
Abstract
Background and aims:
Endoscopic ultrasound-guided tissue acquisition (EUS-TA) is critical for diagnosing solid lesions. The wet-suction technique, which pre-fills the needle lumen with saline, has been proposed to improve specimen quality compared with conventional dry suction. This study aimed to evaluate the efficacy of wet suction versus dry suction in EUS-TA.
Objectives:
This study aimed to evaluate the efficacy of wet suction versus dry suction in EUS-TA.
Design:
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) following PRISMA 2020 guidelines.
Methods:
Electronic searches of PubMed, Embase, Cochrane CENTRAL, and additional databases were performed through January 2025. Primary outcomes were blood contamination, cellularity, and integrity scores; secondary outcomes were diagnostic accuracy and specimen adequacy. Effect sizes were calculated using Hedges’ g or risk ratios (RRs) with 95% confidence intervals (CIs).
Results:
Seven RCTs (784 patients; 1566 specimens) were included. Wet suction significantly reduced blood contamination (Hedges’ g = 0.289, 95% CI: 0.178–0.401, p < 0.0001) and improved cellularity (Hedges’ g = 0.420, 95% CI: 0.241–0.599, p < 0.0001) with low heterogeneity. Integrity score showed no significant difference (p = 0.054). Overall diagnostic accuracy was similar between techniques (RR = 1.025, p = 0.548), but subgroup analysis revealed higher accuracy for wet suction in EUS-fine needle aspiration (FNA; RR = 1.162, p = 0.001). Specimen adequacy did not differ significantly (p = 0.074).
Conclusion:
Wet suction improves sample quality by reducing blood contamination and increasing cellularity, with potential diagnostic benefit in FNA procedures. Effects on integrity and adequacy remain inconclusive. Larger, standardized trials are warranted to confirm these findings.
Plain language summary
Introduction
Endoscopic ultrasound (EUS) has become an indispensable diagnostic tool in gastrointestinal practice, particularly for detecting small lesions often missed by conventional imaging techniques. Through EUS-guided tissue acquisition (EUS-TA), clinicians can obtain real-time cytological or histological samples from tumors or suspicious lesions, enabling accurate pathological and molecular diagnoses. This approach plays a critical role in cancer staging, differentiating pancreatic diseases, and evaluating intra-abdominal lymphadenopathy, and is considered the gold standard for diagnosing pancreatic cancer and other solid tumors. 1
In recent years, advances in needle design and aspiration techniques have introduced the “wet suction” method to improve specimen quality and diagnostic accuracy. This technique involves pre-flushing the needle lumen with saline to replace the air column, thereby enhancing vacuum force transmission during aspiration, increasing tissue yield, and potentially reducing blood contamination.2,3 Specifically, the wet-suction technique removes the stylet from the biopsy needle and irrigates the lumen with 1–2 mL of saline before puncturing the lesion; suction is then applied using a 10 mL vacuum syringe.4,5 By reducing air interference and minimizing the risk of blood contamination, this method is hypothesized to improve tissue quality.
Despite these theoretical advantages, clinical evidence comparing wet suction with conventional dry suction remains inconclusive, particularly regarding key outcomes such as tissue integrity, diagnostic accuracy, and blood contamination. Furthermore, different strategies for EUS-TA—namely EUS-fine needle aspiration (FNA) versus EUS-fine needle biopsy (FNB)—may yield variable results.
Recently, the European Society of Gastrointestinal Endoscopy (ESGE) published an updated Technical and Technology Review on EUS-guided tissue sampling. The ESGE guidelines issue a strong recommendation for using equally the wet-suction or slow-pull techniques for EUS-FNB of pancreatic masses. This recommendation is based on evidence that these techniques provide high rates of adequate samples and tissue integrity while reducing specimen bloodiness compared to traditional dry suction. 6
To address these gaps, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the relative efficacy of wet suction versus dry suction in EUS-TA. Our goal is to provide clinically relevant evidence to guide endosonographers in selecting the most appropriate aspiration technique to optimize diagnostic yield and patient outcomes.
Materials and methods
Protocol and registration
This meta-analysis was conducted in accordance with the PRISMA 2020 guidelines (see Table S1). 7 The study protocol was registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) under the registration number INPLASY202580029 (DOI: 10.37766/inplasy2025.8.0029). Since no human participants were involved, ethics review board approval and participant informed consent were not required.
Search strategy and data collection
Two authors (P.-F.H. and H.-W.C.) made independent electronic searches in the PubMed, Embase, ClinicalKey, Cochrane CENTRAL, ProQuest, ScienceDirect, and Web of Science with keyword of (“endoscopic ultrasound” OR “fine needle aspiration” OR “FNA” OR “FNB” OR “dry-suction” OR “wet-suction”) AND (“pancreatic mass” OR “solid lesions”) through the earliest record up to January 31, 2025. In addition to including gray literature and unpublished data, we also performed an electronic search on the ClinicalTrials.gov platform. A detailed search strategy is provided in the Supplemental Material (Table S2).
In the initial stage, these two authors screened the titles and abstracts for eligibility through consensus. To expand the pool of potential studies, we scrutinized the reference lists of review articles4,8 –13 and performed further manual searches. Later, a third reviewer (Y.-T.K.) was consulted in situations in which the two authors could not achieve consensus. No language restrictions were imposed.
Eligibility criteria and outcomes
This meta-analysis followed the PICO framework (Population, Intervention, Comparison, Outcome) as outlined: P: patients referred for EUS-TA; I: Wet-suction technique; C: Dry-suction technique; O: Blood contamination score, cellularity score, integrity score, specimen adequacy, and diagnostic accuracy.
Inclusion criteria included: (1) RCTs involving human participants, (2) Trials comparing wet-suction with dry suction in EUS-TA, and (3) Studies providing data on tissue integrity score, blood contamination score, and specimen accuracy. Exclusion criteria were: (1) Non-RCT studies, (2) Studies lacking data on tissue integrity score, blood contamination score, or specimen accuracy, and (3) Studies with participant overlap from previously published trials.
Risk of bias and evidence quality
To investigate the methodological quality of the recruited studies, we used a version of the Cochrane risk-of-bias tool for randomized trials (RoB 2), which consists of six main items: randomization process, intervention adherence, missing outcome data, outcome measurement, selective reporting, and overall risk of bias. 14
In RoB 2’s intervention adherence section, one of the two options should be selected for literature assessment: intention-to-treat (intervention assignment) or per-protocol (intervention adherence). In this meta-analysis, we chose a per-protocol evaluation. Any discrepancy in the opinions of assessments between the two evaluators (P.-F.H. and H.-W.C.) was solved by the judgment of the third evaluator (Y.-T.K.).
Primary outcome: Evaluation of blood contamination, cellularity, and integrity scores
This study primarily evaluated in comparison of blood contamination, cellularity, and integrity scores in dry suction technique or wet suction technique.4,8 –13 The outcomes were measured using Hedges’ g score.
Secondary outcome: Evaluation of diagnostic accuracy and specimen adequacy
As a secondary outcome, this investigation also examined diagnostic accuracy and specimen adequacy. The outcomes were measured using risk ratios (RRs).
Data extraction and management
Data were extracted by the author from each study included in this meta-analysis, capturing demographic details, study design elements, and information on EUS-TA with both primary and secondary outcome values. To maintain accuracy, evaluators carefully verified the direction of effect for each scale used. When data were unavailable in published reports, corresponding authors were contacted for original data. Data extraction, transformation, and consolidation across study arms with differing strategies followed the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions and related medical literature. 15 When multiple post-treatment data points were available, we used the outcome reported at the intervention’s conclusion for statistical analysis. In crossover studies, only data from the initial study period were included to avoid carry-over effects. 16
While some of the included RCTs utilized a multi-arm design that evaluated additional tissue acquisition methods—such as the slow-pull or capillary techniques—our data extraction was restricted exclusively to the wet suction and dry suction arms. This approach was taken to directly address the primary objective of comparing these two specific aspiration techniques.
Statistical analysis
Given the variability of the target populations in the studies, we conducted this meta-analysis using a random-effects model with Comprehensive Meta-Analysis software (version 4; Biostat, Englewood, NJ, USA). 17 We used Hedges’ g with 95% confidence intervals (CIs) to measure primary outcomes (i.e., blood contamination score), interpreting Hedges’ g values of 0.2, 0.5, and 0.8 as small, moderate, and large effect sizes, respectively. 18 For secondary outcomes (i.e., accuracy), we assessed RRs with their 95% CIs. Study heterogeneity was evaluated using I2 and Cochran’s Q statistics, where I2 values of 25%, 50%, and 75% indicated low, moderate, and high heterogeneity, respectively. 19 We confirmed the meta-analysis’s robustness through sensitivity analyses using the one-study removal method. 20 Publication bias was assessed following Cochrane Handbook guidelines, and funnel plots were visually examined for asymmetry. 21
Results
Study selection and characteristics
Figure 1 shows the PRISMA flowchart outlining the literature search process. After removing duplicates and excluding non-relevant articles based on title and abstract screening, we ultimately included seven RCTs in the final analysis.4,8 –13 Table S3 lists articles excluded in the final stage, along with reasons for exclusion.22 –24 The 7 eligible RCTs comprised 1566 specimens, 784 participants, with a mean age of 60.50 ± 11.74 years, of whom 59.31% (n = 465) were male. Diagnoses among solid lesions, pancreatic, and non-pancreatic.4,8 –13 The details of these trials are summarized in Table 1.
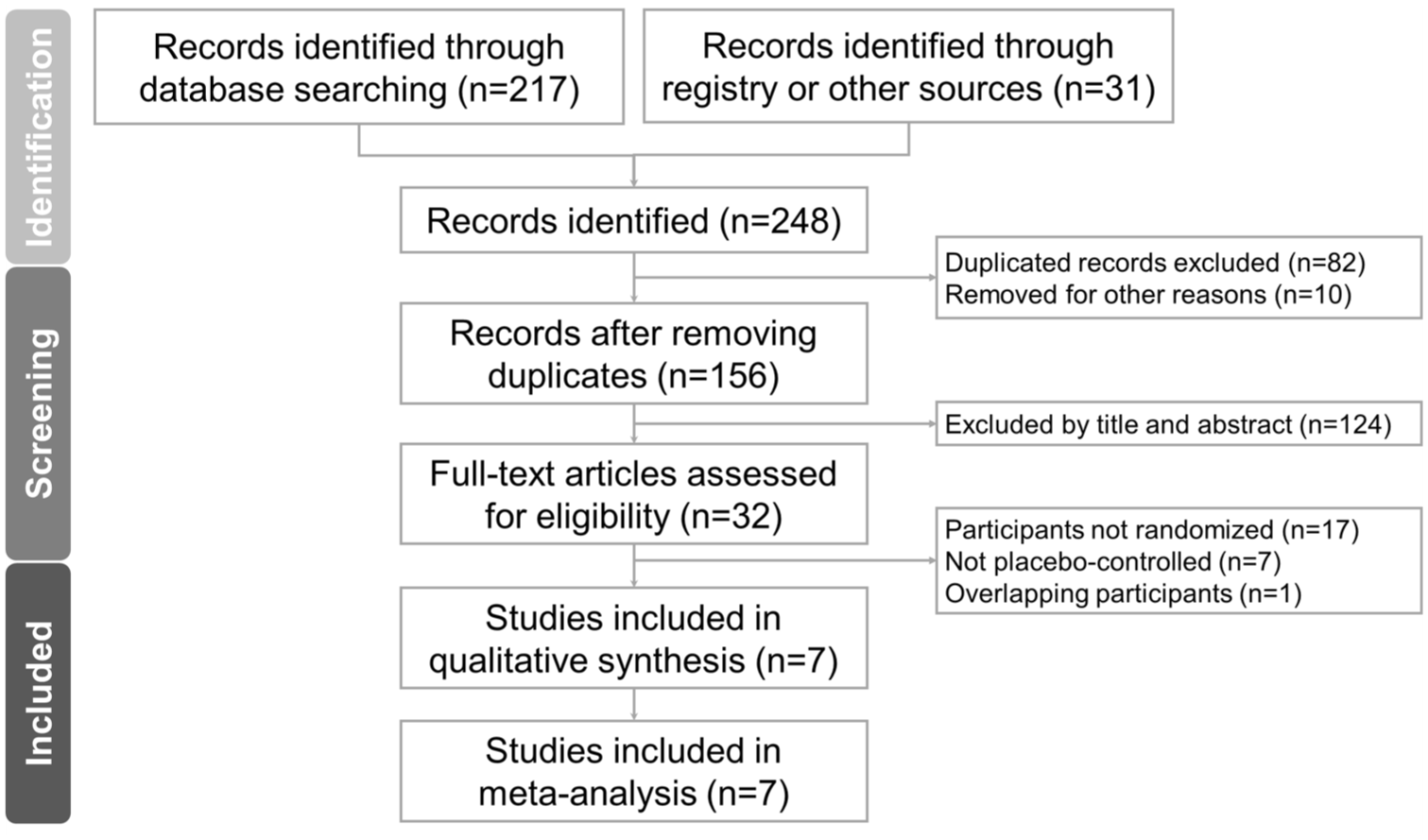
The PRISMA flowchart.
Summary of the retrieved trials investigating the effect of EUS tissue acquisition in the enrolled participants.
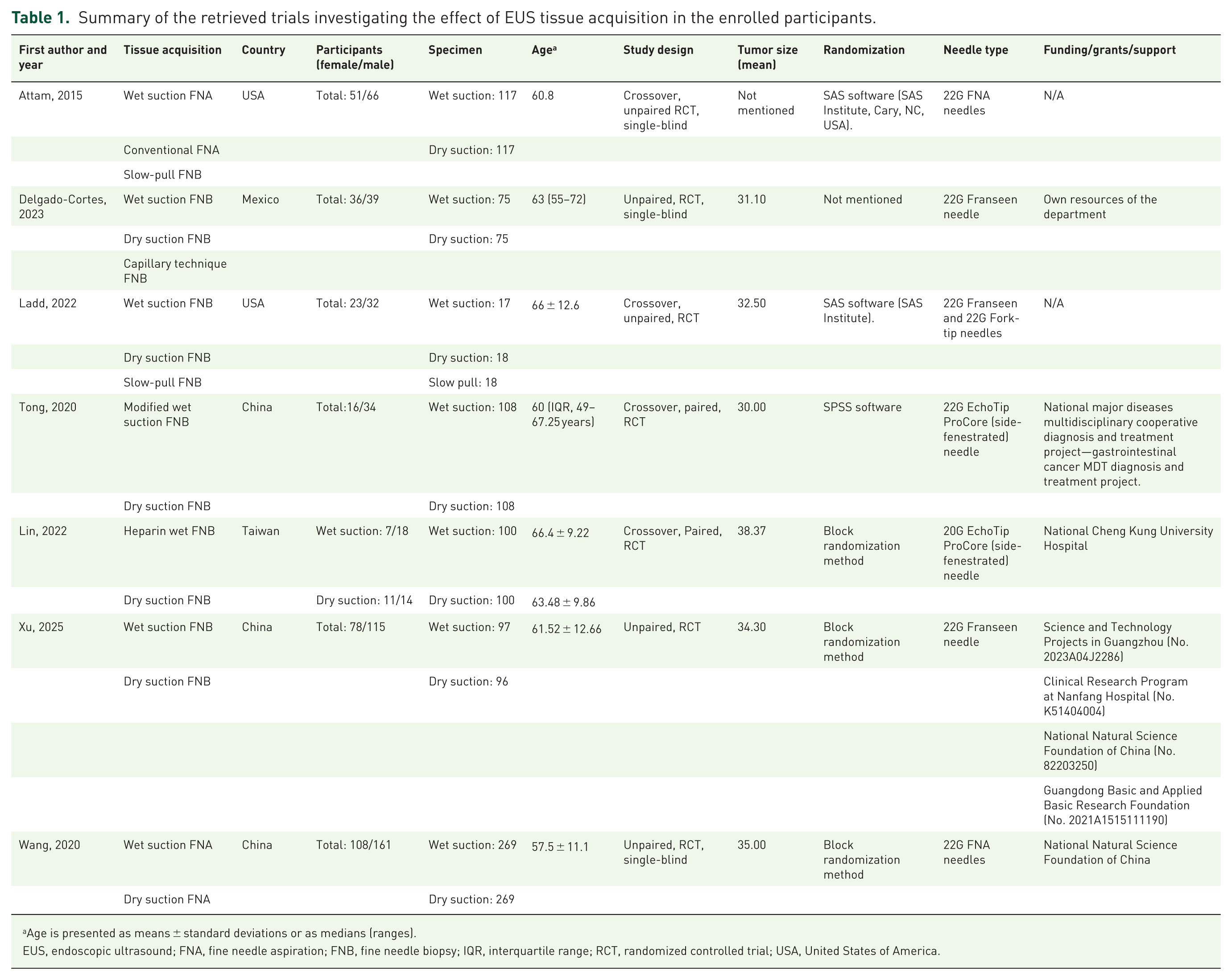
Age is presented as means ± standard deviations or as medians (ranges).
EUS, endoscopic ultrasound; FNA, fine needle aspiration; FNB, fine needle biopsy; IQR, interquartile range; RCT, randomized controlled trial; USA, United States of America.
Risk of bias and quality of evidence
In evaluating the overall methodological quality of the included studies, we found that 42.86% were rated as low risk of bias, 57.14% as having some risk of bias, and none as high risk of bias (Figure 2). More specifically, four studies were classified as having “some” risk of bias in the randomization process due to a lack of information on allocation concealment.8,9,12,13 The details of the risk of bias assessment are summarized in Table 2.
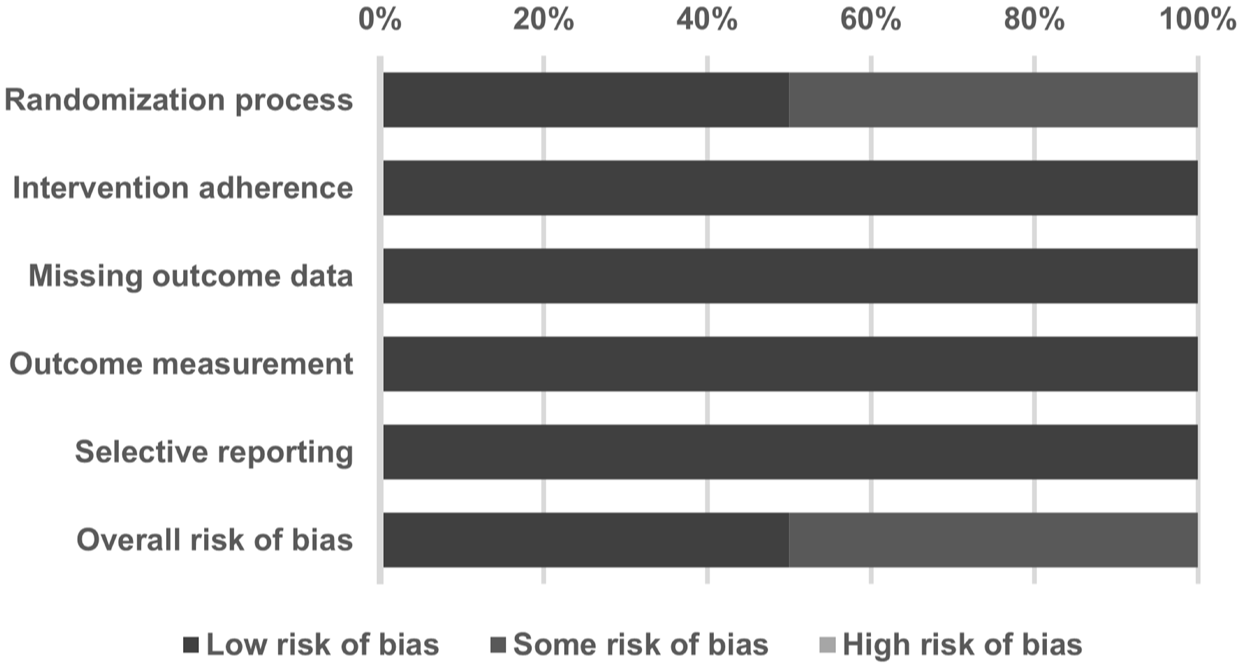
Summary of quality assessment of studies included in the meta-analysis using the Cochrane risk of bias 2 tool.
Detailed quality assessment of included studies using Cochrane risk of bias 2 tool.

The studies didn’t provide allocation concealment details.
L, low risk of bias; RoB, risk of bias; S, risk of bias.
Primary outcome: Evaluation of blood contamination, cellularity, and integrity scores
Blood contamination score
Seven studies were included for blood contamination score (Figure 3(a)). Wet suction significantly reduced blood contamination compared with dry suction, with a pooled Hedges’ g of 0.289 (95% CI: 0.178–0.401, p < 0.0001; I2 = 14.98%), indicating low heterogeneity. Sensitivity analysis demonstrated robust findings (Figure 3(b)). Meta-regression showed a slight positive association between mean lesion size and effect size (coefficient = 0.0093, p < 0.0001), suggesting a potential trend for larger lesions benefiting more from wet suction (Figure 3(c)).

(a) Forest plot comparing wet suction versus dry suction for blood contamination score. Effect sizes are expressed as Hedges’ g with 95% CIs. Positive values favor wet suction. The pooled effect size was 0.289 (95% CI: 0.178–0.401, p < 0.0001; I2 = 14.98%), indicating low heterogeneity and a significant reduction in blood contamination with wet suction. (b) Leave-one-out sensitivity analysis for blood contamination score, showing consistent pooled estimates after removing individual studies. (c) Bubble plot of meta-regression evaluating the association between mean lesion size (mm) and effect size (Hedges’ g) for blood contamination score. Circle sizes are proportional to study weights. The regression line indicates a slight positive association (coefficient = 0.0093, p < 0.0001).
Cellularity score
Three studies reported cellularity score (Figure 4(a)). Wet suction demonstrated a significant improvement in specimen cellularity compared with dry suction (Hedges’ g = 0.420, 95% CI: 0.241–0.599, p < 0.0001; I2 = 0%), indicating homogeneity across studies. Sensitivity analysis confirmed the stability of results (Figure 4(b)).
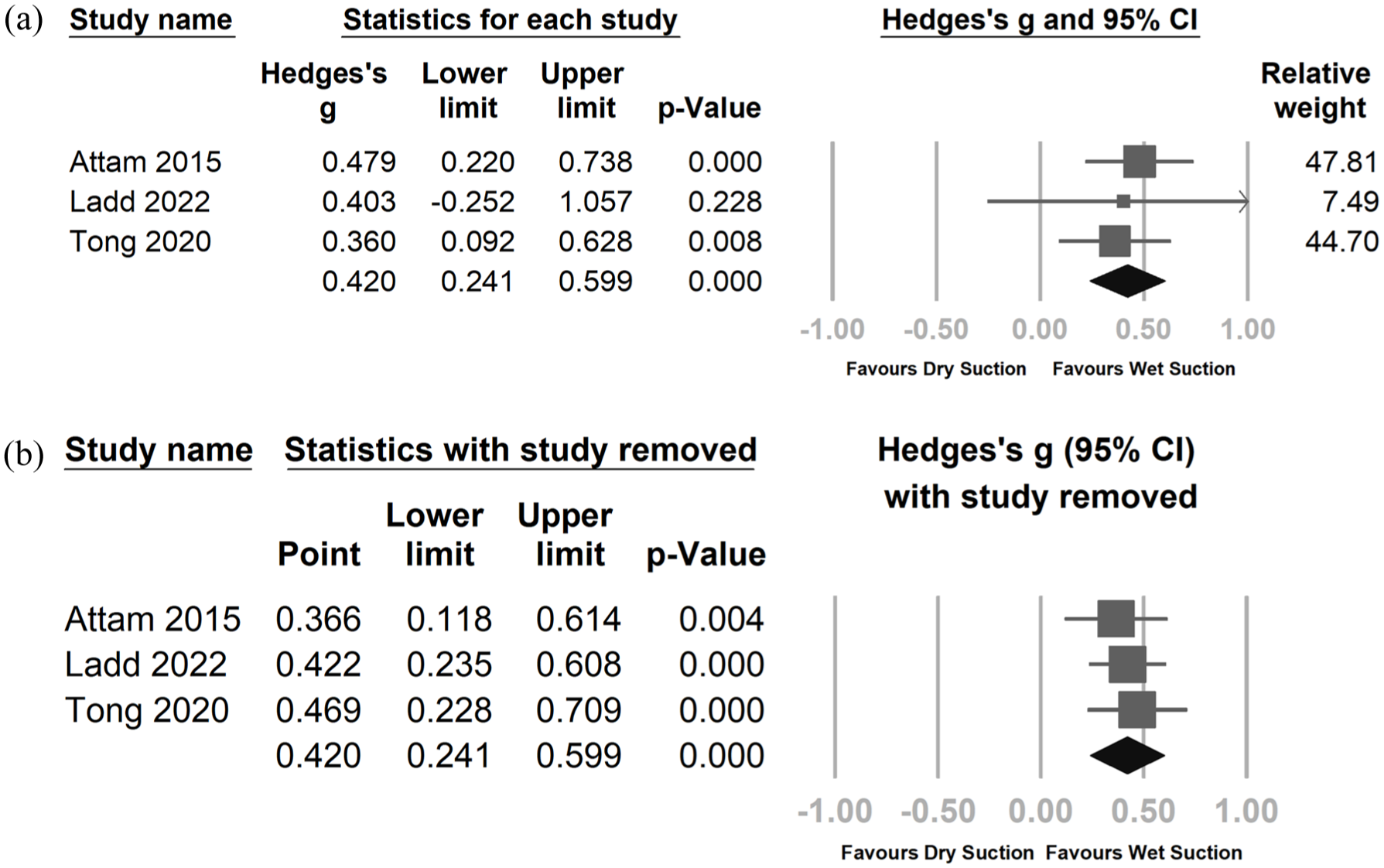
(a) Forest plot comparing wet suction versus dry suction for cellularity score. The pooled effect size was 0.420 (95% CI: 0.241–0.599, p < 0.0001; I2 = 0%), suggesting no heterogeneity and a significant improvement in cellularity with wet suction. (b) Leave-one-out sensitivity analysis for cellularity score, indicating robust results with minimal change in pooled effect estimates after removing individual studies.
Integrity score
Three studies assessed specimen integrity (Figure 5(a)). The pooled effect size was 0.198 (95% CI: −0.004 to 0.399, p = 0.054; I2 = 32.6%), suggesting moderate heterogeneity and no statistically significant difference between wet and dry suction. Sensitivity analysis indicated no single study had a substantial impact on the overall result (Figure 5(b)).
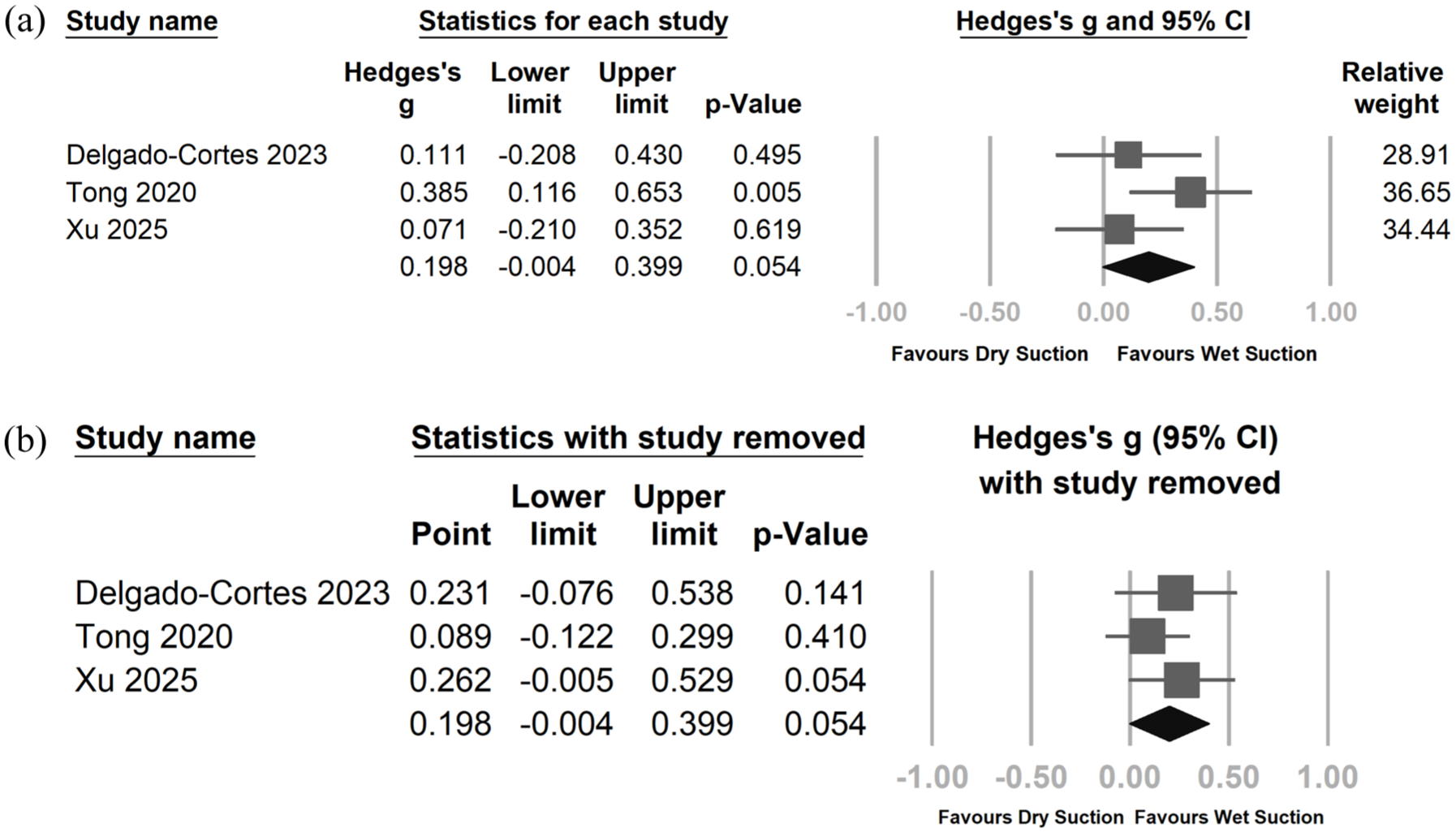
(a) Forest plot comparing wet suction versus dry suction for integrity score. The pooled effect size was 0.198 (95% CI: −0.004 to 0.399, p = 0.054; I2 = 32.6%), indicating moderate heterogeneity and no statistically significant difference between wet and dry suction. (b) Leave-one-out sensitivity analysis for integrity score, revealing stable findings across different scenarios, with all analyses remaining nonsignificant.
Secondary outcome: Evaluation of diagnostic accuracy and specimen adequacy
Diagnostic accuracy
Four studies evaluated diagnostic accuracy. No significant difference was observed overall (RR = 1.025, 95% CI: 0.945–1.112, p = 0.548; I2 = 0%). Subgroup analysis revealed a significant effect in the FNA subgroup (RR = 1.162, 95% CI: 1.065–1.269, p = 0.001), favoring wet suction, while no significant difference was seen in the FNB subgroup (Figure 6(a) and (b)).
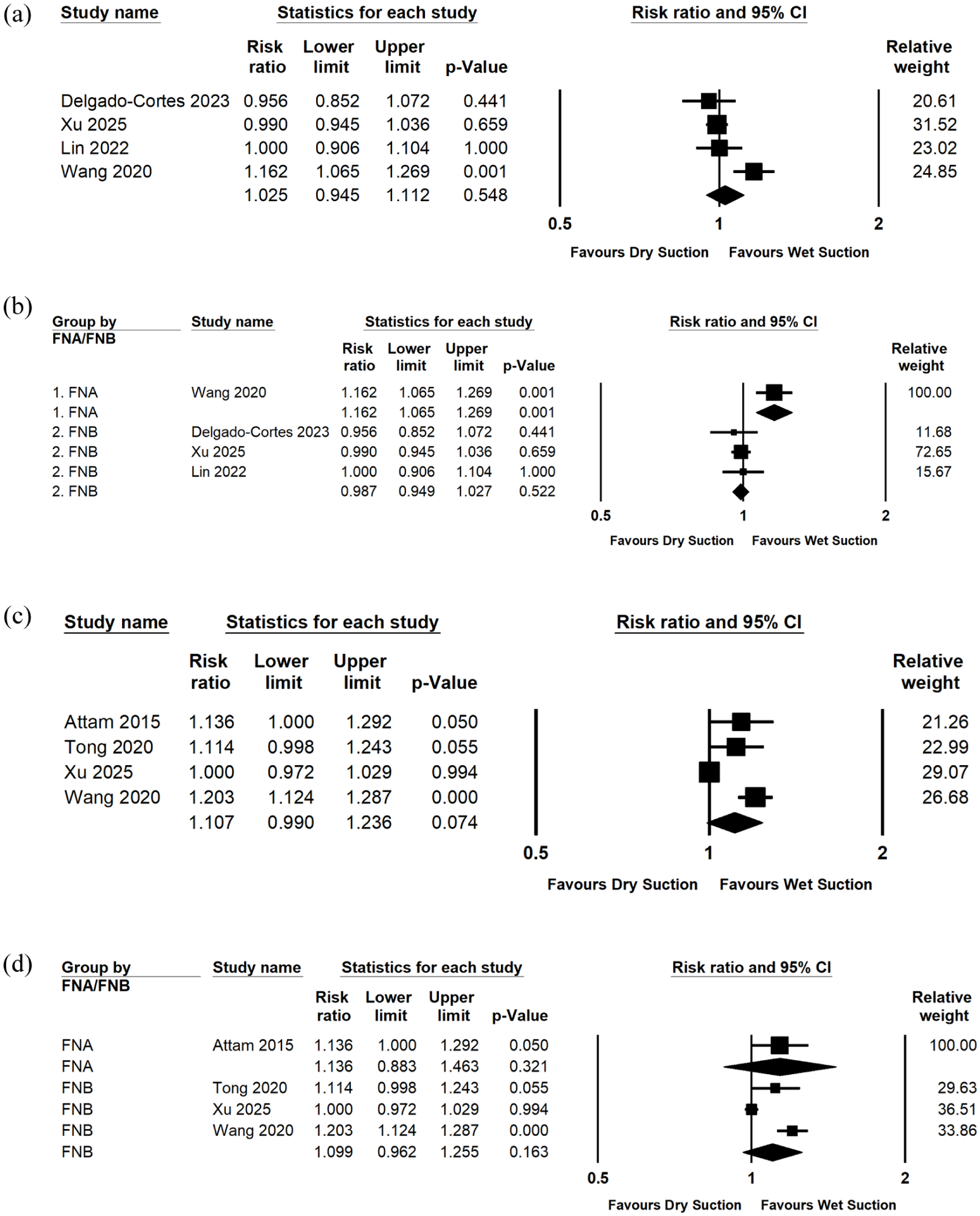
Forest plots comparing wet suction versus dry suction for diagnostic accuracy and specimen adequacy, including subgroup analyses by needle type. (a) Forest plot comparing wet suction versus dry suction for overall diagnostic accuracy. Effect sizes are expressed as RRs with 95% CIs. The pooled RR was 1.025 (95% CI: 0.945–1.112, p = 0.548; I2 = 0%), indicating no significant difference between wet and dry suction in overall diagnostic accuracy. (b) Subgroup analysis by needle type (FNA vs FNB) for diagnostic accuracy. Wet suction significantly improved diagnostic accuracy in the FNA subgroup (RR = 1.162, 95% CI: 1.065–1.269, p = 0.001), whereas no significant difference was observed in the FNB subgroup (all p > 0.05). (c) Forest plot comparing wet suction versus dry suction for specimen adequacy. Effect sizes are expressed as RR with 95% CIs. The pooled RR was 1.107 (95% CI: 0.990–1.236, p = 0.074; I2 = 89%), indicating high heterogeneity and no statistically significant overall difference between wet and dry suction. (d) Subgroup analysis by needle type (FNA vs FNB) for specimen adequacy. Wet suction showed a pooled RR of 1.136 (95% CI: 0.883–1.463, p = 0.321) for FNA and 1.099 (95% CI: 0.962–1.255, p = 0.163) for FNB, suggesting no significant difference in either subgroup, although one individual FNA study 12 demonstrated a marginally significant result (p = 0.050).
Specimen adequacy
Four studies assessed specimen adequacy. The pooled RR was 1.107 (95% CI: 0.990–1.236, p = 0.074; I2 = 89%), indicating substantial heterogeneity and no significant overall difference. Subgroup analysis showed no significant improvement for FNA (RR = 1.136, p = 0.321) or FNB (RR = 1.099, p = 0.163), though Attam 2015 (FNA) individually showed borderline significance (p = 0.050; Figure 6(c) and (d)).
Discussion
Principal findings
This meta-analysis demonstrates that wet suction offers significant advantages over dry suction in reducing blood contamination and improving specimen cellularity during EUS-TA. Specifically, wet suction significantly lowered blood contamination scores (Hedges’ g = 0.289) and enhanced cellularity (Hedges’ g = 0.420), with low to no heterogeneity observed in these outcomes. Sensitivity analyses confirmed the robustness of these findings. In addition, meta-regression indicated a positive correlation between lesion size and the magnitude of benefit for blood contamination, suggesting that larger lesions may derive greater advantage from wet suction.
In contrast, specimen integrity did not differ significantly between techniques, although a nonsignificant trend favoring wet suction was observed (p = 0.054). For diagnostic accuracy, the overall pooled effect showed no significant difference; however, subgroup analysis revealed that wet suction significantly improved diagnostic accuracy in FNA procedures, whereas no benefit was detected in FNB. Similarly, specimen adequacy did not significantly differ between groups, with substantial heterogeneity limiting interpretability, though one individual study showed borderline improvement with wet suction. 12
Overall, these findings suggest that wet suction primarily enhances sample quality by reducing blood contamination and increasing cellularity, with potential additional benefit for diagnostic accuracy in FNA procedures, while effects on integrity and adequacy remain inconclusive.
Mechanisms
In the wet-suction technique, the stylet is removed, and the needle is prefilled with 1–2 mL of saline prior to puncture, replacing the air column with fluid. Suction is subsequently applied using a 10 mL air vacuum syringe. This configuration improves vacuum force transmission, thereby enhancing tissue aspiration efficiency. Computational fluid dynamics modeling demonstrates that wet suction can aspirate approximately 5.6 times more tissue volume than dry suction, owing to reduced compressibility of the fluid-filled system. 5 Furthermore, this approach appears to lower blood contamination compared to simple suction. Excessive blood contamination can compromise histologic interpretation and reduce the reliability of diagnostic samples.
Implications for clinical practice and research
Previous studies have explored lesion- and technique-specific factors influencing the efficacy of wet-suction methods. Delgado-Cortés et al. 13 reported that lesions located in the pancreatic body or tail yielded significantly higher tissue integrity scores with wet suction (mean 4.40 ± 1.60, p = 0.027). 13 Similarly, Crino et al. 24 observed that while tissue core acquisition rates were comparable between wet suction and slow-pull techniques for pancreatic lesions (73.3% vs 67.1%), wet suction provided a significant advantage for nonpancreatic lesions (67.2% vs 48.4%, p = 0.032). This benefit may be particularly relevant in softer, less fibrotic tissues, such as lymph nodes and subepithelial tumors, which respond better to fluid-assisted suction and produce longer, more intact tissue cores.24,25
Adjunctive strategies, including heparin priming, have been proposed to further improve specimen quality. Diehl et al. 26 demonstrated that preflushing needles with heparinized saline can reduce blood contamination and clot formation, thereby enhancing tissue integrity and preserving DNA yield, which is critical for molecular analysis. Similar findings were reported by Lin et al., 10 who confirmed that heparin priming improves specimen quality and reduces fibrin clot formation. 25 Hybrid suction techniques—combining wet suction with continuous negative pressure—have also been developed to minimize variability in manual aspiration, maintain consistent suction force, and reduce friction within the needle lumen. 25
However, the choice of needle remains a key determinant of wet-suction performance. Reverse-bevel needles appear to synergize better with wet suction, while Franseen and fork-tip designs are reported to perform optimally with slow-pull techniques. 24 Despite these advantages, additional procedural steps such as preflushing and heparin priming introduce complexity and prolong procedure time. 27
Future research should focus on larger study populations and the standardization of wet-suction protocols. Key areas for investigation include optimizing saline and heparin volumes, defining appropriate suction pressures, and establishing uniform methodological guidelines. Such efforts will help refine wet-suction strategies and expand their diagnostic applications in EUS-FNA/B.
While our meta-analysis demonstrates that the wet-suction technique improves specimen quality and reduces blood contamination, cases of insufficient or non-diagnostic samples may still occur. From a clinical perspective, management strategies in such scenarios should be tailored to the patient’s condition and the characteristics of the lesion. Potential follow-up approaches include:
Repeat tissue acquisition: If the initial specimen quality is insufficient, a repeat EUS-TA may be performed, possibly applying optimization techniques such as wet suction to improve the diagnostic yield.
Additional imaging: Further evaluation with computed tomography or magnetic resonance imaging can help better characterize the lesion.
Alternative diagnostic methods: Surgical biopsy, laparoscopy, or relevant laboratory tests may be considered as complementary diagnostic approaches.
Referral to specialized centers: When diagnostic uncertainty remains, referral to a tertiary center or multidisciplinary expert consultation is recommended.
Observation and follow-up: For small, indeterminate, or low-risk lesions, short-term follow-up imaging may be an appropriate strategy to monitor morphological changes over time.
Strengths and limitations
The strengths of this review include a comprehensive literature search, inclusion of studies utilizing both FNA and FNB techniques, and consistent application of standardized outcome measures. Nonetheless, several limitations should be acknowledged. The number of eligible studies was relatively small, and heterogeneity in lesion types, suction protocols, and needle designs may limit the generalizability of findings. Further high-quality, randomized studies are warranted to confirm the observed benefits of wet suction and refine its optimal clinical use.
Although our meta-analysis evaluated various FNB needle designs—such as Franseen, fork-tip, and standard side-fenestrated needles—there remains a lack of data regarding the efficacy of the wet suction technique when using the new forward-bevel 20G side-fenestrated needle. 28 Future comparative studies evaluating optimal suction techniques for this specific novel needle design are warranted.
Relation to prior work
To the best of our knowledge, the most relevant prior evidence comes from a network meta-analysis that primarily focused on the integrity and adequacy of specimens obtained with FNB techniques. 29 Our study advances this field by including both FNA and FNB and limiting the analysis to RCTs, thereby strengthening the reliability of the evidence. In addition, we performed subgroup analyses comparing FNA and FNB, which revealed differential benefits of wet suction across needle types, offering a more nuanced understanding of its role in EUS-TA.
Conclusion
This systematic review and meta-analysis demonstrate that wet suction significantly reduces blood contamination and enhances specimen cellularity, with benefits most evident in FNA procedures. While both FNA and FNB appear to gain from wet suction, the effect is more pronounced in FNA. However, these findings should be interpreted with caution due to moderate-to-high heterogeneity in some outcomes and the limited number of included studies. Future research should involve large-scale randomized trials and investigate refinements to wet-suction protocols, including variations in fluid type, volume, and suction pressure, to optimize their diagnostic utility.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261458692 – Supplemental material for Impact of wet suction on specimen quality and diagnostic accuracy in EUS-guided tissue acquisition: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-tag-10.1177_17562848261458692 for Impact of wet suction on specimen quality and diagnostic accuracy in EUS-guided tissue acquisition: a systematic review and meta-analysis of randomized controlled trials by Po-Feng Huang, Jung-Chun Lin, Tien-Yu Huang, Peng-Jen Chen, Chi-Wei Yang, Yu-Ting Kuo and Hsuan-Wei Chen in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
None.
Declarations
Disclosure of AI use in manuscript preparation
The author(s) used the AI platform Gemini (developed by Google) to improve the language and readability of the manuscript during the drafting process. The AI was used for grammatical corrections and stylistic refinement. After using this tool, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the final content of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.