal contrast-enhanced CT scan. If residual varices were identified, additional ligation sessions were performed until eradication was achieved. Follow-up endpoints included rebleeding, death, or transition to alternative treatments such as tissue adhesive injection, sclerotherapy, liver transplantation, TIPS, or surgery.
Outcomes
The study evaluated both efficacy and safety outcomes related to the management of gastroesophageal varices. The primary outcome was one-session eradication (complete variceal eradication after a single index ligation procedure). Secondary outcomes included the number of ligation bands used during the procedure, the number of treatment sessions required to achieve eradication, the incidence of rebleeding, mortality, and procedure-related adverse events, including post-ligation bleeding.
Complete eradication was defined as the absence of visible varices on follow-up endoscopy, with no red color signs and no requirement for further endoscopic intervention at the time of assessment. Eradication was defined as a marked reduction in variceal size such that no additional immediate ligation was required, although minimal residual varices may still be present.
The number of ligation bands refers to the total number of bands applied during the initial endoscopic procedure. The number of treatment sessions was defined as the total number of endoscopic sessions required to achieve eradication of gastric varices. Post-ligation bleeding was defined as clinically evident upper gastrointestinal bleeding occurring within 14 days after the index procedure, confirmed by endoscopic evaluation as originating from post-ligation ulcers or residual varices. Clinical evidence of bleeding included hematemesis, melena, or a decrease in hemoglobin of at least 2 g/dL. Rebleeding was defined as any episode of recurrent upper gastrointestinal bleeding after initial hemostasis during the follow-up period, confirmed to be variceal in origin by endoscopic assessment and excluding non-variceal sources. Mortality was defined as all-cause death occurring during the follow-up period. All outcomes were assessed during scheduled follow-up visits at 1, 3, and 6 months after the initial procedure based on clinical records, laboratory findings, and endoscopic evaluation.
Medical equipment used in the intervention
All endoscopic procedures were performed using a standard diagnostic gastroscope (Olympus, Tokyo, Japan). Variceal ligation was carried out with either the Speedband Superview Super 7™ multiple band ligator (Boston Scientific, Marlborough, Massachusetts, USA) or the Six Shooter Saeed Multi-Band Ligator (Cook Medical, Bloomington, Indiana, USA), based on the availability and operator preference. Metal clips used for flow-restriction and vessel occlusion were supplied by either Hangzhou AGS MedTech Co., Ltd. (Zhejiang Province) or MicroPort Scientific Corporation (Shanghai), both located in China. All equipment was used in accordance with the manufacturer’s guidelines and standard clinical practice.
Outcomes and operational definitions
The primary outcome was one-session eradication, defined as complete eradication achieved after a single index procedure. Complete eradication was defined as the absence of residual variceal columns with red-colored signs on follow-up endoscopy. Secondary outcomes were: overall venous eradication (cumulative across sessions), early rebleeding (clinically evident upper gastrointestinal bleeding occurring between 120 h, i.e., 5 days, and 6 weeks post-procedure), delayed rebleeding (clinically evident bleeding more than 6 weeks post-procedure), any rebleeding (early or delayed), all-cause mortality, and adverse reactions (any procedure-attributable clinical event within 30 days).
Non-selective beta-blocker co-therapy
All patients in both groups received non-selective beta-blocker (NSBB) therapy (propranolol, nadolol, or carvedilol) titrated to the maximally tolerated dose, consistent with the 2023 guideline for management of esophagogastric variceal bleeding in cirrhotic portal hypertension published jointly by the Chinese Society of Hepatology, the Chinese Society of Gastroenterology, and the Chinese Society of Digestive Endoscopology. 14
Operator disclosure
All procedures in both the MEVL and the control (TL) groups were performed by the same attending endoscopist, Dr. Ding Hui, assisted by Wang Yi and Li Zhenjuan.
Procedural details and technical outcomes
Anatomical clip landmarks were (i) the base of the dominant varix column, (ii) feeder-vessel sources identified on preoperative contrast-enhanced CT, and (iii) submucosal arterial branches visible endoscopically. The number of through-the-scope metal hemoclips deployed per procedure was determined by operator judgment based on CT feeder-vessel mapping and intraprocedural visualization; supplementary clips were placed if initial occlusion was incomplete (median 0, interquartile range (IQR) 0–3 in the MEVL group). Technical success was pre-defined as completion of the index-procedure band deployment without intraoperative conversion to an alternative modality; technical success was achieved in 46 of 46 (100%) MEVL and 53 of 53 (100%) TL procedures. For each MEVL procedure, pre-ligation feeder-vessel hemoclips were applied to all identified anatomical clip landmarks ((i) base of the dominant varix column, (ii) feeder-vessel sources on preoperative contrast-enhanced CT, (iii) submucosal arterial branches visible endoscopically) as a defining step of the technique; the precise per-patient count of these pre-ligation hemoclips was not captured in the structured procedural record. Only supplementary band-reinforcement clips deployed at the band base after band placement when occlusion was incomplete were tabulated separately. These supplementary clips, reported in Table 3, had a median (IQR) of 0 (0–3) in MEVL versus 0 (0–0) in TL.
Data analysis
All baseline comparisons were performed using SPSS version 26 (IBM, New York, USA). Since this was a non-randomized retrospective cohort study, propensity score matching (PSM) was utilized to minimize baseline differences between the two treatment groups. Covariate balance before and after matching was evaluated using standardized mean differences (SMD); an SMD value less than 0.10 was considered indicative of good covariate balance. The propensity score model included age, sex, Child-Pugh class, Sarin subtype, INR, and CT-derived variceal diameter. 1:1 nearest-neighbor matching was performed with a caliper of 0.2 times the standard deviation of the logit of the propensity score (caliper = 0.28), without replacement. Inverse probability of treatment weighting (IPTW) with stabilized weights truncated at the 99th percentile was performed in parallel and was pre-specified as the primary balancing method; PSM is reported as a sensitivity analysis. IPTW achieved a maximum residual |SMD| of 0.143 (INR); PSM achieved a maximum residual |SMD| of 0.196 (Sarin subtype).
Statistical testing used the Mann–Whitney U test for ranked data, the Chi-square or Fisher’s exact test for categorical variables as appropriate, and independent-samples t-tests for normally distributed continuous variables. A two-sided p-value of less than 0.05 was considered statistically significant.
Multivariable logistic regression adjusting for the propensity score covariates, PSM-adjusted logistic regression on matched pairs, and IPTW-weighted logistic regression were used for binary outcomes (one-session eradication, any rebleeding, mortality, adverse reactions). Time-to-eradication, time-to-rebleeding, and time-to-death were analyzed by Cox proportional hazards (PHs) regression; the PHs assumption was examined using scaled Schoenfeld residuals. Pre-specified subgroup analyses by Sarin class (GOV1, GOV2) and a treatment-by-subtype interaction test were performed. A temporal sensitivity analysis using era strata (May 2019–October 2021 vs October 2021–December 2023) and a treatment-by-era interaction test were performed to assess calendar-time confounding. Post hoc power was calculated at alpha = 0.05 for each endpoint. Multivariable models, survival analyses, balance diagnostics, and power calculations were performed in Python 3.11 (statsmodels 0.14, lifelines 0.27, scipy 1.11).
Sensitivity analyses
The INR of one MEVL patient was recorded as 13.9, a value considered clinically implausible. Primary and secondary analyses were repeated with this observation excluded; conclusions were unchanged. The cohort INR is reported as median with IQR rather than as mean ± SD to reduce distortion by outliers.
Time-to-eradication Cox specification
The time origin (t = 0) was the date of the index ligation procedure. The event was first documented as complete variceal eradication, defined operationally as the absence of residual variceal columns with red color signs on follow-up endoscopy. Patients with eradication confirmed on the immediate post-index endoscopy (i.e., complete eradication apparent at the index session and validated at the first scheduled follow-up endoscopy) were assigned the date of that first follow-up endoscopy as the event time; a pre-specified sensitivity analysis assigning t = 0.5 days to such patients yielded materially identical effect estimates. Patients who did not achieve documented eradication during follow-up were administratively censored at the date of their last follow-up endoscopy. Patients lost to follow-up before any post-index endoscopy were censored at the date of last clinical contact. Adjustment covariates were age, Child-Pugh score, and CT-derived gastric variceal diameter, pre-specified. The proportional hazards assumption was tested by scaled Schoenfeld residuals; the global PH test was non-significant for the eradication model (p = 0.552, Table 4).
Results
A total of 99 cirrhotic patients with gastric varices were included in this study, identified from a pool of 132 records that met the pre-specified inclusion and exclusion criteria; selection into the analytic cohort was based on those eligibility criteria alone, not on PSM. Of the 33 excluded patients, 8 reported severe major organ dysfunction, 13 reported some other malignancies, 9 reported a need for urgent endoscopic intervention, and 2 patients discontinued the treatment procedure (Figure 1). PSM and IPTW were subsequently applied as analytical methods to balance baseline covariates between the MEVL and TL treatment groups for inferential analyses. Selection criteria were derived from the medical records of patients who met the inclusion and exclusion criteria and were admitted to the hospital between May 2019 and December 2023. The patients were divided into two groups for the study: the MEVL group (n = 46) and the TL group (n = 53).
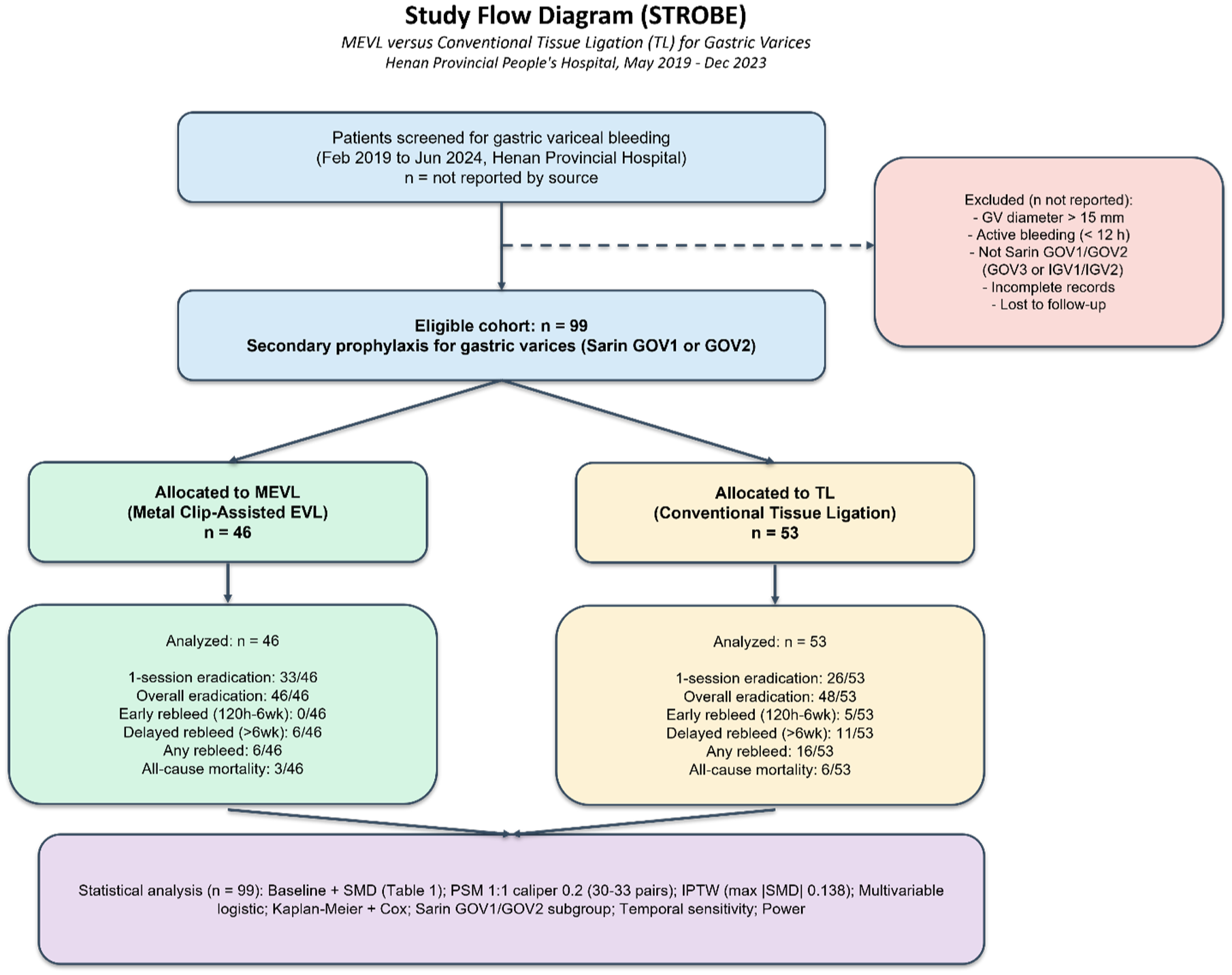
STROBE flow diagram. Flow of 132 screened records through 33 pre-specified exclusions to the final analytic cohort of 99 patients (46 MEVL, 53 TL).
Table 1 depicts the characteristics of the study participants. The proportion of male patients was similar in both groups (60.9% vs 69.8%; p = 0.470) and vice versa to their female counterparts. The mean age was 53.8 ± 12.9 years in the MEVL group versus 51.5 ± 11.6 years in the TL group (p = 0.344). Hematologic and coagulation parameters were comparable: mean hemoglobin 93.1 ± 20.9 versus 94.6 ± 24.2 g/L (p = 0.740); median platelet count 73 × 109/L (IQR 50–100) versus 72 × 109/L (IQR 54–95) (p = 0.652); median prothrombin time 14.6 s (IQR 13.5–16.1) versus 14.5 s (IQR 13.8–15.6; p = 0.588); and median INR 1.22 (IQR 1.09–1.34) versus 1.22 (IQR 1.08–1.38; p = 0.319). Liver function indices were also similar: median total bilirubin 18.4 µmol/L (IQR 12.1–24.9) versus 16.0 µmol/L (IQR 10.4–24.2; p = 0.457); and mean albumin 35.1 ± 5.6 vs 35.5 ± 5.7 g/L (p = 0.705). The distribution of Child-Pugh classes was similar between the MEVL and TL groups: Class A (65.2% vs 54.7%), Class B (32.6% vs 39.6%), and Class C (2.2% vs 5.7%), with no statistically significant difference (p > 0.05). Renal function parameters did not differ significantly, including blood urea nitrogen (5.71 ± 3.24 vs 5.12 ± 2.72 mmol/L; p = 0.330) and serum creatinine (59.3 ± 10.9 vs 55.6 ± 11.6 µmol/L; p = 0.106). Portal hypertension-related features were comparable. Ascites was present in 50.0% of MEVL and 64.2% of TL patients (p = 0.224). Portal vein thrombosis was present in 21.7% and 22.6% of patients, respectively (p = 1.000), and hepatic encephalopathy was rare in both groups (0% vs 1.9%; p = 1.000). Severe esophageal varices were present in 91.3% of the MEVL group and 94.3% of the TL group, while moderate varices were present in 8.7% and 5.7%, respectively (p = 0.846). Endoscopic assessment demonstrated similar variceal severity. Red wale markings were present in 97.8% and 94.3% of patients, respectively (p = 0.714). Mean gastric variceal diameter on CT was 12.21 ± 1.87 mm in the MEVL group and 11.72 ± 1.50 mm in the TL group (p = 0.166). The etiology of cirrhosis was also comparable. Hepatitis B virus infection was the most common cause (69.6% vs 62.3%), followed by hepatitis C virus (13.0% vs 9.4%), alcoholic liver disease (4.3% vs 13.2%), autoimmune liver disease (6.5% vs 3.8%), and cryptogenic cirrhosis (6.5% vs 11.3%), with no statistically significant differences between groups (all p > 0.05). Overall, no statistically significant differences were observed for any baseline variable. Median follow-up was 34 months (IQR 18–54 months).
Baseline characteristics of patients treated with MEVL versus conventional TL.
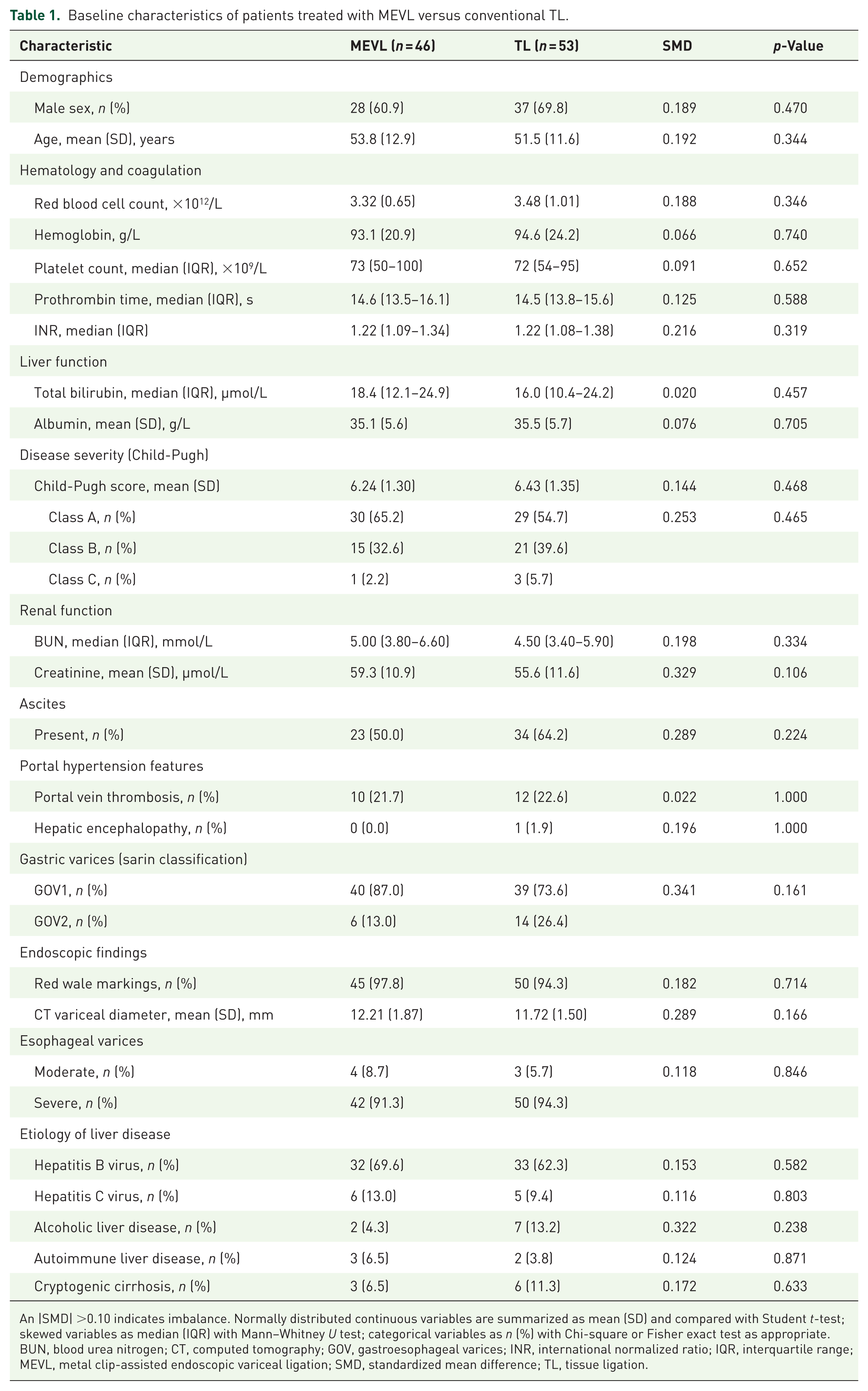
An |SMD| >0.10 indicates imbalance. Normally distributed continuous variables are summarized as mean (SD) and compared with Student t-test; skewed variables as median (IQR) with Mann–Whitney U test; categorical variables as n (%) with Chi-square or Fisher exact test as appropriate.
BUN, blood urea nitrogen; CT, computed tomography; GOV, gastroesophageal varices; INR, international normalized ratio; IQR, interquartile range; MEVL, metal clip-assisted endoscopic variceal ligation; SMD, standardized mean difference; TL, tissue ligation.
Table 2 presents a comparison of clinical and adverse outcomes between TL and MEVL. Complete (one-session) eradication was achieved in 33 of 46 (71.7%) patients in the MEVL group, compared with 26 of 53 (49.1%) in the TL group (unadjusted odds ratio (OR) 2.64, 95% confidence interval (CI) 1.14–6.09; Fisher exact p = 0.025; multivariable-adjusted OR 3.16, 95% CI 1.25–8.01; p = 0.015; IPTW-adjusted OR 2.55, 95% CI 1.03–6.27; p = 0.042; adjusted Cox hazard ratio (HR) 1.53, 95% CI 1.00–2.35; p = 0.049). Early rebleeding between 120 h and 6 weeks occurred in 0 of 46 (0.0%) MEVL patients versus 5 of 53 (9.4%) TL patients (OR 0.09, 95% CI 0.01–1.76; p = 0.059; post hoc power 87%). Post-ligation bleeding did not differ significantly between groups (Fisher’s exact p = 0.121). All-cause mortality was 3 of 46 (6.5%) in the MEVL group and 6 of 53 (11.3%) in the TL group (Fisher’s exact p = 0.498; adjusted Cox HR 0.83, 95% CI 0.19–3.57; p = 0.800); the mortality analysis was underpowered (post hoc power 14%). Patients in the MEVL group required fewer gastric ligation bands and fewer sessions to achieve eradication (see Table 3 for numeric breakdown with p-values). Flow-restriction metal clips were used exclusively in the MEVL group (median 0, IQR 0–3), while the TL group required none (p < 0.001, Mann–Whitney U test).
Efficacy outcomes comparing MEVL with TL.
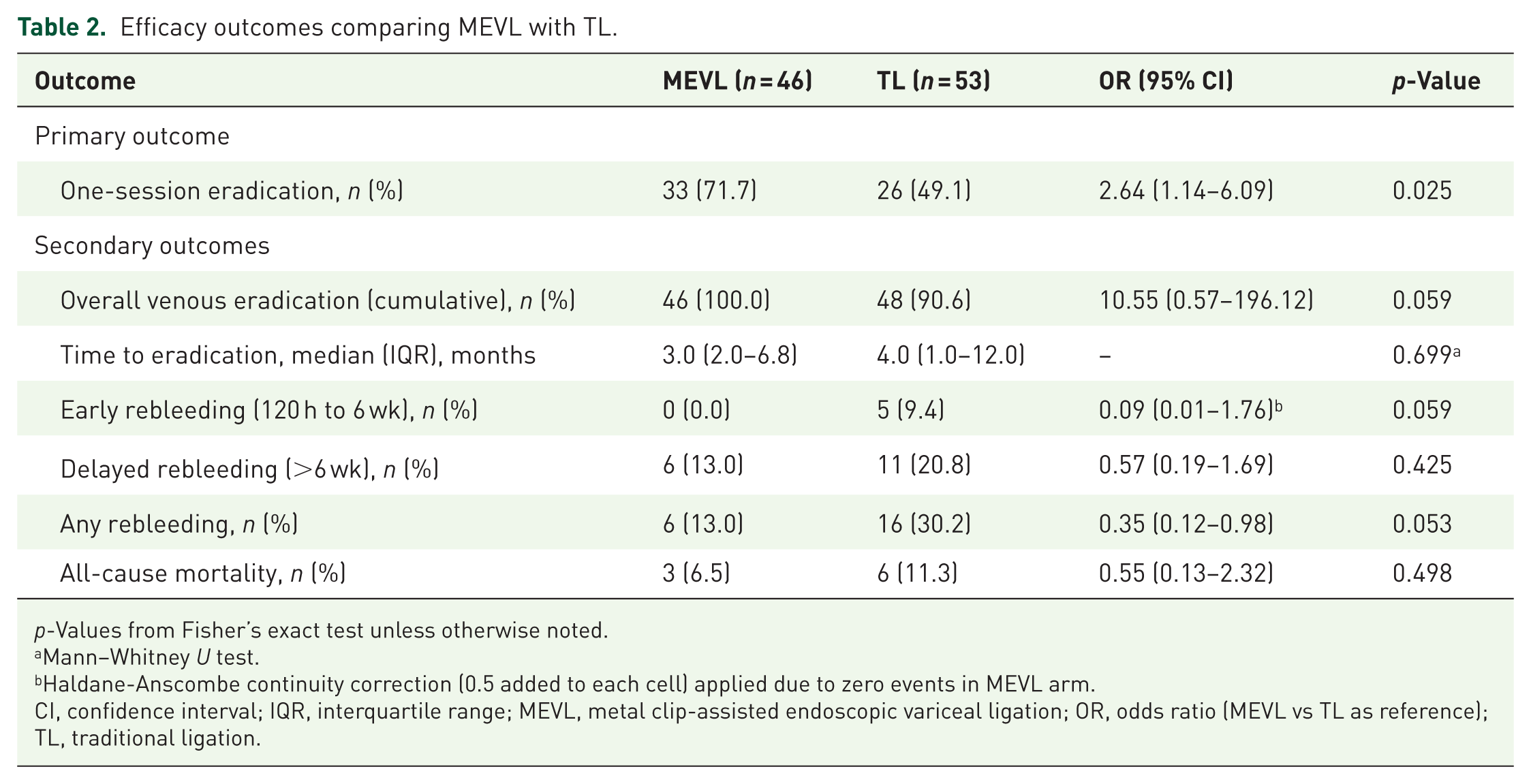
p-Values from Fisher’s exact test unless otherwise noted.
Mann–Whitney U test.
Haldane-Anscombe continuity correction (0.5 added to each cell) applied due to zero events in MEVL arm.
CI, confidence interval; IQR, interquartile range; MEVL, metal clip-assisted endoscopic variceal ligation; OR, odds ratio (MEVL vs TL as reference); TL, traditional ligation.
Safety and procedural outcomes.
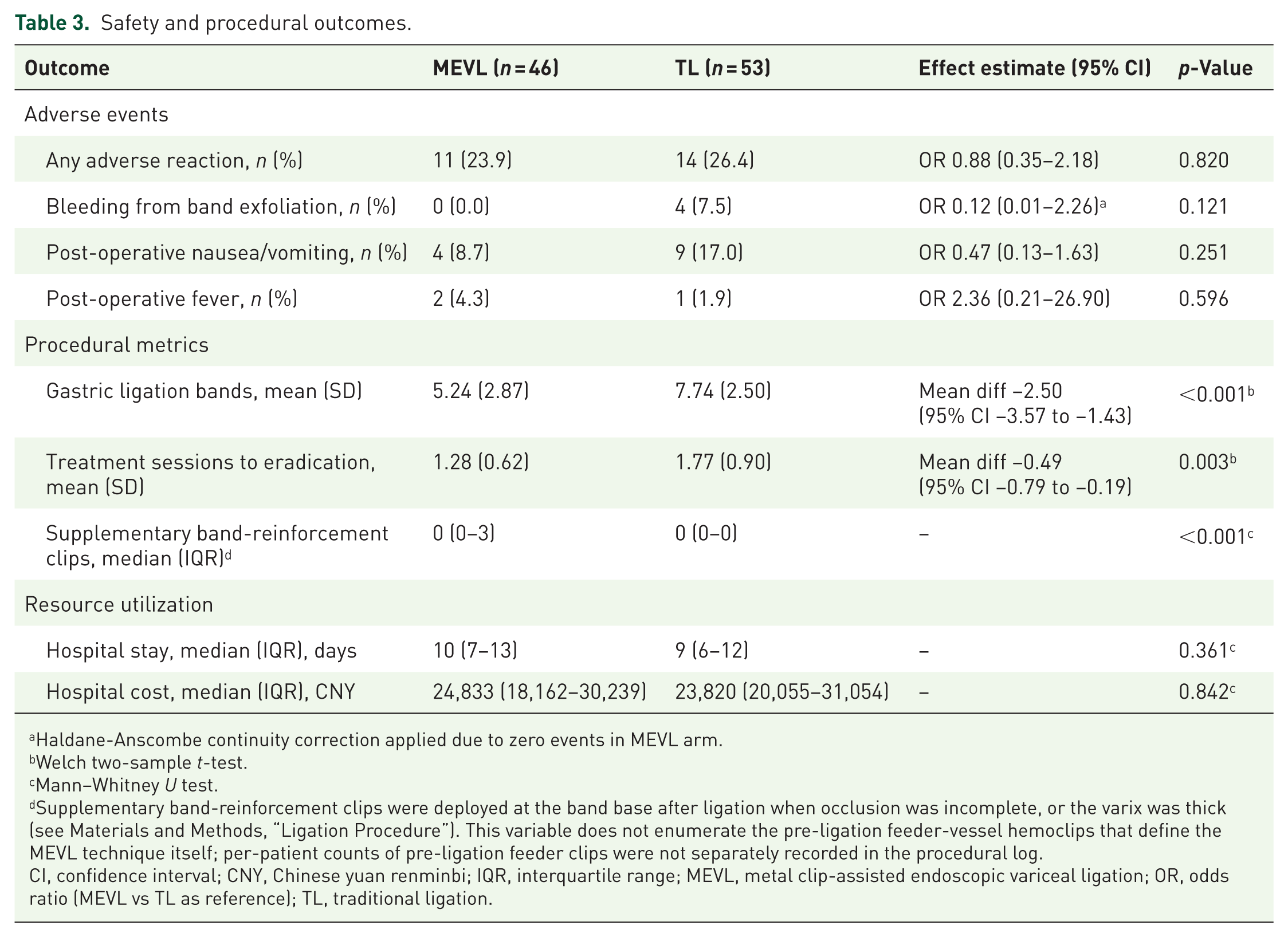
Haldane-Anscombe continuity correction applied due to zero events in MEVL arm.
Welch two-sample t-test.
Mann–Whitney U test.
Supplementary band-reinforcement clips were deployed at the band base after ligation when occlusion was incomplete, or the varix was thick (see Materials and Methods, “Ligation Procedure”). This variable does not enumerate the pre-ligation feeder-vessel hemoclips that define the MEVL technique itself; per-patient counts of pre-ligation feeder clips were not separately recorded in the procedural log.
CI, confidence interval; CNY, Chinese yuan renminbi; IQR, interquartile range; MEVL, metal clip-assisted endoscopic variceal ligation; OR, odds ratio (MEVL vs TL as reference); TL, traditional ligation.
Propensity score balance
The primary 1:1 nearest-neighbor PSM model (caliper 0.2 × SD of the logit propensity score, no replacement) yielded 33 matched pairs (66 patients) for analyses of one-session eradication and overall eradication where complete follow-up was available. Endpoint-specific PSM samples were 33 pairs for eradication endpoints, 32 pairs for any rebleeding (one matched pair excluded due to follow-up shorter than the 120-h rebleeding window), and 31 pairs for all-cause mortality (two matched pairs were excluded for incomplete vital-status follow-up). The range “31–33 matched pairs” therefore reflects per-endpoint analytic samples rather than a single matched cohort (Figure 2). Maximum |SMD| after PSM was 0.196 (Sarin subtype). IPTW with stabilized weights truncated at the 99th percentile reduced the maximum |SMD| to 0.143 and was pre-specified as the primary balancing method.
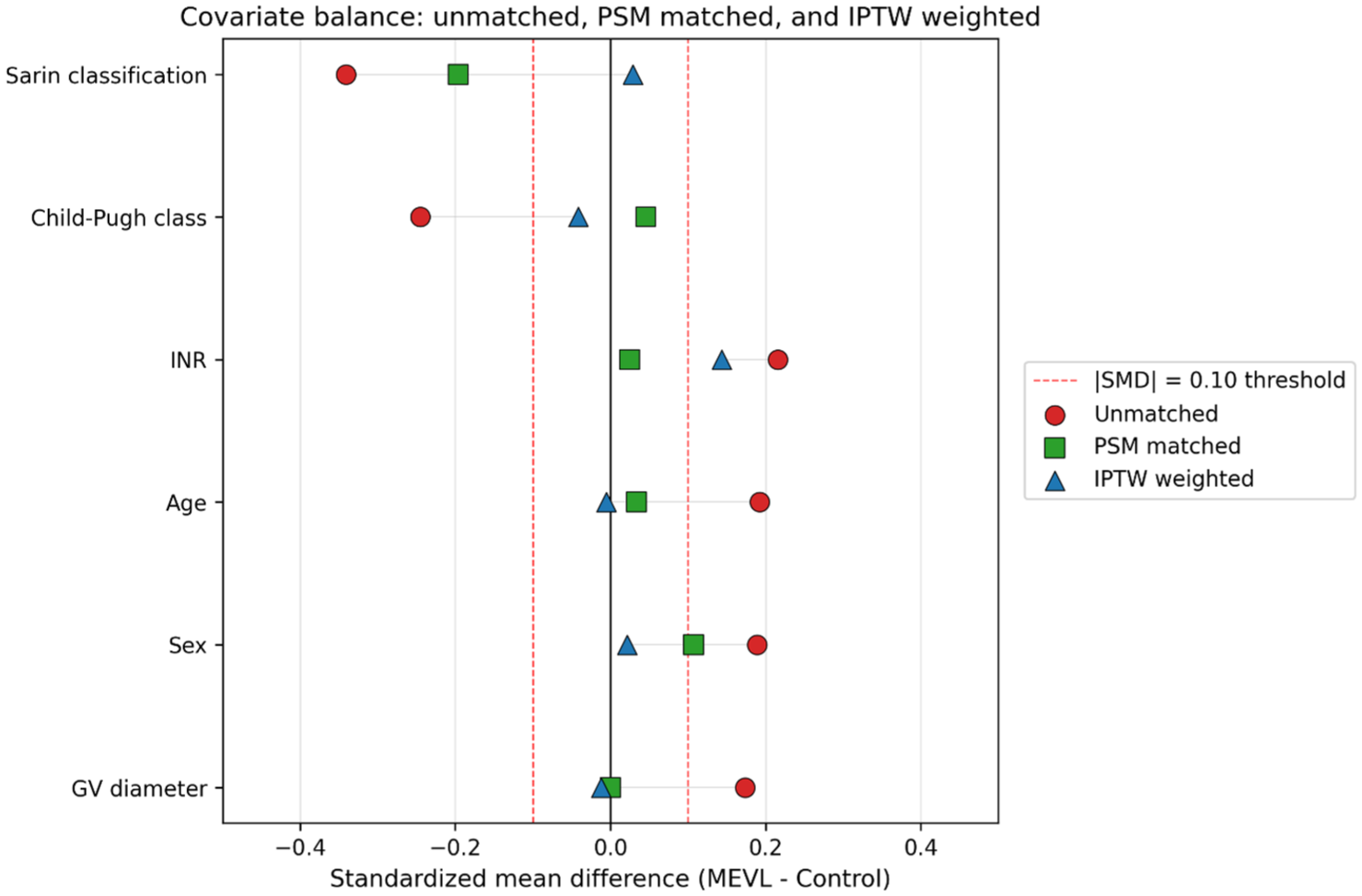
Love plot of SMDs. Covariate balance for age, sex, Child-Pugh class, Sarin subtype, INR, and CT-derived variceal diameter under three states (unmatched, 1:1 PSM, IPTW). IPTW was pre-specified as the primary balancing method and achieved the smallest maximum |SMD| (0.143).
Primary outcome: Adjusted analyses
Results for the primary outcome (one-session eradication) were consistent across five analytical approaches: unadjusted (OR 2.64, 95% CI 1.14–6.09; Fisher p = 0.025), multivariable-adjusted logistic regression (OR 3.16, 95% CI 1.25–8.01; p = 0.015), PSM-adjusted logistic regression (OR 2.94, 95% CI 0.96–9.00; p = 0.059), IPTW-weighted logistic regression (OR 2.55, 95% CI 1.03–6.27; p = 0.042), and Cox regression for time-to-first-eradication (adjusted HR 1.53, 95% CI 1.00–2.35; p = 0.049; Tables 4 and 5). The PHs assumption was not violated. Kaplan–Meier curves for time-to-eradication, time-to-any-rebleeding, and time-to-death are shown in Figure 3(a)–(c).
Cox PHs analysis for key time-to-event endpoints.
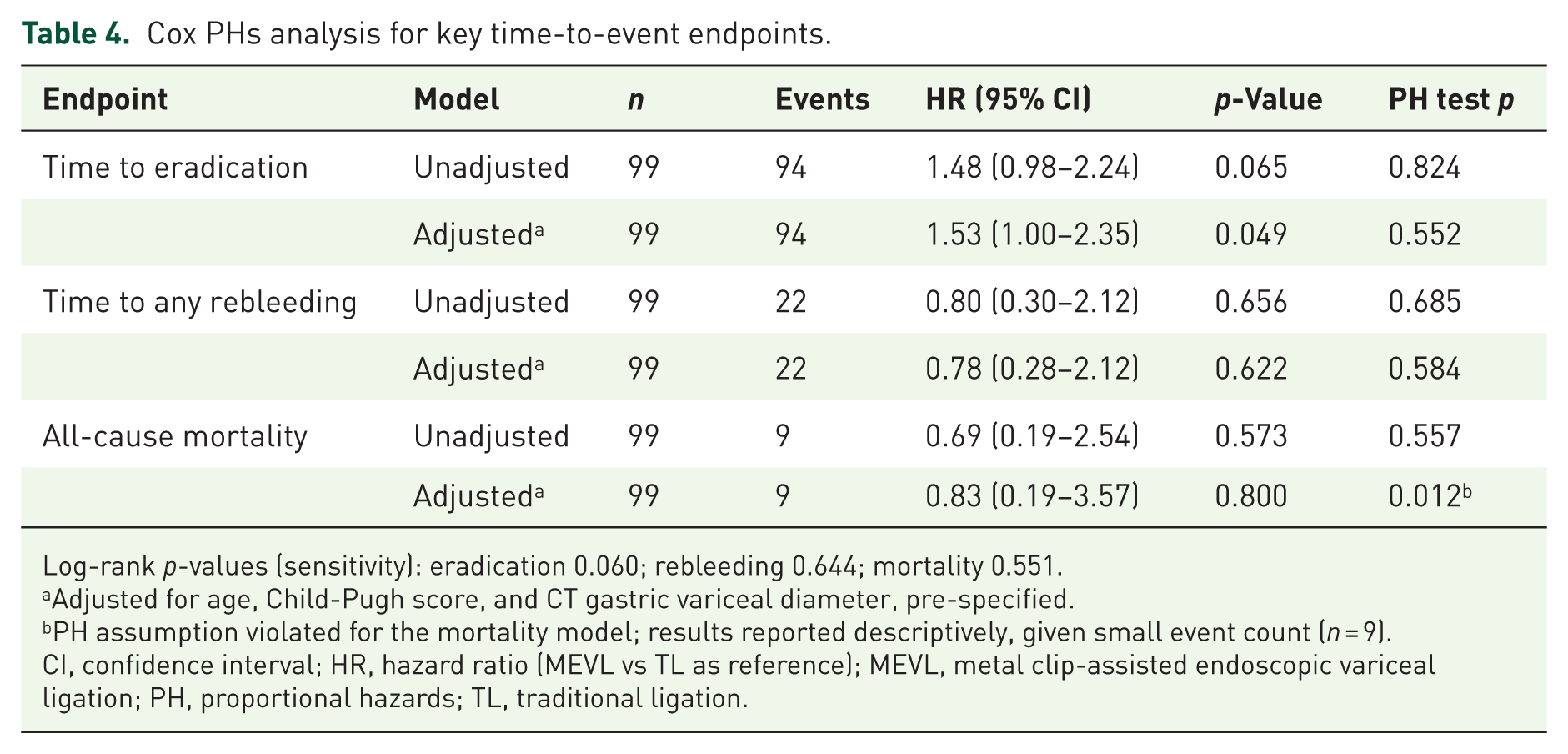
Log-rank p-values (sensitivity): eradication 0.060; rebleeding 0.644; mortality 0.551.
Adjusted for age, Child-Pugh score, and CT gastric variceal diameter, pre-specified.
PH assumption violated for the mortality model; results reported descriptively, given small event count (n = 9).
CI, confidence interval; HR, hazard ratio (MEVL vs TL as reference); MEVL, metal clip-assisted endoscopic variceal ligation; PH, proportional hazards; TL, traditional ligation.
Sensitivity analyses: adjusted estimates across five statistical approaches.
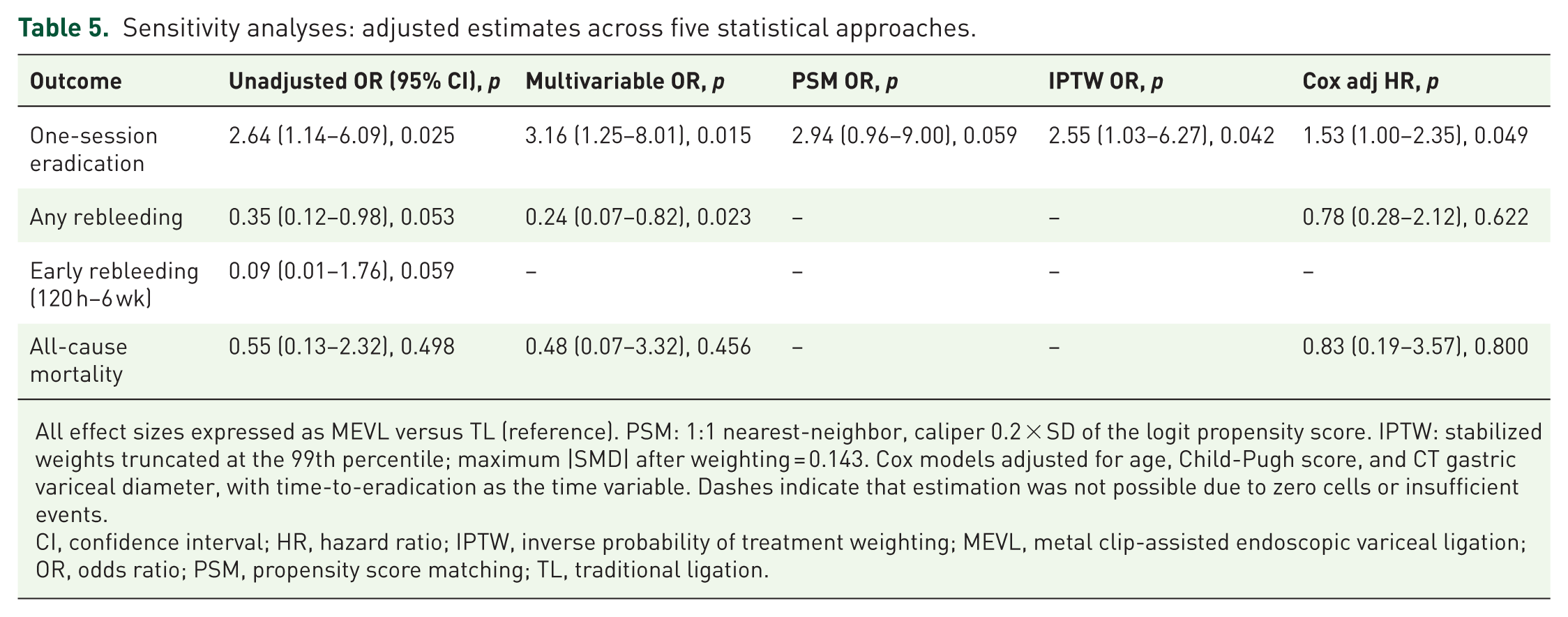
All effect sizes expressed as MEVL versus TL (reference). PSM: 1:1 nearest-neighbor, caliper 0.2 × SD of the logit propensity score. IPTW: stabilized weights truncated at the 99th percentile; maximum |SMD| after weighting = 0.143. Cox models adjusted for age, Child-Pugh score, and CT gastric variceal diameter, with time-to-eradication as the time variable. Dashes indicate that estimation was not possible due to zero cells or insufficient events.
CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; MEVL, metal clip-assisted endoscopic variceal ligation; OR, odds ratio; PSM, propensity score matching; TL, traditional ligation.
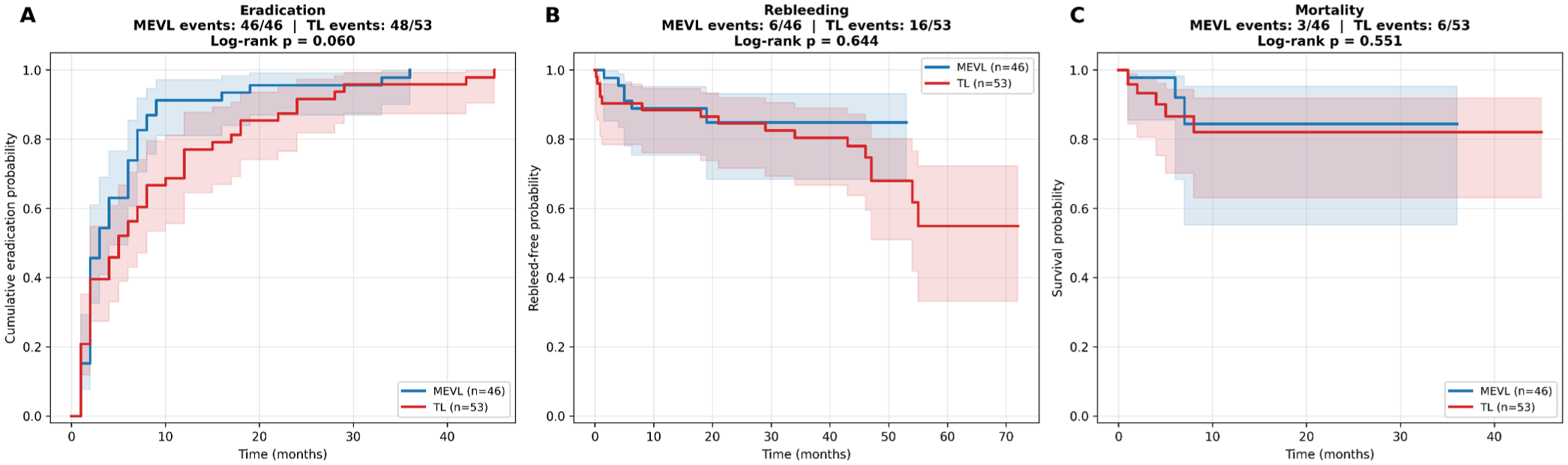
Kaplan–Meier curves. (a) Cumulative one-session eradication probability (log-rank p = 0.060). (b) Time to any rebleeding (log-rank p = 0.644). (c) All-cause mortality (log-rank p = 0.551).
Reconciliation of logistic and Cox results for rebleeding
Logistic regression showed a reduction in the cumulative risk of any rebleeding with MEVL (adjusted OR 0.24, 95% CI 0.07–0.82; p = 0.023), while Cox regression showed no difference in hazard among patients who experienced a rebleed (HR 0.78, 95% CI 0.28–2.12; p = 0.622; Table 4). These findings are complementary: MEVL prevents more patients from ever rebleeding, but does not meaningfully delay the timing of rebleeding among those who eventually do.
Sarin subgroup analysis
In the GOV1 subgroup (n = 79), MEVL was associated with higher odds of one-session eradication (adjusted OR 3.88, 95% CI 1.49–10.09; p = 0.006; Table 6). In the GOV2 subgroup (n = 20), the point estimate did not reach significance (OR 0.56, 95% CI 0.08–3.86; p = 0.642); this subgroup is underpowered. The treatment-by-subgroup interaction term was not significant (p = 0.078), indicating a non-significant trend toward effect modification that does not support differential conclusions across Sarin strata.
Pre-specified Sarin-class subgroup analysis for one-session eradication and any rebleeding, comparing MEVL with TL.
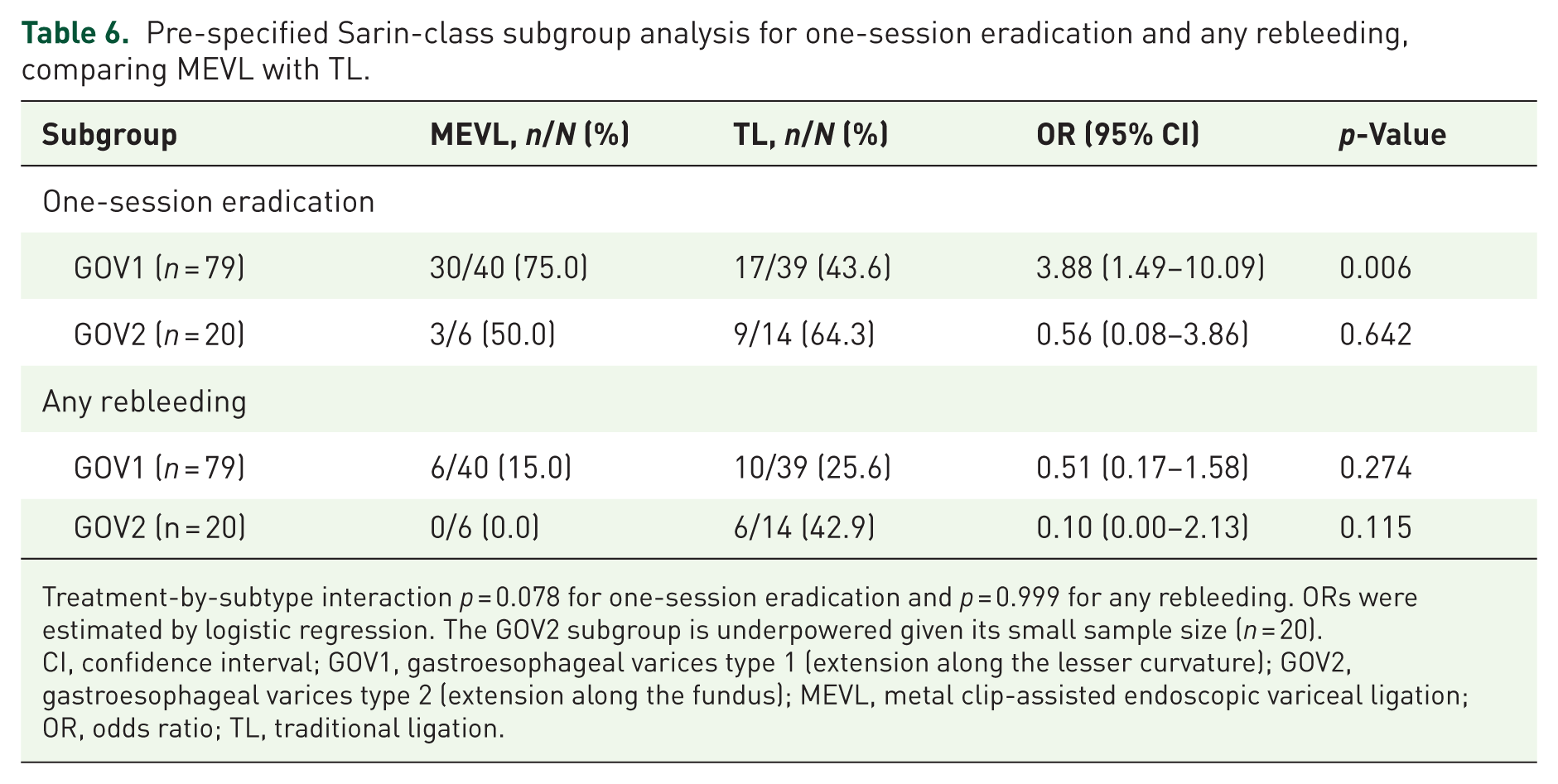
Treatment-by-subtype interaction p = 0.078 for one-session eradication and p = 0.999 for any rebleeding. ORs were estimated by logistic regression. The GOV2 subgroup is underpowered given its small sample size (n = 20).
CI, confidence interval; GOV1, gastroesophageal varices type 1 (extension along the lesser curvature); GOV2, gastroesophageal varices type 2 (extension along the fundus); MEVL, metal clip-assisted endoscopic variceal ligation; OR, odds ratio; TL, traditional ligation.
Temporal sensitivity analysis
The median procedure date was October 12, 2021. In the early era (May 2019–October 2021, n = 50), 44 of 50 procedures were TL and 6 were MEVL; in the late era (October 2021–December 2023, n = 49), 9 of 49 were TL and 40 were MEVL. The Chi-square test for group-by-era association was highly significant (p < 0.001), reflecting progressive adoption of MEVL rather than random allocation. The treatment-by-era interaction term for one-session eradication was not significant (p = 0.254), and the direction of effect was consistent across eras. Residual time-varying confounding cannot be fully excluded.
Post hoc power
Power calculations at alpha = 0.05 for the observed effect sizes were: 64% for one-session eradication (requiring n = 72 per arm for 80% power), 87% for overall eradication, 87% for early rebleeding, 56% for any rebleeding (requiring n = 88 per arm for 80% power), 14% for mortality (requiring n = 545 per arm for 80% power), and 6% for adverse reactions. The study is adequately powered only for the eradication and early-rebleeding endpoints.
Absolute risk measures and numbers needed to treat
For the primary outcome of one-session eradication, the absolute risk difference favoring MEVL was 22.68 percentage points (95% CI 3.96–41.40; number needed to treat (NNT) = 5). Overall venous eradication differed by 9.43 percentage points (95% CI 1.56–17.30; NNT = 11). For safety endpoints, the absolute risk difference for early rebleeding (120 h–6 weeks) was −9.43 percentage points (95% CI −17.30 to −1.56; NNT to prevent one early rebleed = 11), and the absolute risk difference for any rebleeding was −17.15 percentage points (95% CI −32.88 to −1.41; NNT = 6). For all-cause mortality, the absolute risk difference of −4.80 percentage points (95% CI −15.92 to +6.32) included zero within the 95% CI, so a reliable NNT is not reported.
Discussion
In this propensity score-matched retrospective comparative cohort study, a comparison between the clinical effectiveness and safety of MEVL with TL in patients with cirrhosis and gastric varices was observed. A total of 99 patients were included, and the main findings were that MEVL achieved a significantly higher one-session eradication rate (with comparable overall cumulative eradication), required fewer ligation bands, and fewer treatment sessions to achieve eradication compared with the TL group. These results suggest that using the MEVL technique may enhance the technical success of gastric variceal ligation.
In this study, the baseline characteristics of the included participants were comparable between the MEVL and TL groups following PSM. This allowed to produce a more reliable comparison of treatment outcomes, which has reduced the possibility of selection bias in the population group.16,17 The indicators related to endoscopic technique or procedures also supported greater technical efficiency with MEVL. Patients in the MEVL group required fewer gastric and esophageal ligation bands to reach eradication compared to the TL group. Although this study was not designed to evaluate the health-economic benefits of this technique, it may have demonstrated that reducing the number of bands and procedures is a resource-efficient approach. 18 Regarding the safety outcomes, the rate of any rebleeding was lower in the MEVL group after multivariable adjustment (adjusted OR 0.24, 95% CI 0.07–0.82; p = 0.023). All-cause mortality was 6.5% versus 11.3%; the mortality comparison did not reach statistical significance and was underpowered (post hoc power 14%). A recent individual patient data meta-analysis of endovascular and endoscopic interventions for gastric variceal hemorrhage 19 reported pooled any-rebleeding rates of approximately 25%–35% across conventional endoscopic approaches, broadly consistent with the TL arm of the present cohort (30.2%). The reduction in cumulative rebleeding observed with MEVL (13.0%) situates the technique favorably against this contemporary benchmark, while reinforcing that prospective multicenter head-to-head validation is still needed.
Previous studies have reported EVL to be less effective in gastric varices compared with esophageal varices, often citing incomplete variceal capture and mechanical slippage as key limitations.4,20 More recently, a few studies have described the use of additional clips or combined clipping and adhesive injection, which has been found to reduce rebleeding and embolic complications in reports.21,22 However, most of these studies were single-center, non-comparative, or limited by heterogeneous inclusion criteria. Since this study was a retrospective study, the lack of data on NSBB use is an important limitation, as NSBB therapy is known to influence bleeding risk and may have confounded the observed outcomes. In addition, Patients with acute upper gastrointestinal bleeding requiring urgent endoscopy were excluded from the study, which raises concerns about the generalizability of the findings. The identification of feeding vessels was based on a combination of CT interpretation and endoscopic judgment, which may introduce operator-dependent variability and limit reproducibility. In addition, detailed procedural metrics such as clip placement success rate, procedure time, and clip-specific adverse events were not systematically recorded. Outcome assessment was not blinded, which may introduce observer bias, particularly for subjective endpoints such as variceal eradication.
This study has several strengths. These include a clearly defined specific patient cohort, balancing of baseline differences through PSM and IPTW, and pre-specified operational definitions with adjusted estimates and 95% CIs, which improves their interpretability.
Limitations
Several limitations must be acknowledged. First, this is a single-center retrospective observational study, which limits generalizability and precludes causal inference. Although we applied multivariable adjustment, PSM, and IPTW, residual confounding by unmeasured variables cannot be excluded.
Second, the cohort comprised patients undergoing elective EVL for either primary or secondary prophylaxis of gastric variceal bleeding, with urgent endoscopy (time from admission to endoscopy ⩽12 h) excluded. Prior bleeding history was not separately coded in the retrospective source records at a level sufficient to stratify findings by prophylaxis indication, and applicability to pure primary-prophylaxis or pure secondary-prophylaxis subcohorts cannot be inferred from these data.
Third, the cohort contained only Sarin GOV1 and GOV2 patients; no GOV3, IGV1, or IGV2 patients were included. The generalizability of these results to isolated gastric varices and to fundal varices with cardio-fundal extension is therefore unknown and should not be inferred from the present data.
Fourth, allocation was severely imbalanced across calendar time (treatment-by-era Chi-square p less than 0.001), reflecting progressive institutional adoption of MEVL after 2021. While pre-specified treatment-by-era interaction tests were not significant and effect directions were consistent across eras, residual time-varying confounding from changes in supportive care, infection prophylaxis, or referral pathways cannot be fully excluded. The effect estimate reported here, therefore, reflects the combined effect of the MEVL technique and of the calendar-time period in which it was adopted; because all procedures were performed by a single operator, within-operator learning over time cannot be separated from secular trends in care. The causal effect of the MEVL technique cannot be fully identified from these data, and the observed benefit should not be interpreted as a technique-only effect. A contemporaneous multicenter randomized trial with multiple operators is required to provide an identifiability-clean estimate.
Fifth, the study is underpowered for several clinically important endpoints. Post hoc power for mortality was 14% and for adverse reactions was 6%; null findings for these endpoints should not be interpreted as evidence of equivalence or non-inferiority. An adequately powered assessment of mortality would require approximately 545 patients per arm.
Sixth, the overall sample size is modest (n = 99), which limits precision for subgroup analyses. In particular, the GOV2 subgroup (n = 20) is not adequately powered to detect or exclude a clinically relevant effect.
Seventh, endoscopic assessment of eradication was performed in the course of routine care and was not blinded to treatment allocation. Retrospective chart review introduces the possibility of ascertainment bias, although the operational definition of complete eradication (absence of residual variceal columns with red color signs) is standard and was applied uniformly.
Eighth, all procedures were performed by the same attending endoscopist, which is a methodological strength because it eliminates inter-operator variability. However, learning over time within a single operator cannot be fully disentangled from the calendar-time effect described above; the operator’s technical proficiency with MEVL may have increased as adoption progressed, contributing to a within-operator learning curve that is confounded with era. Prospective multicenter studies with multiple operators and randomized allocation are required to address this limitation definitively.
Conclusion
In this single-center retrospective cohort of selected elective GOV1/GOV2 patients, MEVL was associated with a higher one-session eradication rate than conventional TL, with no increase in adverse reactions. The lower count of any-rebleeding events seen in adjusted logistic regression was not corroborated by time-to-event Cox analysis and should be regarded as a hypothesis-generating signal rather than a definitive treatment effect. Residual confounding by calendar time (treatment-by-era imbalance), single-operator experience, and unmeasured factors limits causal inference. These findings should therefore be interpreted as preliminary; confirmation in contemporaneous multicenter randomized studies is required before clinical superiority of MEVL can be inferred. Future research should also assess longer-term outcomes, recurrence risk, and cost-effectiveness.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261453281 – Supplemental material for Preliminary research on the effectiveness and safety of metal clip-assisted endoscopic variceal ligation in the treatment of gastric varices
Supplemental material, sj-docx-1-tag-10.1177_17562848261453281 for Preliminary research on the effectiveness and safety of metal clip-assisted endoscopic variceal ligation in the treatment of gastric varices by Wang Yi, Li Xiuling, Ding Hui, Li Zhenjuan, Li Jiaxin and Quan Runzhao in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank all patients and the participating healthcare providers for their time, consideration, and invaluable contribution to this research study.
Declarations
Generative AI disclosure
A locally downloaded open-source large language model, run entirely on the institutional computing hardware of Henan Provincial People’s Hospital, was used for language polishing of manuscript text and for checklist formatting. No patient-identifiable data, clinical records, raw datasets, analytical outputs, or manuscript text were uploaded to, shared with, or otherwise exposed to any external, cloud-based, or third-party AI service at any stage. All source data and all manuscript text remained within the institutional computing environment throughout the study. The AI model was not used to generate scientific content, clinical interpretation, statistical analyses, or conclusions. All analytical outputs were independently generated by the authors using SPSS 26 for baseline tests and Python 3.11 with statsmodels 0.14, lifelines 0.27, and scipy 1.11 for multivariable, survival, and post hoc power analyses; statistical code and computation were executed locally on institutional hardware, and results were verified by re-execution against source data. The authors take full responsibility for the integrity and accuracy of all content in the manuscript.
Reporting format
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.